Malunion of Long Bones
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Loss of Correction in Cubitus Varus Deformity After Osteotomy
Loss of correction in cubitus varus deformity after osteotomy Chao You Shenzhen children's hospital Yibiao Zhou Shenzhen children's hospital https://orcid.org/0000-0001-9754-1089 Jingming Han ( [email protected] ) Research article Keywords: cubitus varus osteotomy Loss of correction Posted Date: May 5th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-26279/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/14 Abstract Purpose Cubitus varus deformity in the pediatric population is an infrequent but clinically important disease to orthopedic surgeons. Since these patient populations are different in many respects, we sought out to investigate the rates of loss of correction over time as well as the factors associated with loss of correction in pediatric patients undergoing osteotomy for treatment of cubitus varus deformity. Methods Between 2008-7 and 2017-7, we treated 30 cases of cubital varus had underwent the the osteotomy. We compared preoperative and postoperative clinical and imaging parameters (H-cobb angle,Baumman angle) for all patients. Postoperative evaluation was performed by telephone interview. Results In our study,there were 30 patients,included 17 males and 13 females.the mean age was 75 months old.In the rst follow-up,Approximately 80 % of patients had a loss of correction of H-cobband 83% of patients at the second follow-up. The Baumann angle also had a loss of correction,about 57% was lost at the rst follow-up,and 43% was lost at the second follow-up. The average interval between the rst follow-up and the second follow-up was 24 days The H-cobb angle mean loss was 2.4°.There was a statistically signicant difference between the H-cobb angle measured before surgery and the angle measured after surgery (p <0.05). -

Peds Ortho: What Is Normal, What Is Not, and When to Refer
Peds Ortho: What is normal, what is not, and when to refer Future of Pedatrics June 10, 2015 Matthew E. Oetgen Benjamin D. Martin Division of Orthopaedic Surgery AGENDA • Definitions • Lower Extremity Deformity • Spinal Alignment • Back Pain LOWER EXTREMITY ALIGNMENT DEFINITIONS coxa = hip genu = knee cubitus = elbow pes = foot varus valgus “bow-legged” “knock-knee” apex away from midline apex toward midline normal varus hip (coxa vara) varus humerus valgus ankle valgus hip (coxa valga) Genu varum (bow-legged) Genu valgum (knock knee) bow legs and in toeing often together Normal Limb alignment NORMAL < 2 yo physiologic = reassurance, reevaluate @ 2 yo Bow legged 7° knock knee normal Knock knee physiologic = reassurance, reevaluate in future 4 yo abnormal 10 13 yo abnormal + pain 11 Follow-up is essential! 12 Intoeing 1. Femoral anteversion 2. Tibial torsion 3. Metatarsus adductus MOST LIKELY PHYSIOLOGIC AND WILL RESOLVE! BRACES ARE HISTORY! Femoral Anteversion “W” sitters Internal rotation >> External rotation knee caps point in MOST LIKELY PHYSIOLOGIC AND MAY RESOLVE! Internal Tibial Torsion Thigh foot angle MOST LIKELY PHYSIOLOGIC AND WILL RESOLVE BY SCHOOL AGE Foot is rotated inward Internal Tibial Torsion (Fuchs 1996) Metatarsus Adductus • Flexible = correctible • Observe vs. casting CURVED LATERAL BORDER toes point in NOT TO BE CONFUSED WITH… Clubfoot talipes equinovarus adductus internal varus rotation equinus CAN’T DORSIFLEX cavus Clubfoot START19 CASTING JUST AFTER BIRTH Calcaneovalgus Foot • Intrauterine positioning • Resolve -
Efficacy and Safety of a Novel Personalized Navigation Template in Proximal Femoral Corrective Osteotomy for the Treatment of DDH Qiang Shi1,2 and Deyi Sun1*
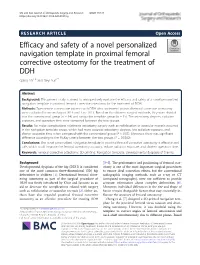
Shi and Sun Journal of Orthopaedic Surgery and Research (2020) 15:317 https://doi.org/10.1186/s13018-020-01843-y RESEARCH ARTICLE Open Access Efficacy and safety of a novel personalized navigation template in proximal femoral corrective osteotomy for the treatment of DDH Qiang Shi1,2 and Deyi Sun1* Abstract Background: This present study is aimed to retrospectively evaluate the efficacy and safety of a novel personalized navigation template in proximal femoral corrective osteotomy for the treatment of DDH. Methods: Twenty-nine consecutive patients with DDH who underwent proximal femoral corrective osteotomy were evaluated between August 2013 and June 2017. Based on the different surgical methods, they were divided into the conventional group (n = 14) and navigation template group (n = 15). The osteotomy degrees, radiation exposure, and operation time were compared between the two groups. Results: No major complications relating to osteotomy surgery such as redislocation or avascular necrosis occurred in the navigation template group, which had more accurate osteotomy degrees, less radiation exposure, and shorter operation time when compared with the conventional group (P < 0.05). Moreover, there was significant difference according to the McKay criteria between the two groups (P = 0.0362). Conclusions: The novel personalized navigation template in proximal femoral corrective osteotomy is effective and safe, which could improve the femoral osteotomy accuracy, reduce radiation exposure, and shorten operation time. Keywords: Femoral corrective osteotomy, 3D printing, Navigation template, Developmental dysplasia of the hip Background [3–5]. The performance and positioning of femoral oste- Developmental dysplasia of the hip (DDH) is considered otomy is one of the most important surgical procedures one of the most common three-dimensional (3D) hip to ensure ideal correction effects, but the conventional deformities in children [1]. -
1 Tips7pp P654-660CR2.Indd
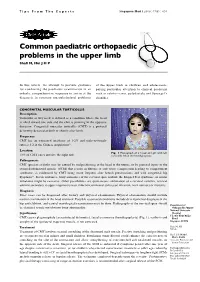
Tips From The Experts SingaporeSingapore Med Med J 2006; J 2006; 47(8) 47(8) : 654 : 1 Common paediatric orthopaedic problems in the upper limb Shafi M, Hui J H P In this article, we attempt to provide guidance of the upper limb in children and adolescents, for conducting the paediatric examination in an paying particular attention to clinical problems orderly, comprehensive sequence to arrive at the such as cubitus varus, polydactyly and Sprengel’s diagnosis in common musculoskeletal problems shoulder. CONGENITAL MUSCULAR TORTICOLLIS Description Torticollis or wry neck is defined as a condition where the head is tilted toward one side and the chin is pointing in the opposite direction. Congenital muscular torticollis (CMT) is a postural deformity detected at birth or shortly after birth. Frequency CMT has an estimated incidence of 1-2% and male-to-female ratio is 3:2 in the Chinese population(1). Location Fig. 1 Photograph of a 3-year-old girl with left 75% of CMT cases involve the right side. torticollis. Note the hemihypoplasia. Pathogenesis CMT (present at birth) may be caused by malpositioning of the head in the uterus, or by prenatal injury to the sternocleidomastoid muscle (SCM) that results in fibrosis or soft tissue compression leading to compartment syndrome, as evidenced by CMT being more frequent after breech presentations and with congenital hip dysplasia(2). In rare instances, bony anomalies of the cervical spine include the Klippel-Feil syndrome, or ocular imbalance might be causative. Other possibilities are spontaneous subluxation of a cervical vertebra, cervical adenitis secondary to upper respiratory tract infection, unilateral soft tissue infection, neck tumours or myositis. -

