Bitemedicine.Com/Watch
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

PATHOLOGY of the RENAL SYSTEM”, I Hope You Guys Like It
ﺑﺴﻢ اﷲ اﻟﺮﺣﻤﻦ اﻟﺮﺣﯿﻢ ھﺬه اﻟﻤﺬﻛﺮة ﻋﺒﺎرة ﻋﻦ إﻋﺎدة ﺗﻨﺴﯿﻖ وإﺿﺎﻓﺔ ﻧﻮﺗﺎت وﻣﻮاﺿﯿﻊ ﻟﻤﺬﻛﺮة زﻣﻼﺋﻨﺎ ﻣﻦ اﻟﺪﻓﻌﺔ اﻟﺴﺎﺑﻘﺔ ٤٢٧ اﻷﻋﺰاء.. ﻟﺘﺘﻮاﻓﻖ ﻣﻊ اﻟﻤﻨﮭﺞ اﻟﻤﻘﺮر ﻣﻦ اﻟﻘﺴﻢ ﺣﺮﺻﻨﺎ ﻓﯿﮭﺎ ﻋﻠﻰ إﻋﺎدة ﺻﯿﺎﻏﺔ ﻛﺜﯿﺮ ﻣﻦ اﻟﺠﻤﻞ ﻟﺘﻜﻮن ﺳﮭﻠﺔ اﻟﻔﮭﻢ وﺳﻠﺴﺔ إن ﺷﺎء اﷲ.. وﺿﻔﻨﺎ ﺑﻌﺾ اﻟﻨﻮﺗﺎت اﻟﻤﮭﻤﺔ وأﺿﻔﻨﺎ ﻣﻮاﺿﯿﻊ ﻣﻮﺟﻮدة ﺑﺎﻟـ curriculum ﺗﻌﺪﯾﻞ ٤٢٨ ﻋﻠﻰ اﻟﻤﺬﻛﺮة ﺑﻮاﺳﻄﺔ اﺧﻮاﻧﻜﻢ: ﻓﺎرس اﻟﻌﺒﺪي ﺑﻼل ﻣﺮوة ﻣﺤﻤﺪ اﻟﺼﻮﯾﺎن أﺣﻤﺪ اﻟﺴﯿﺪ ﺣﺴﻦ اﻟﻌﻨﺰي ﻧﺘﻤﻨﻰ ﻣﻨﮭﺎ اﻟﻔﺎﺋﺪة ﻗﺪر اﻟﻤﺴﺘﻄﺎع، وﻻ ﺗﻨﺴﻮﻧﺎ ﻣﻦ دﻋﻮاﺗﻜﻢ ! 2 After hours, or maybe days, of working hard, WE “THE PATHOLOGY TEAM” are proud to present “PATHOLOGY OF THE RENAL SYSTEM”, I hope you guys like it . Plz give us your prayers. Credits: 1st part = written by Assem “ THe AWesOme” KAlAnTAn revised by A.Z.K 2nd part = written by TMA revised by A.Z.K د.ﺧﺎﻟﺪ اﻟﻘﺮﻧﻲ 3rd part = written by Abo Malik revised by 4th part = written by A.Z.K revised by Assem “ THe AWesOme” KAlAnTAn 5th part = written by The Dude revised by TMA figures were provided by A.Z.K Page styling and figure embedding by: If u find any error, or u want to share any idea then plz, feel free to msg me [email protected] 3 Table of Contents Topic page THE NEPHROTIC SYNDROME 4 Minimal Change Disease 5 MEMBRANOUS GLOMERULONEPHRITIS 7 FOCAL SEGMENTAL GLOMERULOSCLEROSIS 9 MEMBRANOPROLIFERATIVE GLOMERULONEPHRITIS 11 DIABETIC NEPHROPATHY (new) 14 NEPHRITIC SYNDROME 18 Acute Post-infectious GN 19 IgA Nephropathy (Berger Disease) 20 Crescentic GN 22 Chronic GN 24 SLE Nephropathy (new) 26 Allograft rejection of the transplanted kidney (new) 27 Urinary Tract OBSTRUCTION, 28 RENAL STONES 23 HYDRONEPHROSIS -

