An Assessment of Advancing Adolescent Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Farmers' Organizations in Bangladesh: a Mapping and Capacity
Farmers’ Organizations in Bangladesh: Investment Centre Division A Mapping and Capacity Assessment Food and Agriculture Organization of the United Nations (FAO) Viale delle Terme di Caracalla – 00153 Rome, Italy. Bangladesh Integrated Agricultural Productivity Project Technical Assistance Component FAO Representation in Bangladesh House # 37, Road # 8, Dhanmondi Residential Area Dhaka- 1205. iappta.fao.org I3593E/1/01.14 Farmers’ Organizations in Bangladesh: A Mapping and Capacity Assessment Bangladesh Integrated Agricultural Productivity Project Technical Assistance Component Food and agriculture organization oF the united nations rome 2014 Photo credits: cover: © CIMMYt / s. Mojumder. inside: pg. 1: © FAO/Munir uz zaman; pg. 4: © FAO / i. nabi Khan; pg. 6: © FAO / F. Williamson-noble; pg. 8: © FAO / i. nabi Khan; pg. 18: © FAO / i. alam; pg. 38: © FAO / g. napolitano; pg. 41: © FAO / i. nabi Khan; pg. 44: © FAO / g. napolitano; pg. 47: © J.F. lagman; pg. 50: © WorldFish; pg. 52: © FAO / i. nabi Khan. Map credit: the map on pg. xiii has been reproduced with courtesy of the university of texas libraries, the university of texas at austin. the designations employed and the presentation of material in this information product do not imply the expression of any opinion whatsoever on the part of the Food and agriculture organization of the united nations (FAO) concerning the legal or development status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. the mention of specific companies or products of manufacturers, whether or not these have been patented, does not imply that these have been endorsed or recommended by FAO in preference to others of a similar nature that are not mentioned. -
Lamb Annual Report 2020
ANNUAL REPORT | January 2018 - June 2019 Message from the Board Chairperson I am pleased to give my short message to anyone who reads this report of LAMB’s work for 2018/19. It has been a distinct pleasure to have been on the LAMB board for numerous years over the life of my career in Bangladesh of 33 years as an agriculture missionary then scientist. LAMB has evolved over the years, with this past year striking a distinct position. While we as the LAMB Governing Board use the Carver method of governance, this year is the first year where the reporting is using LAMB’s overall goals as the organizing structure (instead of departments). This is a remarkable step in the right direction whereby the fruits of LAMB’s health and development work can be more effectively measured and reported. This past year represents a renewed commitment toward excellence for the future. Everything from improved contacts with local government and health facilities to the NGO Bureau, points LAMB to a brighter future. LAMB responded to flooding in their area by contacts with the UN agencies and became a conduit for relief, proving LAMB’s resilience in not only their forte of health work but also to respond to the needs of the community. A quick perusal of this report will give the reader a real flavour for where LAMB has been in the past year, the results of years of efforts with the local community, and of course wholeness of healing many persons with various illnesses. LAMB is at a cross road; it can remain the same consistent hospital and development team or it can increase its access to finance and investment to become a successful and sustainable hospital, serving both the poor but also the needs of the increasing lower middle income society as Bangladesh people have higher incomes. -
