1-Introduction to the Orthopedics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Koolen-De Vries Syndrome: Clinical Report of an Adult and Literature Review
Case Report Cytogenet Genome Res 2016;150:40–45 Accepted: July 25, 2016 DOI: 10.1159/000452724 by M. Schmid Published online: November 17, 2016 Koolen-de Vries Syndrome: Clinical Report of an Adult and Literature Review Claudia Ciaccio Chiara Dordoni Marco Ritelli Marina Colombi Division of Biology and Genetics, Department of Molecular and Translational Medicine, School of Medicine, University of Brescia, Brescia , Italy Key Words Koolen-de Vries syndrome (KdS, also known as 17q21.31 · Deletion · Joint hypermobility · KANSL1 17q21.31 microdeletion syndrome, OMIM #610443) is a rare genetic disorder (prevalence 1/16,000) characterized by typical facial dysmorphisms, cardiac and renal defects, Abstract developmental delay, and intellectual disability of vari- Koolen-de Vries syndrome (KdS) is a rare genetic condition able level [Tan et al., 2009]. The disorder was initially de- characterized by typical facial dysmorphisms, cardiac and re- scribed as a form of mental retardation caused by a 440– nal defects, skeletal anomalies, developmental delay, and in- 680-kb deletion in the 17q21.31 region, typically encom- tellectual disability of variable level. It is caused by a 440– passing 5 genes: CRHR1 (OMIM 122561), MAPT 680-kb deletion in the 17q21.31 region, encompassing (OMIM 157140), IMP5 (OMIM 608284), STH (OMIM CRHR1 , MAPT , IMP5 , STH , and KANSL1 , or by an intragenic 607067), and KANSL1 (OMIM 612452)* [Koolen et al., KANSL1 mutation. The majority of the patients reported are 2006]. Recently,* it has been shown* that haploinsufficien- pediatric or young adults, and long-term studies able to de- cy* of KANSL1 by itself, due to single* nucleotide variants fine the prognosis of the disease are lacking. -

Phenotypic and Genotypic Characterisation of Noonan-Like
1of5 ELECTRONIC LETTER J Med Genet: first published as 10.1136/jmg.2004.024091 on 2 February 2005. Downloaded from Phenotypic and genotypic characterisation of Noonan-like/ multiple giant cell lesion syndrome J S Lee, M Tartaglia, B D Gelb, K Fridrich, S Sachs, C A Stratakis, M Muenke, P G Robey, M T Collins, A Slavotinek ............................................................................................................................... J Med Genet 2005;42:e11 (http://www.jmedgenet.com/cgi/content/full/42/2/e11). doi: 10.1136/jmg.2004.024091 oonan-like/multiple giant cell lesion syndrome (NL/ MGCLS; OMIM 163955) is a rare condition1–3 with Key points Nphenotypic overlap with Noonan’s syndrome (OMIM 163950) and cherubism (OMIM 118400) (table 1). N Noonan-like/multiple giant cell lesion syndrome (NL/ Recently, missense mutations in the PTPN11 gene on MGCLS) has clinical similarities with Noonan’s syn- chromosome 12q24.1 have been identified as the cause of drome and cherubism. It is unclear whether it is a Noonan’s syndrome in 45% of familial and sporadic cases,45 distinct entity or a variant of Noonan’s syndrome or indicating genetic heterogeneity within the syndrome. In the cherubism. 5 study by Tartaglia et al, there was a family in which three N Three unrelated patients with NL/MGCLS were char- members had features of Noonan’s syndrome; two of these acterised, two of whom were found to have mutations had incidental mandibular giant cell lesions.3 All three in the PTPN11 gene, the mutation found in 45% of members were found to have a PTPN11 mutation known to patients with Noonan’s syndrome. -

Loss of Correction in Cubitus Varus Deformity After Osteotomy