PDI Appendix G Intermediate-Risk Immunocompromised State Ef Ec2
AHRQ QI™ ICD‐10‐CM/PCS Specification Enhanced Version 5.0 1 of 6 Pediatric Quality Indicators Appendices www.qualityindicators.ahrq.gov Pediatric Quality Indicators Appendices APPENDIX G: Intermediate-Risk Immunocompromised State Diagnosis Codes Intermediate-risk immunocompromised state diagnosis codes: (IMMUITD) ICD-9-CM Description ICD-10-CM Description 07022 VIRAL HEPATITIS B W HEPATIC COMA, CHRONIC WO B180 Chronic viral hepatitis B with delta‐agent MENTION OF HEPATITIS DELTA 07023 VIRAL HEPATITIS B W HEPACTIC COMA, CHRONIC W B181 Chronic viral hepatitis B without delta‐agent HEPATITIS DELTA 07044 CHRONIC HEPATITIS C WITH HEPACTIC COMMA B182 Chronic viral hepatitis C 2894 HYPERSPLENISM B520 Plasmodium malariae malaria with nephropathy 28950 DISEASE OF SPLEEN NOS D5702 Hb‐SS disease with splenic sequestration 28951 CHRONIC DIGESTIVE SPLENOMEGALY D57212 Sickle‐cell/Hb‐C disease with splenic sequestration 28952 SPLENIC SEQUESTRATION D57412 Sickle‐cell thalassemia with splenic sequestration 28959 OTHER DISEASE OF SPLEEN, OTHER D57812 Other sickle‐cell disorders with splenic sequestration 4560 ESOPHAGEAL VARICES W BLEEDING D730 Hyposplenism 4561 ESOPHAGEAL VARICES WO MENTION OF BLEEDING D731 Hypersplenism 45620 ESOPHAGEAL VARICES IN DISEASE CLASSIFIED D732 Chronic congestive splenomegaly ELSEWHERE, W BLEEDING 45621 ESOPHAGEAL VARICES IN DISEASE CLASSIFIED D733 Abscess of spleen ELSEWHERE, WO MENTION OF BLEEDING 5723 PORTAL HYPERTENSION D735 Infarction of spleen 5728 OTHER SEQUELAE OF CHRONIC LIVER DISEASE D7389 Other diseases of spleen 5735 -

Extrarenal Complications of the Nephrotic Syndrome
Kidney International, Vol. 33 (/988), pp. 1184—1202 NEPHROLOGY FORUM Extrarenal complications of the nephrotic syndrome Principal discussant: DAVID B. BERNARD The University Hospital and Boston University Sc/zoo!ofMedicine, Boston, Massachusetts present and equal. The temperature was 100°F. The blood pressure was 110/70 mm Hg in the right arm with the patient supine and standing. The Editors patient had no skin rashes, peteehiae, clubbing, or jaundice. Examina- JORDANJ. COHEN tion of the head and neck revealed intact cranial nerves and normal fundi. Ears, nose, and throat were normal. The jugular venous pressure Jot-IN T. HARRtNOTON was not increased. No lymph glands were palpable in the neck or JEROME P. KASSIRER axillae, and the trachea was midline, cardiac examination was normal. NICOLA05 E. MAmAs Examination of the lungs revealed coarse rales at the right base but no other abnormalities. Abdominal examination revealed aseites, but no Editor abdominal guarding, tenderness, or rigidity. The liver and spleen were Managing not palpable and no masses were present. The urine contained 4± CHERYL J. ZUSMAN protein; microscopic examination revealed free fat droplets, many oval fat bodies, and numerous fatty casts. Five to 10 red blood cells were seen per high-power field, but no red blood cell casts were present. A Universityof'Chicago Pritzker School of Medicine 24-hr urine collection contained 8 g of protein. The BUN was 22 mg/dl; creatinine, 2.0 mg/dl; and electrolytes were and normal. Serum total calcium was 7.8 mg/dl, and the phosphorus was 4.0 Taf is University School of' Medicine mg/dl. -