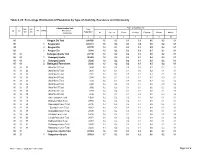
Badarganj Paurashava Table C-09: Percentage Distribution Of
Table C-09: Percentage Distribution of Population by Type of disability, Residence and Community Administrative Unit Type of disability (%) UN / MZ / Total ZL UZ Vill RMO Residence WA MH Population Community All Speech Vision Hearing Physical Mental Autism 1 2 3 4 5 6 7 8 9 10 85 Rangpur Zila Total 2881086 1.6 0.2 0.3 0.2 0.6 0.2 0.1 85 1 Rangpur Zila 2438373 1.6 0.2 0.3 0.2 0.6 0.2 0.1 85 2 Rangpur Zila 387370 1.3 0.1 0.3 0.1 0.5 0.2 0.1 85 3 Rangpur Zila 55343 1.3 0.2 0.2 0.2 0.5 0.2 0.1 85 03 Badarganj Upazila Total 287746 1.2 0.2 0.2 0.1 0.5 0.2 0.1 85 03 1 Badarganj Upazila 262460 1.2 0.2 0.2 0.1 0.4 0.2 0.1 85 03 2 Badarganj Upazila 25286 1.3 0.2 0.2 0.1 0.5 0.2 0.1 85 03 2 Badarganj Paurashava 25286 1.3 0.2 0.2 0.1 0.5 0.2 0.1 85 03 01 Ward No-01 Total 3594 1.5 0.5 0.0 0.0 0.7 0.2 0.1 85 03 02 Ward No-02 Total 2891 1.0 0.4 0.1 0.0 0.2 0.1 0.1 85 03 03 Ward No-03 Total 2372 1.1 0.1 0.5 0.1 0.3 0.1 0.0 85 03 04 Ward No-04 Total 2744 1.4 0.1 0.3 0.1 0.5 0.3 0.1 85 03 05 Ward No-05 Total 3134 1.3 0.3 0.3 0.0 0.3 0.2 0.2 85 03 06 Ward No-06 Total 2368 1.4 0.2 0.0 0.1 0.5 0.5 0.2 85 03 07 Ward No-07 Total 3706 1.2 0.0 0.3 0.1 0.6 0.2 0.0 85 03 08 Ward No-08 Total 2259 1.4 0.4 0.2 0.1 0.5 0.1 0.0 85 03 09 Ward No-09 Total 2218 1.2 0.1 0.1 0.2 0.5 0.2 0.2 85 03 16 Kalu Para Union Total 19697 1.2 0.2 0.2 0.1 0.4 0.1 0.1 85 03 18 Bishnupur Union Total 29860 1.2 0.2 0.2 0.1 0.5 0.1 0.1 85 03 25 Damodarpur Union Total 28310 1.3 0.2 0.2 0.1 0.5 0.2 0.1 85 03 31 ' Gopalpur' Union Total 28252 1.1 0.2 0.2 0.1 0.4 0.2 0.1 85 03 37 Gopinathpur Union -

District Statistics 2011 Rangpur
জলা পিরসংান 3122 রংর District Statistics 2011 Rangpur June 2013 BANGLADESH BUREAU OF STATISTICS STATISTICS AND INFORMATICS DIVISION MINISTRY OF PLANNING GOVERNMENT OF THE PEOPLE'S REPUBLIC OF BANGLADESH District Statistics 2011 District Statistics 2011 Published in June, 2013 Published by : Bangladesh Bureau of Statistics (BBS) Printed at : Reproduction, Documentation and Publication (RDP), FA & MIS, BBS Cover Design: Chitta Ranjon Ghosh, RDP, BBS ISBN: For further information, please contract: Bangladesh Bureau of Statistics (BBS) Statistics and Informatics Division (SID) Ministry of Planning Government of the People’s Republic of Bangladesh Parishankhan Bhaban E-27/A, Agargaon, Dhaka-1207. www.bbs.gov.bd COMPLIMENTARY This book or any portion thereof cannot be copied, microfilmed or reproduced for any commercial purpose. Data therein can, however, be used and published with acknowledgement of the sources. ii District Statistics 2011 Foreword I am delighted to learn that Bangladesh Bureau of Statistics (BBS) has successfully completed the ‘District Statistics 2011’ under Medium-Term Budget Framework (MTBF). The initiative of publishing ‘District Statistics 2011’ has been undertaken considering the importance of district and upazila level data in the process of determining policy, strategy and decision-making. The basic aim of the activity is to publish the various priority statistical information and data relating to all the districts of Bangladesh. The data are collected from various upazilas belonging to a particular district. The Government has been preparing and implementing various short, medium and long term plans and programs of development in all sectors of the country in order to realize the goals of Vision 2021. -

Getting to Grips with Power Can Ngos Improve Justice in Bangladesh?