Loss of correction in cubitus varus deformity after osteotomy Chao You Shenzhen children's hospital Yibiao Zhou Shenzhen children's hospital https://orcid.org/0000-0001-9754-1089 Jingming Han ( [email protected] ) Research article Keywords: cubitus varus osteotomy Loss of correction Posted Date: May 5th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-26279/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/14 Abstract Purpose Cubitus varus deformity in the pediatric population is an infrequent but clinically important disease to orthopedic surgeons. Since these patient populations are different in many respects, we sought out to investigate the rates of loss of correction over time as well as the factors associated with loss of correction in pediatric patients undergoing osteotomy for treatment of cubitus varus deformity. Methods Between 2008-7 and 2017-7, we treated 30 cases of cubital varus had underwent the the osteotomy. We compared preoperative and postoperative clinical and imaging parameters (H-cobb angle,Baumman angle) for all patients. Postoperative evaluation was performed by telephone interview. Results In our study,there were 30 patients,included 17 males and 13 females.the mean age was 75 months old.In the rst follow-up,Approximately 80 % of patients had a loss of correction of H-cobband 83% of patients at the second follow-up. The Baumann angle also had a loss of correction,about 57% was lost at the rst follow-up,and 43% was lost at the second follow-up. The average interval between the rst follow-up and the second follow-up was 24 days The H-cobb angle mean loss was 2.4°.There was a statistically signicant difference between the H-cobb angle measured before surgery and the angle measured after surgery (p <0.05). -
Efficacy and Safety of a Novel Personalized Navigation Template in Proximal Femoral Corrective Osteotomy for the Treatment of DDH Qiang Shi1,2 and Deyi Sun1*
Shi and Sun Journal of Orthopaedic Surgery and Research (2020) 15:317 https://doi.org/10.1186/s13018-020-01843-y RESEARCH ARTICLE Open Access Efficacy and safety of a novel personalized navigation template in proximal femoral corrective osteotomy for the treatment of DDH Qiang Shi1,2 and Deyi Sun1* Abstract Background: This present study is aimed to retrospectively evaluate the efficacy and safety of a novel personalized navigation template in proximal femoral corrective osteotomy for the treatment of DDH. Methods: Twenty-nine consecutive patients with DDH who underwent proximal femoral corrective osteotomy were evaluated between August 2013 and June 2017. Based on the different surgical methods, they were divided into the conventional group (n = 14) and navigation template group (n = 15). The osteotomy degrees, radiation exposure, and operation time were compared between the two groups. Results: No major complications relating to osteotomy surgery such as redislocation or avascular necrosis occurred in the navigation template group, which had more accurate osteotomy degrees, less radiation exposure, and shorter operation time when compared with the conventional group (P < 0.05). Moreover, there was significant difference according to the McKay criteria between the two groups (P = 0.0362). Conclusions: The novel personalized navigation template in proximal femoral corrective osteotomy is effective and safe, which could improve the femoral osteotomy accuracy, reduce radiation exposure, and shorten operation time. Keywords: Femoral corrective osteotomy, 3D printing, Navigation template, Developmental dysplasia of the hip Background [3–5]. The performance and positioning of femoral oste- Developmental dysplasia of the hip (DDH) is considered otomy is one of the most important surgical procedures one of the most common three-dimensional (3D) hip to ensure ideal correction effects, but the conventional deformities in children [1]. -
1 Tips7pp P654-660CR2.Indd
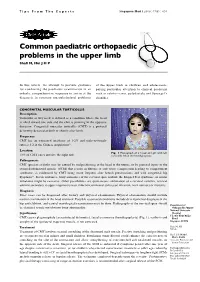
Tips From The Experts SingaporeSingapore Med Med J 2006; J 2006; 47(8) 47(8) : 654 : 1 Common paediatric orthopaedic problems in the upper limb Shafi M, Hui J H P In this article, we attempt to provide guidance of the upper limb in children and adolescents, for conducting the paediatric examination in an paying particular attention to clinical problems orderly, comprehensive sequence to arrive at the such as cubitus varus, polydactyly and Sprengel’s diagnosis in common musculoskeletal problems shoulder. CONGENITAL MUSCULAR TORTICOLLIS Description Torticollis or wry neck is defined as a condition where the head is tilted toward one side and the chin is pointing in the opposite direction. Congenital muscular torticollis (CMT) is a postural deformity detected at birth or shortly after birth. Frequency CMT has an estimated incidence of 1-2% and male-to-female ratio is 3:2 in the Chinese population(1). Location Fig. 1 Photograph of a 3-year-old girl with left 75% of