Glomerulonephritis Management in General Practice
Renal disease • THEME Glomerulonephritis Management in general practice Nicole M Isbel MBBS, FRACP, is Consultant Nephrologist, Princess Alexandra lomerular disease remains an important cause Hospital, Brisbane, BACKGROUND Glomerulonephritis (GN) is an G and Senior Lecturer in important cause of both acute and chronic kidney of renal impairment (and is the commonest cause Medicine, University disease, however the diagnosis can be difficult of end stage kidney disease [ESKD] in Australia).1 of Queensland. nikky_ due to the variability of presenting features. Early diagnosis is essential as intervention can make [email protected] a significant impact on improving patient outcomes. OBJECTIVE This article aims to develop However, presentation can be variable – from indolent a structured approach to the investigation of patients with markers of kidney disease, and and asymptomatic to explosive with rapid loss of kidney promote the recognition of patients who need function. Pathology may be localised to the kidney or further assessment. Consideration is given to the part of a systemic illness. Therefore diagnosis involves importance of general measures required in the a systematic approach using a combination of clinical care of patients with GN. features, directed laboratory and radiological testing, DISCUSSION Glomerulonephritis is not an and in many (but not all) cases, a kidney biopsy to everyday presentation, however recognition establish the histological diagnosis. Management of and appropriate management is important to glomerulonephritis (GN) involves specific therapies prevent loss of kidney function. Disease specific directed at the underlying, often immunological cause treatment of GN may require specialist care, of the disease and more general strategies aimed at however much of the management involves delaying progression of kidney impairment. -

Path Renal Outline
Path Renal Outline Krane’s Categorization of Disease + A lot of Extras Kidney Disease Acute Renal Failure Intrinsic Kidney Disease Pre‐Renal Renal Intrinsic Post‐Renal Sodium Excretion <1% Glomerular Disease Tubulointerstitial Disease Sodium Excretion < 1% Sodium Excretion >2% Labs aren’t that useful BUN/Creatinine > 20 BUN/Creatinine < 10 CHF, Cirrhosis, Edema Urinalysis: Proteinuria + Hematuria Benign Proteinuria Spot Test Ratio >1.5, Spot Test Ratio <1.5, Acute Tubular Acute Interstitial Acute 24 Urine contains > 2.0g/24hrs 24 Urine contains < 1.0g/24hrs Necrosis Nephritis Glomerulonephritis Nephrotic Syndrome Nephritic Syndrome Inability to concentrate Urine RBC Casts Dirty Brown Casts Inability to secrete acid >3.5g protein / 24 hrs (huge proteinuria) Hematuria and Proteinuria (<3.5) Sodium Excretion >2% Edema Hypoalbuminemia RBC Casts Hypercholesterolemia Leukocytes Salt and Water Retention = HTN Focal Tubular Necrosis Edema Reduced GFR Pyelonephritis Minimal change disease Allergic Interstitial Nephritis Acute Proliferative Glomerulonephritis Membranous Glomerulopathy Analgesic Nephropathy Goodpasture’s (a form of RPGN) Focal segmental Glomerulosclerosis Rapidly Progressive Glomerulonephritis Multiple Myeloma Post‐Streptococcal Glomerulonephritis Membranoproliferative Glomerulonephritis IgA nephropathy (MPGN) Type 1 and Type 2 Alport’s Meleg‐Smith’s Hematuria Break Down Hematuria RBCs Only RBC + Crystals RBC + WBC RBC+ Protein Tumor Lithiasis (Stones) Infection Renal Syndrome Imaging Chemical Analysis Culture Renal Biopsy Calcium -