Report Getting to grips with power Can NGOs improve justice in Bangladesh? Craig Valters and Ferdous Jahan March 2017 This research paper is a product of a collaboration between ODI and dRi. Development Research Initiative (dRi) is a leading independent consultancy, research and evaluation center in Bangladesh. dRi conducts dynamic research and analysis of a wide range of issues related to development, international aid, NGOs, markets and the state. Since its inception in 2008, dRi has completed a wide array of research projects, building its reputation for generating high-quality evidence of what works in development practice. Overseas Development Institute 203 Blackfriars Road London SE1 8NJ Tel. +44 (0) 20 7922 0300 Fax. +44 (0) 20 7922 0399 E-mail: [email protected] www.odi.org www.odi.org/facebook www.odi.org/twitter Readers are encouraged to reproduce material from ODI Reports for their own publications, as long as they are not being sold commercially. As copyright holder, ODI requests due acknowledgement and a copy of the publication. For online use, we ask readers to link to the original resource on the ODI website. The views presented in this paper are those of the author(s) and do not necessarily represent the views of ODI. © Overseas Development Institute 2017. This work is licensed under a Creative Commons Attribution-NonCommercial Licence (CC BY-NC 4.0). Cover photo: ‘Courtyard Meeting’ for raising awareness on legal rights and entitlements, Madaripur Sadar Upazila, Madaripur District, Bangladesh, 2012 © Emdadul Islam Bitu Acknowledgements This research benefited from the support of a wide range of people, both within Bangladesh and internationally. -

Zila Report : Rangpur
POPULATION & HOUSING CENSUS 2011 ZILA REPORT : RANGPUR Bangladesh Bureau of Statistics Statistics and Informatics Division Ministry of Planning BANGLADESH POPULATION AND HOUSING CENSUS 2011 Zila Report: RANGPUR October 2015 BANGLADESH BUREAU OF STATISTICS (BBS) STATISTICS AND INFORMATICS DIVISION (SID) MINISTRY OF PLANNING GOVERNMENT OF THE PEOPLE’S REPUBLIC OF BANGLADESH ISBN-978-984-33-8638-0 COMPLIMENTARY Published by Bangladesh Bureau of Statistics (BBS) Statistics and Informatics Division (SID) Ministry of Planning Website: www.bbs.gov.bd This book or any portion thereof cannot be copied, microfilmed or reproduced for any commercial purpose. Data therein can, however, be used and published with acknowledgement of their sources. Contents Page Message of Honorable Minister, Ministry of Planning …………………………………………….. vii Message of Honorable State Minister, Ministry of Finance and Ministry of Planning …………. ix Foreword ……………………………………………………………………………………………….. xi Preface …………………………………………………………………………………………………. xiii Zila at a Glance ………………………………………………………………………………………... xv Physical Features ……………………………………………………………………………………... xix Zila Map ………………………………………………………………………………………………… xxi Geo-code ………………………………………………………………………………………………. xxii Chapter-1: Introductory Notes on Census ………………………………………………………….. 1 1.1 Introduction ………………………………………………………………………………… 1 1.2 Census and its periodicity ………………………………………………………………... 1 1.3 Objectives ………………………………………………………………………………….. 1 1.4 Census Phases …………………………………………………………………………… 2 1.5 Census Planning …………………………………………………………………………. -

List of Upazilas of Bangladesh
List Of Upazilas of Bangladesh : Division District Upazila Rajshahi Division Joypurhat District Akkelpur Upazila Rajshahi Division Joypurhat District Joypurhat Sadar Upazila Rajshahi Division Joypurhat District Kalai Upazila Rajshahi Division Joypurhat District Khetlal Upazila Rajshahi Division Joypurhat District Panchbibi Upazila Rajshahi Division Bogra District Adamdighi Upazila Rajshahi Division Bogra District Bogra Sadar Upazila Rajshahi Division Bogra District Dhunat Upazila Rajshahi Division Bogra District Dhupchanchia Upazila Rajshahi Division Bogra District Gabtali Upazila Rajshahi Division Bogra District Kahaloo Upazila Rajshahi Division Bogra District Nandigram Upazila Rajshahi Division Bogra District Sariakandi Upazila Rajshahi Division Bogra District Shajahanpur Upazila Rajshahi Division Bogra District Sherpur Upazila Rajshahi Division Bogra District Shibganj Upazila Rajshahi Division Bogra District Sonatola Upazila Rajshahi Division Naogaon District Atrai Upazila Rajshahi Division Naogaon District Badalgachhi Upazila Rajshahi Division Naogaon District Manda Upazila Rajshahi Division Naogaon District Dhamoirhat Upazila Rajshahi Division Naogaon District Mohadevpur Upazila Rajshahi Division Naogaon District Naogaon Sadar Upazila Rajshahi Division Naogaon District Niamatpur Upazila Rajshahi Division Naogaon District Patnitala Upazila Rajshahi Division Naogaon District Porsha Upazila Rajshahi Division Naogaon District Raninagar Upazila Rajshahi Division Naogaon District Sapahar Upazila Rajshahi Division Natore District Bagatipara -

