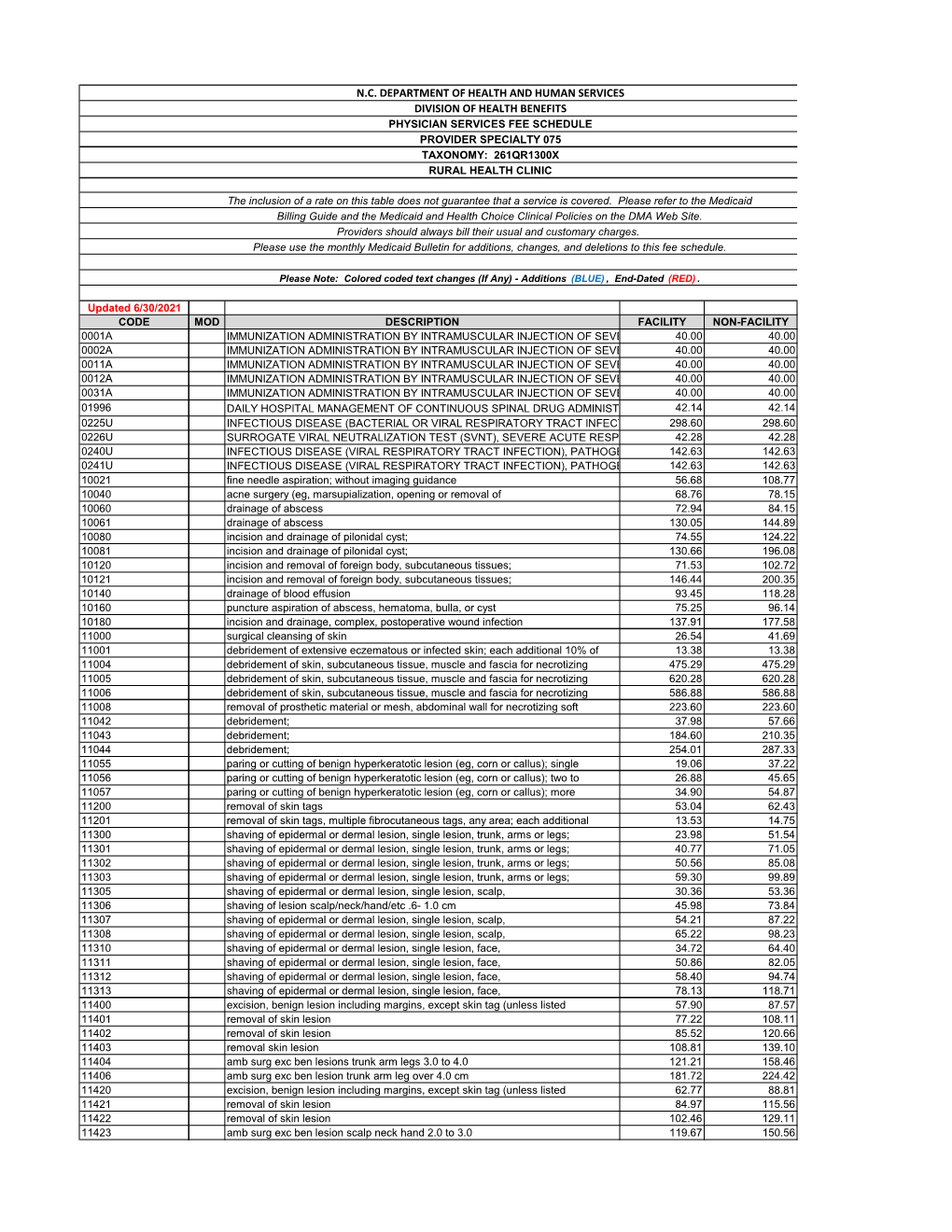
Rural Health Clinic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Decompressive Craniectomy Following Severe Traumatic Brain Injury with an Initial Glasgow Coma Scale Score of 3 Or 4
Case Report Clinics in Surgery Published: 03 Jul, 2019 Decompressive Craniectomy Following Severe Traumatic Brain Injury with an Initial Glasgow Coma Scale Score of 3 or 4 Afif AFIF* Department of Neurosurgery and Anatomy, Pierre Wertheimer Hospital, France Abstract Background: Decompressive craniectomy is a surgical management option for severe Traumatic Brain Injury (TBI). However, few studies have followed patients with TBI who have a Glasgow Coma Scale (GCS) score of 3 or 4 (out of 15). Decompressive craniectomy has been avoided in such patients owing to poor outcomes and poor functional recoveries in previous cases of treatment using this method. Clinical Presentation: Two patients are presented in our case series. The first suffered severe TBI following an aggression, with a GCS score of 3 and bilaterally dilated unreactive pupils. Brains CT scan showed right frontal fracture, bifrontal hematoma contusion, a fronto-temporo-parietal acute Subdural Hematoma (SDH) with a thickness of 14 mm on the right side, traumatic subarachnoid hemorrhage, with 20 mm of midline shift to the left side, and diffuses brain edema. The second presented with severe TBI following an automobile accident, with a GCS score of 4 and iso- reactive pupils. A brain CT scan showed bilateral fronto-temporal fracture, diffuse brain hematoma contusion, traumatic subarachnoid hemorrhage, right Extradural Hematoma (EDH) and bilateral fronto-temporo-parietal acute SDH that was more pronounced on the right side. Conclusion: Follow-up after the operations showed an Extended Glasgow Outcome Scale (EGOS) score of 8 and a very good functional recovery for both patients. Our case series suggests that in patients with severe TBI and a GCS score of 3 or 4; decompressive craniectomy can be performed OPEN ACCESS with good long-term neurological outcomes. -

Cranioplasty: Indications, Procedures, and Outcome – an Institutional Experience Syed M
OPEN ACCESS Editor: James I. Ausman, MD, PhD For entire Editorial Board visit : University of California, Los http://www.surgicalneurologyint.com Angeles, CA, USA SNI: General Neurosurgery Original Article Cranioplasty: Indications, procedures, and outcome – An institutional experience Syed M. Andrabi, Arif H. Sarmast, Altaf R. Kirmani, Abdul R. Bhat Department of Neurosurgery, Sher I Kashmir Institute of Medical Sciences, Srinagar, Jammu and Kashmir, India E‑mail: Syed M. Andrabi ‑ [email protected]; *Arif H. Sarmast ‑ [email protected]; Altaf R. Kirmani ‑ [email protected]; Abdul R. Bhat ‑ [email protected] *Corresponding author Received: 27 January 17 Accepted: 16 March 17 Published: 26 May 17 Abstract Background: Cranioplasty, the repair of a skull vault defect by insertion of an object (bone or nonbiological materials such as metal or plastic plates), is a well‑known procedure in modern neurosurgery. Brain protection and cosmetic aspects are the major indications of cranioplasty. A retroprospective study was conducted for evaluating the indications, materials used, complications, and outcome of cranioplasty. Methods: This study was prospective from August 2013 to September 2015 and retrospective from August 2010 to July 2013. In the retrospective study, patients files were retrieved from the mentioned date (August 2010 to July 2013) from the medical records and the findings were recorded. Abstracted data included age at the time of cranioplasty (years), sex (male or female), medical comorbidities (hypertension, -