Nephrology Clinical Undergraduate Training
School of Medicine Nephrology clinical undergraduate training All care is taken to ensure that the information in this handbook is correct at the time of going to print. Handbook Version 5.0 Date of Origin: March 2019 Contents OBJECTIVES OF ATTACHMENT ................................................................................................... 3 TEACHING STRUCTURE: 3RD MEDICAL YEAR CLINICAL MEDICINE ATTACHMENTS .......................... 3 PROPOSED ATTACHMENT TIMETABLE: ................................................................................................ 5 READING LIST AND WEBSITES ............................................................................................................. 6 2 3rd Medical Year SPECIALTY: Nephrology - www.tcd.ie/medicine/thkc/education/ CONSULTANT: Prof G. Mellotte, Prof C Wall, Dr P Lavin, Dr B Griffin, Prof M Little HOSPITAL: Trinity Health Kidney Centre, Tallaght Hospital YEAR OF COURSE: 3 OBJECTIVES OF ATTACHMENT During this attachment, a student is expected to understand: - The clinical presentation of renal disease, e.g., proteinuria, hypertension, haematuria and uraemia. - Normal regulation of body water and sodium by the RAAS and ADH and how abnormalities give rise to changes in water and sodium homeostasis - Normal values of electrolytes in blood and urine and the clinical sequelae of a derangement in these. - A basic understanding of the following conditions: a. Acute kidney injury (pre-renal, post renal or intrinsic renal) b. Chronic kidney disease, focusing on diabetic nephropathy c. Glomerulonephritis: nephrotic / nephritic syndrome d. Myeloma and the kidney - The management of acute and chronic renal failure, including preparation for dialysis. - Impact of renal failure on drug handling. Be able to: - Take a full and appropriate current and past medical history. - Construct a synopsis or problem list based on the clinical assessment of a patient - Discuss the range of clinical investigations available and understand how they may be used to inform the differential diagnosis. -

16 the Kidney J
16 The Kidney J. Charles Jennette FPO FPO FPO FPO CONGENITAL ANOMALIES IgA Nephropathy (Berger Disease) Renal Agenesis Anti-Glomerular Basement Membrane Ectopic Kidney Glomerulonephritis Horseshoe Kidney ANCA Glomerulonephritis Renal Dysplasia VASCULAR DISEASES CONGENITAL POLYCYSTIC KIDNEY DISEASES Renal Vasculitis Autosomal Dominant Polycystic Kidney Disease Hypertensive Nephrosclerosis (Benign Nephrosclerosis) (ADPKD) Malignant Hypertensive Nephropathy Autosomal Recessive Polycystic Kidney Disease Renovascular Hypertension (ARPKD) Thrombotic Microangiopathy Nephronophthisis–Medullary Cystic Disease Cortical Necrosis ACQUIRED CYSTIC KIDNEY DISEASE DISEASES OF TUBULES AND INTERSTITIUM GLOMERULAR DISEASES Acute Tubular Necrosis (ATN) Nephrotic Syndrome Pyelonephritis Nephritic Syndrome Analgesic Nephropathy Glomerular Inflammation and Immune Mechanisms Drug-Induced (Hypersensitivity) Acute Tubulointerstitial Minimal-Change Glomerulopathy Nephritis Focal Segmental Glomerulosclerosis (FSGS) Light-Chain Cast Nephropathy Membranous Glomerulopathy Urate Nephropathy Diabetic Glomerulosclerosis RENAL STONES (NEPHROLITHIASIS AND Amyloidosis UROLITHIASIS) Hereditary Nephritis (Alport Syndrome) OBSTRUCTIVE UROPATHY AND HYDRONEPHROSIS Thin Glomerular Basement Membrane Nephropathy RENAL TRANSPLANTATION Acute Postinfectious Glomerulonephritis MALIGNANT TUMORS OF THE KIDNEY Type I Membranoproliferative Glomerulonephritis Wilms’ Tumor (Nephroblastoma) Type II Membranoproliferative Glomerulonephritis Renal Cell Carcinoma (RCC) (Dense Deposit Disease) -

