Populated Printable COP 2009 Botswana Generated 9/28/2009 12:01:26 AM
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Scramble for Land Between the Barokologadi Community and Hermannsburg Missionaries
The Scramble for Land between the Barokologadi Community and Hermannsburg Missionaries Victor MS Molobi https://orcid.org/0000-0001-7824-1048 University of South Africa [email protected] Abstract This article investigates the land claim of the Barokologadi of Melorane, with their long history of disadvantages in the land of their forefathers. The sources of such disadvantages are traceable way back to tribal wars (known as “difaqane”) in South Africa. At first, people were forced to retreat temporarily to a safer site when the wars were in progress. On their return, the Hermannsburg missionaries came to serve in Melorane, benefiting from the land provided by the Kgosi. Later the government of the time expropriated that land. What was the significance of this land? The experience of Melorane was not necessarily unique; it was actually a common practice aimed at acquiring land from rural communities. This article is an attempt to present the facts of that event. There were, however, later interruptions, such as when the Hermannsburg Mission Church became part of the Evangelical Lutheran Church of Southern Africa (ELCSA). Keywords: land claim; church land; Barokologadi; missionary movement; Hermannsburg; Melorane; Lutheran Introduction Melorane is the area that includes the southern part of Madikwe Game Park in the North West Province, with the village situated inside the park. The community of Melorane is known as the Barokologadi of Maotwe, which was forcibly removed in 1950. Morokologadi is a porcupine, which is a totem of the Barokologadi community. The community received their land back on 6 July 2007 through the National Department of Land Affairs. -

Invitation to Register
INVITATION TO REGISTER Botswana Tourism Organisation (BTO) is a parastatal body set up through an Act of Parliament with the Mandate to: market and promote Botswana as a tourist destination of choice; promote investment in the tourism sector; as well as to grade and classify tourism facilities BTO has Nine (9) Satellite Offices and Information Offices throughout the country in Maun, Tsabong, Ghanzi, Kang, Kasane, Francistown, Selibe Phikwe, Palapye, Letlhakane and the Head Office in Gaborone. Further, BTO operationally supports Four (4) Community Projects being the Tsabong Camel Park, Seboba Cultural Village in Kasane, Goo Moremi Gorge and Resort and Lepokole. BTO is on a drive to enhance efficiency, competitiveness and transparency as well as create opportunity in the supply and delivery of goods and services by locally registered suppliers, hence the invitation to be considered for accreditation and listing in the supplier database for an initial minimum period of Two (2) years. BTO therefore wishes to invite interested, capable and committed suppliers to register for listing of the following goods and services; The interested suppliers are required to register and collect application forms from any of the BTO offices in Gaborone, Tsabong, Kang, Ghanzi, Maun, Kasane, Francistown, Selibe – Phikwe, Palapye and Letlhakane. Tented Accommodation Safaris Catering & Conferencing Travel & Transportation Event Management & Stage setup Printing Services Maintenance (Air-conditioners, Plumbing, Electrical, carpentry Branding & Signage IT Hardware -

IVIV VV VI Pretoria Pretoria Soweto Soweto 0 125 250 Kmiv IV V V VV V
Earthquake Green Shaking Alert M 6.5, Botswana Origin Time: Mon 2017-04-03 17:40:16 UTC (19:40:16 local) PAGER o o Location: 22.62 S 25.15 E Depth: 11 km Version 1 Created: 40 minutes, 53 seconds after earthquake Estimated Fatalities Green alert for shaking-related fatalities Estimated Economic Losses and economic losses. There is a low likelihood of casualties and damage. 65% 50% 30% 32% 15% 4% 3% 1 100 10,000 1 100 10,000 10 1,000 100,000 10 1,000 100,000 Fatalities USD (Millions) Estimated Population Exposed to Earthquake Shaking ESTIMATED POPULATION - -* 3,776k* 19,253k* 2,733k 54k 2k 0 0 0 EXPOSURE (k = x1000) ESTIMATED MODIFIED MERCALLI INTENSITY PERCEIVED SHAKING Not felt Weak Light Moderate Strong Very Strong Severe Violent Extreme Resistant none none none V. Light Light Moderate Moderate/Heavy Heavy V. Heavy POTENTIAL Structures DAMAGE Vulnerable Structures none none none Light Moderate Moderate/Heavy Heavy V. Heavy V. Heavy *Estimated exposure only includes population within the map area. Population Exposure population per ~1 sq. km from Landscan Structures: Overall, the population in this region resides in structures that are vulnerable to IV 21°E ShakaweShakaweShakawe 24°E HwangeHwange27°E earthquake shaking, though some resistant PandamatengaPandamatengaPandamatenga DeteDete structures exist. LupaneLupaneLupane Historical Earthquakes (with MMI levels): There were no earthquakes with significant NokanengNokaneng InyathiInyathiInyathi ShanganiShanganiShangani population exposure to shaking within a 400 MaunMaun MaunMaun SuaSuaSua -