Phone No. Upazila Health Center
gvevBj ÑdvÖb ß^vßå† Ñmev gvevBj ÑdvÖbi gva†Ög bvMwiKMY GLb miKvix ß^vßå† ÑKÖï`¢ Kg°iZ wPwKrmÖKi KvQ Ñ_ÖK webvg~Öj† ß^vßå† civgk° wbÖZ cviÖQb| ÑmRb† evsjvÖ`Öki cŒwZwU ÑRjv DcÖRjv nvmcvZvÖj( ÑgvU 482wU nvmcvZvj) GKwU KÖi ÑgvevBj Ñdvb Ñ`qv nÖqÖQ| AvcwbI GB Ñmev MŒnY KiÖZ cvÖib| Gme ÑgvevBj ÑdvÖbi bú^i ßåvbxq ch°vÖq cŒPvÖii e†eßåv Kiv nÖqÖQ| 24 NïUv e†vcx ÑKvb bv ÑKvb wPwKrmK GB ÑgvevBj ÑdvÖbi Kj wiwmf KÖib| ßåvbxq RbMY Gme ÑgvevBj ÑdvÖb Ñdvb KÖi nvmcvZvÖj bv GÖmB webvg~Öj† wPwKrmv civgk° wbÖZ cvÖib District Upazila Name of Hospitals Mobile No. Dinajpur Birampur Birampur Upazila Health Complex 01730324634 Dinajpur Birganj Birganj Upazila Health Complex 01730324635 Dinajpur Birol Birol Upazila Health Complex 01730324636 Dinajpur Bochaganj Bochaganj Upazila Health Complex 01730324637 Dinajpur Chirirbandar Chirirbandar Upazila Health Complex 01730324638 Dinajpur Fulbari Fulbari Upazila Health Complex 01730324639 Dinajpur Ghoraghat Ghoraghat Upazila Health Complex 01730324640 Dinajpur Hakimpur Hakimpur Upazila Health Complex 01730324641 Dinajpur Kaharol Kaharol Upazila Health Complex 01730324642 Dinajpur Khansama Khansama Upazila Health Complex 01730324643 Dinajpur Nawabganj Nawabganj Upazila Health Complex 01730324644 Dinajpur Parbatipur Parbatipur Upazila Health Complex 01730324645 Dinajpur District Sadar District Hospital 01730324805 District Upazila Name of Hospitals Mobile No. Jessore Abhoynagar Abhoynagar Upazila Health Complex 01730324581 Jessore Bagherpara Bagherpara Upazila Health Complex 01730324582 Jessore Chowgacha Chowgacha Upazila -

Bangladesh Journal of Public Administration Volume XXV Number I 2017
Bangladesh Journal of Public Administration Volume XXV Number I 2017 BPATC: P31/EJ (725)/94 BPATC: LIBRARY: 05035 ISSN 1563-5032 Peer Reviewed Journal @2017 Bangladesh Public Administration Training Centre Savar, Dhaka, Bangladesh (Actual Time of Publication- June 2018) All business correspondence should be addressed to Deputy Director (Publication) Bangladesh Public Administration Training Centre Savar, Dhaka, Bangladesh Rates of Subscription Bangladesh: Tk. 180:00 per issue, Tk. 360 per year Foreign: US $ 15 per year (including air postage) 2 The Bangladesh Journal of Public Administration is a bi-annual publication of the Bangladesh Public Administration Training Centre (BPATC), Savar, Dhaka. This Journal is issued to disseminate the latest research on social sciences in general and Economics and Public Administration in particular. Opinions expressed are those of the authors and do not necessarily reflect the policy of the organizations in which they work or of the Centre. Again the Editor, Assistant Editor, the Editorial Board and the publisher accept no responsibility or liability whatsoever for any inaccurate or misleading data, opinion or statement. The Editor reserves the rights to edit the materials to conform in the style and format of the Journal. Manuscripts of papers, reviewed articles will be considered for publication on the understanding that they have not been published or submitted simultaneously for publication elsewhere. MANUSCRIPT SPECIFICATIONS: Manuscripts should be based on substantive research on the areas mentioned above. Please submit three copies of your manuscript. Two copies will be used for blind review. So these copies must have no authors‟ names. Please send a copy of the manuscript to Editor labeled with the title of the articles and author (s) name. -
Annual Report 2016