Case Series Sinking Skin Flap Syndrome Following Posttraumatic Hydrocephalus
Hindawi Case Reports in Neurological Medicine Volume 2021, Article ID 6682310, 8 pages https://doi.org/10.1155/2021/6682310 Case Series Sinking Skin Flap Syndrome following Posttraumatic Hydrocephalus Ashish Chugh, Prashant Punia , and Sarang Gotecha Dr. D. Y. Patil Medical College and Hospital, Pimpri, Pune, Maharashtra, India Correspondence should be addressed to Prashant Punia; [email protected] Received 21 November 2020; Revised 8 January 2021; Accepted 11 January 2021; Published 9 February 2021 Academic Editor: Tapas Kumar Banerjee Copyright © 2021 Ashish Chugh et al. (is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Introduction. Complications following craniotomy are not uncommon and Sinking Skin Flap Syndrome (SSFS) constitutes a rare entity that may present after a large Decompressive Craniectomy. Although the entity is widely reported, the literature mostly consists of case reports. Authors present a case series of three patients with review of literature highlighting the various factors which can prove therapeutic and can help in avoidance of complications. Materials and Methods. (e study was conducted over a period of 3 years, from 2016 to 2019, and included 212 patients who underwent unilateral Decompressive Craniectomy (DC) for trauma in our institute. All 212 patients underwent a similar DC following a strict institutional protocol and the craniectomies were performed by the same surgical team. At total of 160 patients survived and elective cranioplasty was planned at a 3-month interval. Out of a total of 160 patients who survived, 38 developed hydrocephalus, 3 patients presented with hydrocephalus acutely and had to be shunted before cranioplasty and underwent ventriculoperitoneal (VP) shunting on the opposite side of craniectomy. -

Partial Nephrectomy for Renal Cancer: Part I
REVIEW ARTICLE Partial nephrectomy for renal cancer: Part I BJUIBJU INTERNATIONAL Paul Russo Department of Surgery, Urology Service, and Weill Medical College, Cornell University, Memorial Sloan Kettering Cancer Center, New York, NY, USA INTRODUCTION The Problem of Kidney Cancer Kidney Cancer Is The Third Most Common Genitourinary Tumour With 57 760 New Cases And 12 980 Deaths Expected In 2009 [1]. There Are Currently Two Distinct Groups Of Patients With Kidney Cancer. The First Consists Of The Symptomatic, Large, Locally Advanced Tumours Often Presenting With Regional Adenopathy, Adrenal Invasion, And Extension Into The Renal Vein Or Inferior Vena Cava. Despite Radical Nephrectomy (Rn) In Conjunction With Regional Lymphadenectomy And Adrenalectomy, Progression To Distant Metastasis And Death From Disease Occurs In ≈30% Of These Patients. For