HIV/AIDS Beh Dukw Haviour Wi Refug Ral Surv Gee Cam Veillanc
HIV/AIDS Behavioural Surveillance Survey (BSS) Dukwi Refugee Camp, Botswana May 2013 UNHCR & Botswana Ministry of Health 1 Acknowledgements The 2012 Botswana Behavioural Surveillance Survey (BSS) was a joint effort of UNHCR and the Botswana Ministry of Health, with funding from UNAIDS and WHO, and the support of Botswana Red Cross Society. The BSS was initiated and coordinated by Ms. Marian Schilperoord of UNHCR Geneva, and Dr. Njogu Patterson of UNHCR Pretoria, whose depth of experience overseeing similar surveys was incredibly valuable. Dr. Emmanuel Baingana of UNAIDS and Dr. Eugene Nyarko of WHO lent invaluable advice and support during critical phases of the project, and we are exceptionally grateful. The investigation team was led by the Principal Investigator Ms. Aimee Rose who managed the adaptation of the protocol and tools, field work, analysis and reporting. Dr. Marina Anderson, Co‐ Principal Investigator from the Ministry of Health, provided excellent technical oversight and coordination with the Ministry of Health. Three Investigators from the Ministry of Health, Ms. Lumba Nchunga, Ms. Betty Orapeleng and Ms. Bene Ntwayagae, provided input in each phase of the survey, from protocol development, pre‐planning missions to Dukwi Camp, monitoring of training and field work, and report compilation. The team benefitted from the dedicated support of UNHCR Country Representative Lynn Ngugi. We give special appreciation to UNHCR Program Officer Galefele Beleme for her tireless work on recruiting, finance, and logistics, and numerous other issues. UNHCR Head of Field Office Jane Okello facilitated the survey’s success at Dukwi Camp, with superb assistance from UNHCR staff Niroj Shrestha, Gracias Atwine, and Onkemetse Leburu. -

Botswana Environment Statistics Water Digest 2018
Botswana Environment Statistics Water Digest 2018 Private Bag 0024 Gaborone TOLL FREE NUMBER: 0800600200 Tel: ( +267) 367 1300 Fax: ( +267) 395 2201 E-mail: [email protected] Website: http://www.statsbots.org.bw Published by STATISTICS BOTSWANA Private Bag 0024, Gaborone Phone: 3671300 Fax: 3952201 Email: [email protected] Website: www.statsbots.org.bw Contact Unit: Environment Statistics Unit Phone: 367 1300 ISBN: 978-99968-482-3-0 (e-book) Copyright © Statistics Botswana 2020 No part of this information shall be reproduced, stored in a Retrieval system, or even transmitted in any form or by any means, whether electronically, mechanically, photocopying or otherwise, without the prior permission of Statistics Botswana. BOTSWANA ENVIRONMENT STATISTICS WATER DIGEST 2018 Statistics Botswana PREFACE This is Statistics Botswana’s annual Botswana Environment Statistics: Water Digest. It is the first solely water statistics annual digest. This Digest will provide data for use by decision-makers in water management and development and provide tools for the monitoring of trends in water statistics. The indicators in this report cover data on dam levels, water production, billed water consumption, non-revenue water, and water supplied to mines. It is envisaged that coverage of indicators will be expanded as more data becomes available. International standards and guidelines were followed in the compilation of this report. The United Nations Framework for the Development of Environment Statistics (UNFDES) and the United Nations International Recommendations for Water Statistics were particularly useful guidelines. The data collected herein will feed into the UN System of Environmental Economic Accounting (SEEA) for water and hence facilitate an informed management of water resources. -
Questions 1. Mr. Dl Keorapetse
BOTSWANA NATIONAL ASSEMBLY O R D E R P A P E R (WEDNESDAY 3RD FEBRUARY, 2016) QUESTIONS 1. MR. D. L. KEORAPETSE, MP. (SELEBI PHIKWE WEST): To ask the (187) Minister of Minerals, Energy and Water Resources:- (i) how often electricity and water meters should be serviced; (ii) whether Botswana Power Corporation (BPC) and Water Utilities Corporation (WUC) allow consumers to service electricity and water meters themselves; if not, (iii) how often BPC and WUC service the said meters; and (iv) who, in the absence of electricity and water regulators, independently receives and investigates consumer complaints about malfunctioning and/or suspect electricity and water meters. 2. MR. N. M. NGAKA, MP. (TAKATOKWANE): To ask the Minister of (188) Health if she is aware that Motokwe, Khekhenye and Tsetseng Health Posts are not in either Kgalagadi or Kweneng Districts’ staff houses building lists; if so:- (i) why and which of the two lists are they supposed to be in; (ii) how many houses are the three (3) health posts mentioned above allocated; and (iii) whether this omission is not a sign that the three (3) health posts should be serviced by Kweneng and not Kgalagadi as it was the case before. 3. MR. A. S. KESUPILE, MP. (KANYE SOUTH): To ask the Minister of (189) Agriculture:- (i) if he is aware that Lobutse is a well organised community that needs regular visits by the agriculture officer to advise on a host of issues regarding the use of their fields and to resolve with their involvement the long standing issue of a drift fence; if so, (ii) to explain why the agriculture officers are not regular enough to the satisfaction of the farmers; and (iii) when Lobutse community will be assisted to put up the drift fence. -