CMT cases involve the right side. torticollis. Note the hemihypoplasia. Pathogenesis CMT (present at birth) may be caused by malpositioning of the head in the uterus, or by prenatal injury to the sternocleidomastoid muscle (SCM) that results in fibrosis or soft tissue compression leading to compartment syndrome, as evidenced by CMT being more frequent after breech presentations and with congenital hip dysplasia(2). In rare instances, bony anomalies of the cervical spine include the Klippel-Feil syndrome, or ocular imbalance might be causative. Other possibilities are spontaneous subluxation of a cervical vertebra, cervical adenitis secondary to upper respiratory tract infection, unilateral soft tissue infection, neck tumours or myositis. -
Quesid: -1 Which Bone Does Not Form the Wrist Joint 1
匀夀䰀䰀䄀䈀唀匀 䐀爀⸀ 䄀瀀甀爀瘀 䴀攀栀爀愀 QuesID: -1 Which Bone does not form the Wrist joint 1. Radius 2. Triquetrum 3. Scaphoid 4. Ulna QuesID: -2 Sunray appearance in osteosarcoma is due to: 1. Bone destruction 2. Periosteal reaction 3. Vascular calcification 4. Bone hypertrophy QuesID: -3 Most sensitive investigation for early bone infections is: (NEET DEC 2016) 1. X-ray 2. CT scan 3. Bone scan 4. USG QuesID: -4 Stress fractures are diagnosed by:(JIPMER May 2016, AIIMS May 2015, AI 2004) 1. X-ray 2. CT 3. MRI 4. Bone scan QuesID: -5 Identify the marked structure: (AI 2016) 1. Trapezium 2. Lunate 3. Trapezoid 4. Capitate QuesID: -6 Synovial Tenosynovitis of flexor tendon. What is the correct option? 1. The affected finger is extended at all joints 2. It has to be conservatively managed 3. Little finger infection can spread to thumb but not to index finger 4. Patient present with minimal pain QuesID: -7 12 years male came with swelling of lower end tibia which is surrounded by rim of reactive bone. What is most likely diagnosis? 1. GCT 2. Brodie’s Abscess 3. Hyper PTH 4. Osteomyelitis QuesID: -8 Which amongst the following occurs in immunocompetent host ? 1. GCT 2. Brodie’s Abscess 3. Hyper PTH 4. Osteomyelitis \ QuesID: -9 A child presents with fever and discharging pus from right thigh x 3 months. Following is the xray. Identify the labelled structured: 1. Sequestrum 2. Cloacae 3. Involucrum 4. Worsen Bone QuesID: -10 Tom smith septic arthritis affects? 1. Neck of infants 2. Hip joint of infants 3. -

Expanded Indications for Guided Growth in Pediatric Extremities
Current Concept Review Expanded Indications for Guided Growth in Pediatric Extremities Teresa Cappello, MD Shriners Hospitals for Children, Chicago, IL Abstract: Guided growth for coronal plane knee deformity has successfully historically been utilized for knee val- gus and knee varus. More recent use of this technique has expanded its indications to correct other lower and upper extremity deformities such as hallux valgus, hindfoot calcaneus, ankle valgus and equinus, rotational abnormalities of the lower extremity, knee flexion, coxa valga, and distal radius deformity. Guiding the growth of the extremity can be successful and is a low morbidity method for correcting deformity and should be considered early in the treatment of these conditions when the child has a minimum of 2 years of growth remaining. Further expansion of the application of this concept in the treatment of pediatric limb deformities should be considered. Key Concepts: • Guiding the growth of pediatric physes can successfully correct a variety of angular and potentially rotational deformities of the extremities. • Guided growth can be performed using a variety of techniques, from permanent partial epiphysiodesis to tem- porary methods utilizing staples, screws, or plate and screw constructs. • Utilizing the potential of growth in the pediatric population, guided growth principals have even been success- fully applied to correct deformities such as knee flexion contractures, hip dysplasia, femoral anteversion, ankle deformities, hallux valgus, and distal radius deformity. Introduction Guiding the growth of pediatric orthopaedic deformities other indications and uses for guided growth that may is represented by the symbol of orthopaedics itself, as not have wide appreciation. the growth of a tree is guided as it is tethered to a post (Figure 1). -

Malunion of Long Bones