Acute Renal Failure Introduction • Incidence Can Range from 7% to 50
Acute Renal Failure Introduction Incidence can range from 7% to 50% of ICU patients Abrupt decline in kidney function (hours to weeks) Acute Kidney Injury Network Criteria (Bellomo R et al. Crit Care. 2004;8(4):R204-R212) Stage Serum Creatinine Criteria Urine Output 1 Cr inc by 1.5-2x or Cr inc by 0.3 mg/dL <0.5 mL/kg/hr for 6 h 2 Cr inc by 2-3x <0.5 mL/kg/hr for 12 h 3 Cr inc by more than 3x or Cr inc of 0.5 <0.3 mL/kg/hr for 24 hr (or anuria with baseline Cr >4 mg/dL for 12 h) Use criteria after fluid challenge in most cases Causes Pre-renal o Volume depletion o Cardiac o Redistribution o Hepatorenal syndrome . Cirrhosis with ascites . Serum creatinine > 1.5 mg/dL . Not improved by holding diuretics and giving albumin challenge (1g/kg for 2 days) . Absence of shock and nephrotoxins . No intrinsic renal disease i.e. no proteinuria (<500 mg/day) or microhematuria (< 50 RBCs) o NSAIDS o ACE-inhibitor Post-renal o Consider obstruction in every patient with ARF o Sites of obstruction . Bladder neck obstruction . Bilateral ureters o Urine volume is variable. Patients can be asymptomatic and with no change in urine output. o Diagnose with renal USG, straight catherization, or bladder scan Intrinsic o Vascular . Vascular occlusion . Atheroembolic disease Eosinophilia, low complement Can see multi-organ dysfunction, livedo reticularis, blue toes Generally irreversible . Thrombotic microangiopathy Fibrin deposition in the microvasculature, intravascular hemolysis, thrombocytopenia, organ dysfunction Associated disorders: Malignant HTN, HUS/TTP, Scleroderma renal crises, HELLP, drugs (tacrolimus, cyclosporine, mitomycin, Plavix) o Glomerular: RPGN . -

Jemds.Com Original Research Article
Jemds.com Original Research Article CLINICAL PROFILE AND SHORT-TERM OUTCOME OF ACUTE NEPHRITIC SYNDROME IN CHILDREN Surya Kandashamparambil Kamalakarababu1, Ansu Sam2, Sajini Varghese3 1Assistant Professor, Department of Paediatrics, Government Medical College, Kottayam. 2Senior Resident, Department of Paediatrics, Government Medical College, Kottayam. 3Assistant Professor, Department of Paediatrics, Government Medical College, Kottayam. ABSTRACT BACKGROUND Glomerulonephritis generally presents as a constellation of findings that includes haematuria, proteinuria and oedema. Poststreptococcal glomerulonephritis is the commonest form of acute glomerulonephritis in developing countries. Objectives- 1. To study the clinical profile of acute glomerulonephritis. 2. To study the different clinical laboratory parameters at admission and at 8 weeks of onset of illness. MATERIAL AND METHODS This is a prospective, descriptive study conducted in a tertiary care teaching hospital in South India from January 2016-December 2016. Data regarding the clinical features, laboratory parameters, treatment were collected. All these patients were further followed up at 8 weeks and descriptive analysis done. RESULTS The most common cause of glomerulonephritis in the study group was poststreptococcal glomerulonephritis (42.9%) followed by drug-induced nephropathy (28.6%). The most common complaints were haematuria, facial puffiness, decreased urine output and oedema. Hypertension was found only in 14.3% of study group. 4.8% of patients had nephrotic range of proteinuria. The most common infection preceding was Pyoderma (61.5%) in case of PSGN. High ASO titre was seen commonly with pharyngitis. 45.2% patients had decreased Serum C3 at diagnosis. All the patients were treated conservatively. At 8 weeks followup, haematuria was persisting in 28.6% patients. Only 2 patients had persistently low serum C3 and single patient had high creatinine. -