Ÿþm I C R O S O F T W O R
E WL E WL REGISTERED WITH THE DIRECTOR OF POSTS AND TELEGRAPHS AS A NEWSPAPER Volume V No. 7 Organ of the Botswana Democratic Party JULY, 1967. LOETO LA TONA YA 'TEMO MO dikgweding tse di fitileng Tona ya Temo, Morena Tsheko T~sheko o ne a tsamaya thata mo mafelong a mantsi a Botswana, go bona balemi le barua-kgomo le go bona ditiro tsa ba Lephata la Temo le ba Lephata la Leruo. Mo mafelong otihe o ne a ntse a buisanya le babusi le magosi le merafe mo kgotleng le balemi ba basweu le ba bantsho. Me go itumedisa thata go bolela gore mo mafelong otlhe a a a tsamaileng pula e nele sentle mabele a teng le phulo e ntsi. Tota mo mafelong a mangwe pula e nele go feta selekanyo mo ebileng e ntshofaditse mabele ya bodisa dinawa le dithotse. Puo e o neng a e bua le batho bogolo e ne e le ya go ba kgothatsa go lema thata go katolosa masimo le go a epa disana le gore batho ba dire mo masimong a bone ngwaga otlhe eseng go ntsha dijo mo masismo go tswa foo batho ba bo ba siela kwa magaeng a matona goya go nna ba sa dire sepe. 0 ne a tlhalosa ka gore Goromente o lemoga gore temo le leruo mo Bot.swana ke tsone tse di tshetsang batho ka go sena mekoti le ditiro. Me a bolela ka gore Goromente o aga sekwele se segolo kwa Gaborone se se tla rutang makau a Botswana temo le tlhokomelo ya leruo gore ba gasiwe le lefatshe la Botswana go ruta batho ka bontsi go lema mo go tla ba tswelang molemo. -
List of Examination Centres by Region Bobirwa Region Centr Name Addres Place Phone 0101 Bobonong Primary School P.O
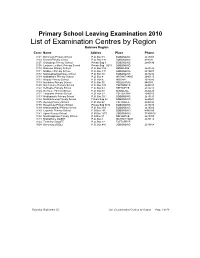
Primary School Leaving Examination 2010 List of Examination Centres by Region Bobirwa Region Centr Name Addres Place Phone 0101 Bobonong Primary School P.O. Box 48 BOBONONG 2619207 0103 Borotsi Primary School P.O. Box 136 BOBONONG 819208 0107 Gobojango Primary School Private Bag 8 BOBONONG 2645436 0108 Lentswe-Le-Moriti Primary School Private Bag 0019 BOBONONG 0110 Mabolwe Primary School P.O. Box 182 SEMOLALE 2645422 0111 Madikwe Primary School P.O. Box 131 BOBONONG 2619221 0112 Mafetsakgang primary school P.O. Box 46 BOBONONG 2619232 0114 Mathathane Primary School P.O. Box 4 MATHATHANE 2645110 0117 Mogapi Primary School P.O. Box 6 MOGAPI 2618545 0119 Molalatau Primary School P.O. Box 50 MOLALATAU 845374 0120 Moletemane Primary School P.O. Box 176 TSETSEBYE 2646035 0123 Sefhophe Primary School P.O. Box 41 SEFHOPHE 2618210 0124 Semolale Primary School P.O. Box 10 SEMOLALE 2645422 0131 Tsetsejwe Primary School P.O. Box 33 TSETSEJWE 2646103 0133 Modisaotsile Primary School P.O. Box 591 BOBONONG 2619123 0134 Motlhabaneng Primary School Private Bag 20 BOBONONG 2645541 0135 Busang Primary School P.O. Box 47 TSETSEBJE 2646144 0138 Rasetimela Primary School Private Bag 0014 BOBONONG 2619485 0139 Mabumahibidu Primary School P.O. Box 168 BOBONONG 2619040 0140 Lepokole Primary School P O Box 148 BOBONONG 4900035 0141 Agosi Primary School P O Box 1673 BOBONONG 71868614 0142 Motsholapheko Primary School P O Box 37 SEFHOPHE 2618305 0143 Mathathane DOSET P.O. Box 4 MATHATHANE 2645110 0144 Tsetsebye DOSET P.O. Box 33 TSETSEBYE 3024 Bobonong DOSET P.O. Box 483 BOBONONG 2619164 Saturday, September 25, List of Examination Centres by Region Page 1 of 39 Boteti Region Centr Name Addres Place Phone 0201 Adult Education Private Bag 1 ORAPA 0202 Baipidi Primary School P.O. -