Malunion of long bones Andreas Panagopoulos Assistant professor in Orthopaedics University Hospital of Patras Definition A malunited fracture is one that has healed with the fragments in a non- anatomical position Acceptability of fracture reduction alignment rotation normal length actual position of fragments (least important) Classification Based to location Intrarticular Metaphsial Diaphysial Based to complexity Simple (one plane) e.g. valgus-varus Complex ( multi planes) However, some malalignments are better tolerated from the neighboring joints than others (e.g. malunions of the upper extremity) Also lower leg valgus is more acceptable than varus This means there are both relative and absolute indications to correct deformities and leg length discrepancies Absolute Indications - Presence of disabling pain - Severe functional disability Relative Indications - Cosmetic reasons - No response to nonoperative treatment The object of surgery for malunion is to restore function Operative treatment for malunion of most fractures should not be considered until 6 to 12 months after the fracture has occurred. However, in intraarticular fractures, surgery may be required sooner if satisfactory function is to be restored When considering surgical correction of the malunion we should take in account: 1. Age of the patient 2. Socio-economic factors 3. The function of the joint 4. The bone stock and the degree of osteoporosis 5. The state of the soft tissue envelope Corrective surgery at the site of malunion is not always feasible. In some instances, -

Page 1 of 4 COPYRIGHT © by the JOURNAL of BONE and JOINT SURGERY, INCORPORATED LAMPLOT ET AL
COPYRIGHT © BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED LAMPLOT ET AL. RISK OF SUBSEQUENT JOINT ARTHROPLASTY IN CONTRALATERAL OR DIFFERENT JOINT AFTER INDEX SHOULDER, HIP, OR KNEE ARTHROPLASTY http://dx.doi.org/10.2106/JBJS.17.00948 Page 1 Appendix TABLE E-1 Included Alternative Primary Diagnoses ICD-9-CM Code Diagnosis* 716.91 Arthropathy NOS, shoulder 716.95 Arthropathy NOS, pelvis 716.96 Arthropathy NOS, lower leg 719.45 Joint pain, pelvis 719.91 Joint disease NOS, shoulder *NOS = not otherwise specified. Page 1 of 4 COPYRIGHT © BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED LAMPLOT ET AL. RISK OF SUBSEQUENT JOINT ARTHROPLASTY IN CONTRALATERAL OR DIFFERENT JOINT AFTER INDEX SHOULDER, HIP, OR KNEE ARTHROPLASTY http://dx.doi.org/10.2106/JBJS.17.00948 Page 2 TABLE E-2 Excluded Diagnoses* ICD-9- ICD-9- ICD-9- ICD-9- CM Code Diagnosis CM Code Diagnosis CM Code Diagnosis CM Code Diagnosis 274 Gouty arthropathy NOS 696 Psoriatic 711.03 Pyogen 711.38 Dysenter arthropathy arthritis- arthritis NEC forearm 274.01 Acute gouty arthropathy 696.1 Other psoriasis 711.04 Pyogen 711.4 Bact arthritis- arthritis-hand unspec 274.02 Chr gouty arthropathy 696.2 Parapsoriasis 711.05 Pyogen 711.46 Bact arthritis- w/o tophi arthritis-pelvis l/leg 274.03 Chr gouty arthropathy w 696.3 Pityriasis rosea 711.06 Pyogen 711.5 Viral arthritis- tophi arthritis-l/leg unspec 274.1 Gouty nephropathy NOS 696.4 Pityriasis rubra 711.07 Pyogen 711.55 Viral arthritis- pilaris arthritis-ankle pelvis 274.11 Uric acid nephrolithiasis 696.5 Pityriasis NEC & 711.08 -

Introduction to the Orthopedics
[ Color index : Important | Notes | Extra ] Editing file link Introduction to the Orthopedics Objectives: ★ To explain what Orthopedic is and what conditions will be discussed during this course ★ Explain what we mean by Red Flags ★ List the different causes of orthopedic disease. ★ Describe some of clinical examination tests ★ Introduce titles of Clinical Skills which will be taught during this course. Done by: Rana Albarrak & Lamya Alsaghan Edited By: Bedoor Julaidan Revised by: Dalal Alhuzaimi References: slides + Toronto notes + 433 team + 435 team group A Introduction Orthopedic specialty: ★ Branch of surgery concerned with conditions involving the musculoskeletal system. Orthopedic surgeons use both surgical and nonsurgical means to treat musculoskeletal trauma, spine diseases, sports injuries, degenerative diseases, infections, tumors, and congenital disorders. ★ It includes: bones, muscles, tendons, ligaments, joints, peripheral nerves (peripheral neuropathy of hand and foot), , vertebral column, spinal cord and its nerves. NOT only