ANNUAL REPORT 2016 Introducing LAMB's Updated Brand A bit about LAMB World Mission Prayer League (LAMB Hospital) or 'LAMB' is a registered International NGO in Bangladesh and is a separately constituted organization of the World Mission Prayer League, Inc., based in Minneapolis, MN, USA. Since 1997 LAMB has used its own brand to more clearly communicate who we are in Bangladesh. After twenty years of using that logo, we now present a new brand that provides some consistency from the past and with a new modern look. The Design The new logo design carries over some important aspects from the old. The map of Bangladesh has been put into an artistic design using the shape of Bangladesh. The cross of Jesus Christ has been adapted and communicates our Christian identity and focus on health care.We are a multilingual community, hence the use of both Bangla and English in our logo and tag lines. The tag lines 'That All May Have Abundant Life' remains as LAMB's ultimate purpose coming from God's Word and 'Integrated Rural Health and Development' explains in part how we are going about doing it. The Color Palette Scarlet : The use of the color Scarlet represents LAMB's Christian identity and the power that is in the blood of Jesus Christ. His precious blood redeems us, 'as of a lamb without blemish and without spot'. His blood brings us into fellowship with God, reconciles us to God, cleanses us from sin and gives us power over the devil. LAMB is committed to sacrificial service to the people of Bangladesh as exemplified by the life, death and resurrection of Jesus Christ. -
Esdo Profile
2016 ESDO PROFILE Head Office Address: Collegepara, Thakurgaon, Bangladesh Post: Thakurgaon-5100, Upazila: Thakurgaon Sadar District: Thakurgaon, Bangladesh Phone: +88-0561-52149, Fax: +88-0561-61599 Mobile: +88-01714-063360 E-mail: [email protected], [email protected] Web: www. esdo.net.bd Dhaka Office : ESDO House, Plot # 748, Road # 08, Baitul Aman Housing Society, Adabar Dhaka-1207, Bangladesh Phone: +88-02-58154857, Mobile:+88-01713-149259 E-mail: [email protected], Web: www. esdo.net.bd Contents 1.Background of ESDO ....................................................................................................................... 3 2. Executive Summery ......................................................................................................................... 3 3. Vision ............................................................................................................................................... 4 4. Mission ............................................................................................................................................ 4 5. Establishment: ................................................................................................................................. 4 6. Legal Status .................................................................................................................................... 4 7. Networking ..................................................................................................................................... -

Phone No. Upazila Health Center
District Upazila Name of Hospitals Mobile No. Bagerhat Chitalmari Chitalmari Upazila Health Complex 01730324570 Bagerhat Fakirhat Fakirhat Upazila Health Complex 01730324571 Bagerhat Kachua Kachua Upazila Health Complex 01730324572 Bagerhat Mollarhat Mollarhat Upazila Health Complex 01730324573 Bagerhat Mongla Mongla Upazila Health Complex 01730324574 Bagerhat Morelganj Morelganj Upazila Health Complex 01730324575 Bagerhat Rampal Rampal Upazila Health Complex 01730324576 Bagerhat Sarankhola Sarankhola Upazila Health Complex 01730324577 Bagerhat District Sadar District Hospital 01730324793 District Upazila Name of Hospitals Mobile No. Bandarban Alikadam Alikadam Upazila Health Complex 01730324824 Bandarban Lama Lama Upazila Health Complex 01730324825 Bandarban Nykongchari Nykongchari Upazila Health Complex 01730324826 Bandarban Rowangchari Rowangchari Upazila Health Complex 01811444605 Bandarban Ruma Ruma Upazila Health Complex 01730324828 Bandarban Thanchi Thanchi Upazila Health Complex 01552140401 Bandarban District Sadar District Hospital, Bandarban 01730324765 District Upazila Name of Hospitals Mobile No. Barguna Bamna Bamna Upazila Health Complex 01730324405 Barguna Betagi Betagi Upazila Health Complex 01730324406 Barguna Pathargatha Pathargatha Upazila Health Complex 01730324407 Barguna Amtali Amtali Upazila Health Complex 01730324759 Barguna District Sadar District Hospital 01730324884 District Upazila Name of Hospitals Mobile No. Barisal Agailjhara Agailjhara Upazila Health Complex 01730324408 Barisal Babuganj Babuganj Upazila Health