Part. 4.2 (Fin.) FOURTH MEETING of the CONFERENCE of THE
Part. 4.2 (Fin.) FOURTH MEETING OF THE CONFERENCE OF THE PARTIES CUARTA REUNION DE LA CONFERENCIA DE LAS PARTES QUATRIEME SESSION DE LA CONFERENCE DES PARTIES Gaborone (Botswana) 19 to 30 April 1983 Gaborone (Botswana) 19 a1 30 de abril 1983 Gaborone (Botswana) 19 au 30 avril 1983 LIST OF PARTICIPANTS LISTA DE PARTICIPANTES LISTE DES PARTICIPANTS OBSERVERS/OBSERVADORES/OBSERVATEURS UNITED NATIONS ENVIRONMENT PROGRAMME /PROGRAMA DE LAS NACIONES UNIDAS PARA EL MEDIO AMBIENTE/PROGRAMME DES NATIONS UNIES POUR L'ENVIRONNEMENT Mona BJORKLUND Mostafa K. TOLBA Environmental Management Service United Nations Environment United Nations Environment Programme Programme P.O. Box 30552 P.O. Box 30552 Nairobi Nairobi Kenya Kenya A.T. BROUGH Fund Management Branch United Nations Environment Programme P.O. Box 30552 Nairobi Kenya FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS/ORGANIZACION DE LAS NACIONES UNIDAS PARA LA AGRICULTURA Y LA ALIMENTACION/ORGANISATION DES NATIONS UNIES POUR L'AGRICULTURE ET L'ALIMENTATION G.S. CHILD Forestry Resources Division FAO Via delle Terme di Caracalla I-00100 Roma Italy INTERNATIONAL CRIMINAL POLICE ORGANIZATION/ORGANIZATION INTERNACIONAL DE POLICIA CRIMINAL/ORGANISATION INTERNATIONALE DE POLICE CRIMINELLE Kesera KARUNATILLEKE General Secretariat ICPO- INTERPOL 26, rue Armengaud F-92210 Saint Cloud France 1203 EUROPEAN ECONOMIC COMMUNITY/COMUNIDAD ECONOMICA EUROPEA/COMMUNAUTE ECONOMIQUE EUROPEENNE Guy CORCELLE Claus STUFFMANN 170, rue de la Loi 200, rue de la Loi B-1049 Bruxelles B-1049 Bruxelles Belgique Belgique Auke HAAGSMA Willem WIJNSTEKERS 200, rue de la Loi 200, rue de la Loi B-1049 Bruxelles B-1049 Bruxelles Belgique Belgique ANTIGUA AND BARBUDA/ANTIGUA Y BARBUDA/ANTIGUA-ET-BARBUDA Richard BARON 70 North East 96th Street Miami Shores Florida 33161 U.S.A. -