Patients Presenting With Isolated Metastatic Disease, Metastasectomy In Carefully Selected Patients Has Been Associated With Long-term Survival [2]. For Patients With Diffuse Metastatic Disease And An Acceptable Performance Status, Cytoreductive Nephrectomy Might Add Several Additional Months Of Survival, As Opposed To Cytokine Therapy Alone, And Prepare Patients For Integrated Treatment, Now In Neoadjuvant And Adjuvant Clinical Trials, With The New Multitargeted Tyrosine Kinase Inhibitors (Sunitinib, Sorafenib) And Mtor Inhibitors (Temsirolimus, Everolimus) [3,4]. The second groups of patients with kidney overall survival. The explanation for this cancer are those with small renal tumours observation is not clear and could indicate (median tumour size <4 cm, T1a), often that aggressive surgical treatment of small incidentally discovered in asymptomatic renal masses in patients not in imminent patients during danger did not counterbalance a population imaging for of patients with increasingly virulent larger nonspecific abdominal tumours. -

Core Neurosurgery
BAYLOR SCOTT & WHITE TEXAS SPINE & JOINT HOSPITAL NEUROLOGICAL SURGERY CLINICAL PRIVILEGES NAME: ________________________________ Initial appointment Reappointment All new applicants must meet the following requirements as approved by the governing body. To be eligible to apply for core privileges in neurological surgery, the initial applicant must meet the following criteria: Successful completion of ACGME or American Osteopathic Association accredited residency in neurological surgery. Required previous experience: Applicants for initial appointment must be able to demonstrate the performance of at least 50 neurological surgical procedures, reflective of the scope of privileges requested, during the last 12 months or demonstrate successful completion of residency or fellowship within the past 12 months. Reappointment requirements: To be eligible to renew core privileges in Neurological Surgery, the applicant must meet the following maintenance of privilege criteria: Current demonstrated competence and an adequate volume of neurological surgery procedures with acceptable results, reflective of the scope of privileges requested, for the past 24 months based on results of ongoing professional practice evaluation and outcomes. Evidence of current ability to perform privileges requested is required of all applicants for renewal of privileges NEUROLOGICAL SURGERY CORE PRIVILEGES Requested: Admit, evaluate, diagnose, consult and provide nonoperative and pre-, intran, and postoperative care to patients of all ages presenting with injuries -

Neurosurgery
KALEIDA HEALTH Name ____________________________________ Date _____________ DELINEATION OF PRIVILEGES - NEUROSURGERY All members of the Department of Neurosurgery at Kaleida Health must have the following credentials: 1. Successful completion of an ACGME accredited Residency, Royal College of Physicians and Surgeons of Canada, or an ACGME equivalent Neurosurgery Residency Program. 