bones. ★ Subspecialties: General, pediatric, sport and reconstructive (commonly ACL “anterior cruciate ligament” injury), trauma, arthroplasty, spinal surgery, foot and ankle surgery, oncology, hand surgery (usually it is a mixed speciality depending on the center. Orthopedics = up to the wrist joint. Orthopedics OR plastic surgery = from carpal bones and beyond, upper limb (new) elbow & shoulder. will be discussed in details in a separate lectures Red Flags: ★ Red Flags = warning symptoms or signs = necessity for urgent or different action/intervention. ★ Should always be looked for and remembered. you have to rule out red flags with all emergency cases! Fever is NOT a red flag! Do not confuse medicine with ortho. Post-op day 1 fever is considered normal! ★ There are 5 main red flags: 1. -

Radioulnar Fusion for Forearm Defects in Children – a Salvage Procedure MN Rasool Department of Orthopaedics, Nelson R Mandela School of Medicine, Kwazulu-Natal
CLINICAL ARTICLE SA ORTHOPAEDIC JOURNAL Summer 2008 / Page 60 C LINICAL A RTICLE Radioulnar fusion for forearm defects in children – a salvage procedure MN Rasool Department of Orthopaedics, Nelson R Mandela School of Medicine, KwaZulu-Natal Reprint requests: Mr MN Rasool Department of Orthopaedics Faculty of Medicine Nelson R Mandela School of Medicine Private Bag X Congella 4013 Tel: (27) 031 260-4297 Fax: (27) 031 260-4518 E-mail: [email protected] Abstract Eight children aged 1-14 yrs with defects in the forearm were treated with the one-bone forearm procedure and followed up for 1-11 yrs. The defects were due to pyogenic osteomyelitis (n=3), osteochondroma (n=3), neurofibromatosis (n=1) and ulnar dysmelia (n=1). The radius was fixed to the ulna shaft with an intramedullary pin in six cases, and two children had centralisation of the radial metaphysis onto the ulna for “radial club hand” type deformity with Kirschner wires. All forearms united in 3-6 months. Shortening ranged from 1-10 cm. Fixed flexion deformity of the elbow (20°) resulted in one child and cubitus valgus (20°) occurred in another. One child had a radial articular tilt of 45°. The procedure achieved stability at the wrist and elbow. There was cosmetic and functional improvement in all patients. Introduction loss of elbow rotation. Rotation at the shoulder compen- 1-3 The treatment of forearm defects in children is challeng- sates for this adequately. Correction of the deviation of ing. When one growing forearm bone is destroyed by dis- the hand on a solid forearm gives a much stronger grip, ease, develops imperfectly or abnormally, secondary and improves elbow and wrist movements. -

Anatomy, Physical Examination and Imaging of Thoracic and Lumbosacral Spine
Anatomy, Physical Examination and Imaging of Thoracic and Lumbosacral Spine NGUYỄN THÀNH NHÂN LEARNING OBJECTIVES Understand: * Basic anatomy of the spine * Thoracic and Lumbar spine anatomy Understand basic imaging of X ray, CT Scan and MRI Identify and assess functions of the structures in clinical aspect: * Identify structures: inspection, palpation * Assess: Thoracic - Lumbar spine movements Understand: dermatomes, * SLR test, Bragard’s test, Neri’s test, … CONTENT Basic anatomy of the spine Thoracic - Lumbosacral spine anatomy Imaging of Thoracic - Lumbar spine Physical examination of Thoracic and Lumbar spine Anatomy Basic anatomy of the spine - The vertebral column consists of 33 vertebrae, - 5 segments: cervical, thoracic, lumbar, sacral, and coccygeal. - There are 7 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 4 coccygeal vertebrae. - The two major exceptions are C1 (atlas) and C2 (axis) - Atlantoaxial joint - cervical rotation Anatomy Basic anatomy of the spine [1] Anatomy Basic anatomy of the spine [1] Anatomy Basic anatomy of the spine - The spinal cord - Conus medullaris: L1 - L2 - There are 8 cervical, 12 thoracic, 5 lumbar, and 5 sacral pairs, and 1 coccygeal pair of spinal nerves. - The sacral spinal nerves make up the cauda equina The neural anatomy is such that the spinal cord resides within the bony canal between C1 and L1 and/or L2. The filum terminale extends from the conus and attaches to the coccyx.[1] Anatomy Basic neurology of the spine - Gray matter + Spinal neurons (lower motor neurons), + Interneurons