2017 SEAT Report Orapa, Letlhakane and Damtshaa Mines
SEAT 3 REPORT Debswana - Orapa, Letlhakane and Damtshaa Mine (OLDM) November 2017 1 2 FOREWORD rounded assessment of the socio-economic impacts of our operation – positive and negative - in our zone of influence. This is the second impact assessment of this nature being conducted, the first one having been carried out in 2014. The information in this socio-economic assessment report helped to improve our understanding of the local dynamics associated with the impact our operation’s that are real and perceived. It also provided us with invaluable insight into our stakeholders’ perspectives, expectations, concerns and suggestions. This report is a valuable tool to guide our thinking on community development and our management of the social impacts of OLDM’s future closure at the end of the life of mine. Furthermore, it provides a useful mechanism in mobilising local stakeholders to work with us towards successful mine closure. The report has also given valuable feedback on issues around mine expansion initiatives and access to resources like land and groundwater. More importantly, meaningful feedback has been provided around two critical areas: resettlement and options around town transformation. We recognise the complexity of a proper plan for future mine closure at the end of the life of mine. In the past, our plans for future mine closure mainly focused on environmental aspects, with community involvement often limited to cursory consultation processes. Today, in line with current trends, my team and I are convinced that community ownership of the post closure goals is the only sustainable means to propel communities to prosper when OLDM is no longer involved. -

Refundable Fee of P280.00 (Two Hundred and Eighty Pula Only) VAT Inclusive
PUBLIC TENDER NOTICE TENDER NO: BOCRA/PT/006/2020.2021 SUPPLY, INSTALLATION AND COMMISSIONING OF ICT EQUIPMENT AT TWELVE (12) TRIBAL ADMINISTRATIONS IN KWENENG DISTRICT The Botswana Communications Regulatory Authority (BOCRA or the Authority) hereby invites experienced and reputable companies to tender for the Supply, Installation and Commissioning of ICT Equipment at twelve (12) Tribal Administrations in Kweneng District. The tender is reserved for 100% citizen-owned companies who are registered with the Public Procurement and Asset Disposal Board (PPADB) under the following codes and subcodes; Code 203: Electrical, Electronic, Mechanical and ICT Supplies Subcode 01: Electrical and Electronic Equipment, Spares and Accessories (includes ICT, photographic equipment, and others). Youth owned companies in Botswana shall purchase the ITT at 50% of the purchase price as per Presidential Directive CAB 14 (B)/2015. The Invitation to Tender (ITT) document may be purchased at the BOCRA Head Office by interested companies at a non-refundable fee of P280.00 (Two Hundred and Eighty Pula Only) VAT inclusive. Payment must be made in the form of bank transfer or deposits to the following bank details: Bank Name: First National Bank Botswana Ltd Branch Name: Mall Branch Code: 28-28-67 Account Name: Botswana Communications Regulatory Authority Bank Account No: 62011115088 Swift Code: FIRNBWGX Reference: BTA0001 Tender documents shall be issued upon provision of Proof of Payment (POP). All funds transfer bank charges shall be borne by the bidder. Compulsory -

BABBLER 2008 Babbler No
ISSN 1012 - 2974 JanuaryBABBLER 2008 Babbler No. 50 BABBLER Journal of BirdLife Botswana Journal of BirdLife Botswana BABBLER No. 50 January 2008 No. BABBLER The sincere thanks of all the members of BirdLife Botswana go to Remi and Wendy Borello who have once again generously supported the printing of this issue of the Babbler. Cover Design by Impression House Journal of Birdlife Botswana 1 Printing by Impression House Number 50 January 2008 Babbler No. 50 January 2008 BIRDLIFE BOTSWANA Partnership with the Private Sector: Conservation Corporation Africa (CCA Africa) BirdLife Botswana is a member of IUCN, the World Conservation Union. Founded in 1948, the World Conservation Union brings together States, government agencies and non-governmental Guests to Africa’s beatiful wilderness areas want to do more than simple tick organisations in a unique world partnership: almost 900 members off the Big Five. Birding is in, and CC Africa recognises this phenomenon as in all, spread across some 138 countries. a largely untapped experience for our guests - especially those who consider As a union, IUCN seeks to influence, encourage and assist themselves birding beginners. Star Bird is CC Africa’s new must-do safari societies throughout the world to conserve the integrity and experience! diversity of nature and to ensure that any use of natural resources is equitable and ecologically sustainable. With between 300 and 450 bird species in each of the 20 game areas in which CC Africa operates, aspirant birders are frequently overwhelmed by the sheer The World Conservation Union builds on the strength of its diversity of Africa.