2. Members of the clinical service of Neurosurgery must, within five (5) years of appointment to staff, achieve board certification in Neurosurgery. *Maintenance of board certification is mandatory for all providers who have achieved this status* Level 1 (core) privileges are those able to be performed after successful completion of an accredited Neurosurgery Residency program. The removal or restriction of these privileges would require further investigation as to the individual’s overall ability to practice, but there is no need to delineate these privileges individually. PLEASE NOTE: Please check the box for each privilege requested. Do not use an arrow or line to make selections. We will return applications that ignore this directive. LEVEL I (CORE) PRIVILEGES Basic Procedures including: Admission and Follow-Up Repair cranial or dural defect or lesion History and Physical for diagnosis and treatment plan* Seizure Chest tube placement Sterotactic framed localization of lesion Debride wound Sterotactic frameless localization Endotracheal intubation Transsphenoidal surgery of pituitary lesion Excision of foreign body Trauma Insertion of percutaneous arterial -

Reversible Signal Abnormalities in the Hippocampus and Neocortex After Prolonged Seizures
Reversible Signal Abnormalities in the Hippocampus and Neocortex after Prolonged Seizures Stephen Chan, Steven S. M. Chin, Krishnan Kartha, Douglas R. Nordli, Robert R. Goodman, Timothy A. Pedley, and Sadek K. Hilal PURPOSE: To investigate the phenomenon of reversible increased signal intensity of medial temporal lobe structures and cerebral neocortex seen on MR images of six patients with recent prolonged seizure activity. METHODS: After excluding patients with known causes of reversible signal abnormalities (such as hypertensive encephalopathy), we retrospectively reviewed the clinical findings and MR studies of six patients whose MR studies showed reversible signal abnor- malities. MR pulse sequences included T2-weighted spin-echo coronal views or conventional short-tau inversion-recovery coronal images of the temporal lobes. RESULTS: All six MR studies showed increased signal intensity within the medial temporal lobe, including the hippocampus in five studies. All follow-up MR examinations showed partial or complete resolution of the hyperin- tensity within the medial temporal lobe and the neocortex. In one patient, results of a brain biopsy revealed severe cerebral cortical gliosis. Temporal lobectomy performed 4 years later showed moderate cortical gliosis and nonspecific hippocampal cell loss and gliosis. CONCLUSION: Sig- nificant hyperintensity within the temporal lobe is demonstrable on MR images after prolonged seizure activity, suggestive of seizure-induced edema or gliosis. Damage to medial temporal lobe structures by prolonged seizure activity indicates a possible mechanism of epileptogenic disorders. Index terms: Brain, magnetic resonance; Brain, temporal lobe; Hippocampus; Seizures AJNR Am J Neuroradiol 17:1725–1731, October 1996 Prolonged seizure activity is associated with character of the acute neuronal loss in the hip- long-lasting neurologic damage and even death pocampus seen after an episode of status epi- in humans (1–3); prompt treatment is required lepticus is different from the neuronal loss and to forestall irreversible changes (4). -
Wrvus: Do They Really Measure the Workload and Complexity of What We Do?