An Unusual Occurrence of Erythrocytosis in a Child with Nephrotic Syndrome and Advanced Chronic Kidney Disease
Case Report An Unusual Occurrence of Erythrocytosis in a Child with Nephrotic Syndrome and Advanced Chronic Kidney Disease Ratna Acharya 1 and Kiran Upadhyay 2,* 1 Division of General Pediatrics, Department of Pediatrics, University of Florida, Gainesville, FL 32610, USA; racharya@ufl.edu 2 Division of Pediatric Nephrology, Department of Pediatrics, University of Florida, Gainesville, FL 32610, USA * Correspondence: kupadhyay@ufl.edu; Tel.: +1-352-273-9180 Abstract: Background: Anemia is common in patients with nephrotic syndrome (NS) for various reasons. Furthermore, anemia can occur in patients with chronic kidney disease (CKD) predominantly owing to inappropriately low erythropoietin (EPO) production relative to the degree of anemia. However, erythrocytosis is uncommon in patients with NS and advanced CKD who are not treated with exogenous erythropoietin stimulating agents, and when present, will necessitate exploration of the other etiologies. Case summary: Here, we describe an 8-year-old girl with erythrocytosis in association with NS and advanced CKD. The patient was found to have erythrocytosis during the evaluation for hypertensive urgency. She also had nephrotic range proteinuria without edema. Serum hemoglobin and hematocrit were 17 gm/dL and 51%, respectively, despite hydration. Renal function test showed an estimated glomerular filtration rate of 30 mL/min/1.73 m2. There was mild iron deficiency anemia with serum iron saturation of 18%. Serum EPO level was normal. Urine EPO was not measured. Renal biopsy showed evidence of focal segmental glomerulosclerosis. Genetic testing for NS showed mutations in podocyte genes: NUP93, INF2, KANK1, and ACTN4. Gene Citation: Acharya, R.; Upadhyay, K. sequence analysis of genes associated with erythrocytosis showed no variants in any of these genes. -
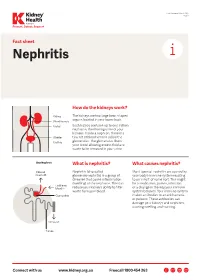
Nephritis Fact Sheet
Last Reviewed March 2017 Page 1 Prevent, Detect, Support. Fact sheet Nephritis How do the kidneys work? The kidneys are two large bean-shaped organs located in your lower back. Each kidney contains up to one million nephrons, the filtering units of your kidneys. Inside a nephron, there is a tiny set of blood vessels called the glomerulus. The glomerulus filters your blood allowing excess fluid and waste to be removed in your urine. What is nephritis? What causes nephritis? Nephritis (also called Most types of nephritis are caused by glomerulonephritis) is a group of your body’s immune system reacting diseases that cause inflammation to an ‘insult’ of some sort. This might (swelling) of the nephrons. This can be a medication, poison, infection reduce your kidney’s ability to filter or a change in the way your immune waste from your blood. system behaves. Your immune system makes antibodies to attack bacteria or poisons. These antibodies can damage your kidneys and nephrons, causing swelling and scarring. Connect with us www.kidney.org.au Freecall 1800 454 363 Kidney Health Australia Nephritis Last Reviewed March 2017 Prevent, Detect, Support. Page 2 What are the different types of nephritis? There are many different types of Different types of nephritis include: Nephrotic syndrome: Damage to the nephritis. It can vary from a mild, nephrons causes them to leak large Focal nephritis: Less than a half of non-damaging condition to a serious amounts of protein into your urine your nephrons have scarring, and problem causing kidney failure. Some but little blood. Losing this protein blood and a small amount of protein types of nephritis appear mild at means your body does not have are found in your urine. -

Nephrotic Syndrome What You Should Know
Nephrotic Syndrome what you should know WHAT IS NEPHROTIC SYNDROME? • Tiny filtering units (glomeruli) in the kidney are damaged or not working. • Protein normally kept in your body, leaks into the urine. Signs and symptoms include: Many diseases can cause it: • High urine protein (proteinuria) • Minimal change disease (MCD) • Swelling (edema) around the eyes, • Membranous glomerulonephritis face, feet, ankles, and/or belly • Focal segmental glomerulosclerosis (FSGS) • Weight gain (from fluid retention) • IGA nephropathy • Foamy urine • Lupus • Poor appetite • Diabetes • High blood cholesterol • Certain infections such as Hepatitis B and C, HIV, others HOW IS IT TESTED? HOW IS IT TREATED? • Physical exam: • Depending on the disease and person’s Visible signs and symptoms overall health, dietary changes and medicines are used to: • Blood and urine tests: - Lower excess salt and fluids in the body Signs of kidney damage and - Lower loss of protein in the urine other diseases - Lower cholesterol in the blood • Imaging tests and/or • Certain medicines that suppress or “calm” kidney biopsy: the immune system can be used. Signs of kidney disease • Sometimes, the dose might need to be • Genetic tests: changed, or a different medicine might Inherited diseases that are be used. linked with kidney disease • In some cases, nephrotic syndrome can lead to kidney failure, which is treated with dialysis or a kidney transplant. Nephrotic Syndrome what you should know HOW CAN I REDUCE MY RISK? Diet, Exercise, and Lifestyle Changes Medicines • Follow a healthy diet that is low in salt • Before taking any over-the-counter and cholesterol. medicine or supplement, ask your healthcare provider which is safe.