wRVUs: Do They Really Measure the Workload and Complexity Of What We Do? Raj S. Pruthi MD MHA FACS Rhodes Distinguished Professor and Chair Department of Urology The University of North Carolina at Chapel Hill INTRODUCTION Productivity-based Compensation • InCreasing use of wRVU in employed Compensation models • 2007 (16%) à 2016 (> 60%) • Use of benChmarked data (MGMA, AMGA, SC) to determine compensation/produCtivity ($/wRVU) • e.g. AMGA $441,836 / 7649 = $57.76/wRVU 2 INTRODUCTION wRVU • RBRVS - Developed for HCFA by Hsaio et al (1986-92) • Passed in 1989 -- implemented in 1992 INTRODUCTION Work RVU x Work GPCI + Practice Expense RVU x PE GPCI Conversion Payment = x FaCtor Rate + Malpractice RVU x MP GPCI GPCI = geographiC praCtiCe Cost index INTRODUCTION • RVUs à metric of physician productivity • RVUs : CPT code 405 urologiCal serviCes 22 383 Work = Time x Intensity INTRODUCTION Work 100 units INTRODUCTION • RVU assignments initially made in consultation with nominees from various medical specialties • Quarterly adjustments based on survey data • Zero sum game INTRODUCTION Changes to Work RVUs RUC Summary of Recommendation INTRODUCTION Who Gets Surveys? • Respondents seleCted by AUA by random sampling • May be sub-speCialty, e.g. prosthetiCs • May be general, e.g. cysto with dilation • Private praCtiCe (small & large), hospital-based, and aCademiC • Need at least 30-50 responses -- ideally >100 responses INTRODUCTION • Subjective methodology linked with compensation • Accurate measure of surgical complexity? workload? effort? time? -

ICD~10~PCS Complete Code Set Procedural Coding System Sample
ICD~10~PCS Complete Code Set Procedural Coding System Sample Table.of.Contents Preface....................................................................................00 Mouth and Throat ............................................................................. 00 Introducton...........................................................................00 Gastrointestinal System .................................................................. 00 Hepatobiliary System and Pancreas ........................................... 00 What is ICD-10-PCS? ........................................................................ 00 Endocrine System ............................................................................. 00 ICD-10-PCS Code Structure ........................................................... 00 Skin and Breast .................................................................................. 00 ICD-10-PCS Design ........................................................................... 00 Subcutaneous Tissue and Fascia ................................................. 00 ICD-10-PCS Additional Characteristics ...................................... 00 Muscles ................................................................................................. 00 ICD-10-PCS Applications ................................................................ 00 Tendons ................................................................................................ 00 Understandng.Root.Operatons..........................................00 -

Infection on Neurological Implanted Devices
ECCMID Amsterdam 09.04.2016 Challenging complex infections for ID physicians Infection on neurological implanted devices Anna Conen, MD MSc Deputy Head Physician Division of Infectious Diseases and Hospital Hygiene ESCMIDKantonsspital Aarau, eLibrary Switzerland by author Disclosures Received travel grants from Gilead, Merck Sharp Dohme, ViiV Healthcare, Bristol- Myers Squibb and Janssen. ESCMID eLibrary by author Outline • Diagnosis of implant-associated infections • Treatment concepts of implant-associated infections • Specific infections associated with the following implants: Craniotomy/bone flap Cranioplasty Deep brain stimulator Ventriculo-peritoneal shunt Neurological implants ESCMIDSpinal cord stimulator External ventricular eLibrary drainage Ventriculo-atrial shunt by author Risk of implant-associated infections Device No. inserted in the US, Infection rate, % per year Fracture fixation devices 2,000,000 5–10 Dental implants 1,000,000 5–10 Joint prostheses 600,000 1–3 Neurosurgical implants 450,000 3–15 Cardiac pacemakers 300,000 1–7 Mammary implants 130,000 1–2 Mechanical heart valves 85,000 1–3 Penile implants 15,000 1–3 Heart assist devices 700 25–50 ESCMID eLibraryDarouiche RO. Clin Infect Dis 2011; 33:1567-1572 by author Concept and diagnosis of biofilm Biofilm Sonication - Bacteria adhere to implant - Sonication of implants*: surface detachment of biofilm - Embed in a matrix - Sonication fluid plated on - In stationary growth phase culture media - Slowly replicate Standard method: 3 Sonication of tissue biopsies implant: Sensitivity ~60% Sensitivity 80-90% *Cranioplasty, shunts, screws, plates, stimulators, etc. Zimmerli W. J Infect Dis. 1982;146(4):487-97. Trampuz A. NEJM 2007;357:654–663. Portillo M. J Clin Microbiol 2015;53(5):1622-7. -

Urology Scientific Session Monday, September 28, 2020
Urology Scientific Session Monday, September 28, 2020 Moderators/Panelists: Drs. Sabine Zundel, Sameh Shehata, Holger Till, Yuri Kozlov, Philipp Szavay, Eduardo Perez (S26) PNEUMOVESICOSCOPIC CORRECTION OF PRIMARY VESICOURETERAL REFLUX (VUR) IN CHILDREN. - OUR INITIAL EXPERIENCE- A. M. Benaired, Pediatric, Surgeon; H Zahaf, Pediatric, Surgeon; Military Central Hospital Purpose: Vesicoureteral reflux is a common urological abnormality predisposing risk of childhood hypertension and chronic renal failure. It is called primitive when it is due to an abnormality of the vesicoureteral junction. Different treatment approaches have been proposed a long time. Two main trends can be identified, conservative and operative approach. The main objective of our prospective study is to demonstrate the feasibility of vesicoscopic crosstrigonal ureteral reimplantation under CO2 pneumovesicum in treatment on primary vesicoureteral reflux and analyze results of this approach. Methods: A total of 60 patients underwent transvesicoscopic ureteral reimplantation (33 boys, 27 girls) by the same surgeon from Mai 2011 to Mai 2015. All patients had primary vesicoureteral reflux, and surgery was performed because of breakthrough urinary tract infection despite antibiotic prophylaxis, persistent high grade of vesicoureteral reflux especially in association with significant renal scarring, mean age at operation was 47.47 month (5 month - 12 years). Of the 60 patients, 34 had bilateral reflux and 26 had unilateral reflux. The reflux grade in the total of 94 ureters was grade IV, V in 59.57%, grade III in 35.11% and grade II in 5.32% in association with contralateral high grade vesicoureteral reflux. Our surgical methods followed those reported by Valla et al. Results: The transvesicoscopic procedure was successfully completed in all patients without perioperative complication except one case of pneumoperitoneum that required exsufflation by open laparoscopy. -

Laparoscopic Ureteral Repair in Gynaecological Surgery Carlo De Ciccoa, Anastasia Ussiab and Philippe Robert Koninckxb,C
Laparoscopic ureteral repair in gynaecological surgery Carlo De Ciccoa, Anastasia Ussiab and Philippe Robert Koninckxb,c aDepartment of Obstetrics and Gynaecology, Purpose of review University Hospital A. Gemelli, Universita` Cattolica del Sacro Cuore, bGruppo Italo-Belga, Rome, Italy and To review laparoscopic surgery in the treatment options for ureteral lesions in cDepartment of Obstetrics and Gynaecology, gynaecological surgery. University Hospital Gasthuisberg, Katholieke Recent findings Universiteit Leuven, Leuven, Belgium Laparoscopic treatment of ureteral injuries has been increasingly reported over the past Correspondence to Dr Carlo De Cicco, Department of Obstetrics and Gynaecology, University Hospital A. years. Treatment has progressively shifted from ureteroneocystostomy performed by Gemelli, Universita` Cattolica del Sacro Cuore, Largo F. laparotomy to less invasive treatment options such as ureteral stenting or dilatation in Vito 1, 00168 Rome, Italy Tel: +39 06 30155131; case of stricture, stenting under laparoscopic guidance and laparoscopic stitching of e-mail: [email protected] lacerations, laparoscopic ureteral reanastomosis or laparoscopic Current Opinion in Obstetrics and Gynecology ureteroneocystostomy for transections. Deep endometriosis surgery of an associated 2011, 23:296–300 hydronephrosis is associated with a high incidence of ureteral lesions making preoperative stenting desirable in order to facilitate the eventual repair, while avoiding the more problematic insertion of a stent after a lesion is made. The available data confirm the excellent outcome of stenting obstructive lesions. When stenting proves difficult or in case of a ureteral leakage, laparoscopic aided stenting is strongly suggested, in order to avoid further damage while permitting simultaneous repair if necessary. Laparoscopic suturing of a laceration over a stent is clearly superior to stenting only.