Mackenzie's Mission Gene & Condition List
Mackenzie’s Mission Gene & Condition List What conditions are being screened for in Mackenzie’s Mission? Genetic carrier screening offered through this research study has been carefully developed. It is focused on providing people with information about their chance of having children with a severe genetic condition occurring in childhood. The screening is designed to provide genetic information that is relevant and useful, and to minimise uncertain and unclear information. How the conditions and genes are selected The Mackenzie’s Mission reproductive genetic carrier screen currently includes approximately 1300 genes which are associated with about 750 conditions. The reason there are fewer conditions than genes is that some genetic conditions can be caused by changes in more than one gene. The gene list is reviewed regularly. To select the conditions and genes to be screened, a committee comprised of experts in genetics and screening was established including: clinical geneticists, genetic scientists, a genetic pathologist, genetic counsellors, an ethicist and a parent of a child with a genetic condition. The following criteria were developed and are used to select the genes to be included: • Screening the gene is technically possible using currently available technology • The gene is known to cause a genetic condition • The condition affects people in childhood • The condition has a serious impact on a person’s quality of life and/or is life-limiting o For many of the conditions there is no treatment or the treatment is very burdensome for the child and their family. For some conditions very early diagnosis and treatment can make a difference for the child. -

Congenital Abnormalities of the Femur
Arch Dis Child: first published as 10.1136/adc.36.188.410 on 1 August 1961. Downloaded from CONGENITAL ABNORMALITIES OF THE FEMUR BY P. A. RING From the Royal College of Surgeons (RECEIVED FOR PUBLICATION NOVEMBER 25, 1960) Congenital defects of the femur vary from simple tion of its incidence is difficult to obtain, but it hypoplasia of the bone to complete absence. appears to be the commonest congenital defect Classification of these defects has been suggested causing major abnormalities of limb growth. by Nilsonne (1928) and by Mouchet and Ibos (1928), but neither has met with general acceptance. In more recent years Golding (1939, 1948) has demon- Clinical Features strated the close association of the short femur with There is no evidence that this is a familial disorder, congenital coxa vara, and has emphasized that and careful inquiry of the parents has revealed no these are variations of the same underlying abnor- evidence of other congenital disorders within the mality. The clinical distinction between the various immediate family. The history of the pregnancy types of femoral defect is important as a guide to and delivery has failed to indicate any significant the prognosis of limb development. infection or abnormality at this time. In most From an examination of patients with congenital patients the abnormality is apparent at birth, but abnormalities of the femur the following classifica- where the inequality of leg length is slight, the by copyright. tion is suggested: diagnosis may not be made until the child begins to 1. Simple femoral hypoplasia. walk. To ordinary clinical testing the abnormality 2. -

Common Lower Extremity Problems in Children Susan A
Article orthopedics Common Lower Extremity Problems in Children Susan A. Scherl, MD* Objectives After completing this article, readers should be able to: 1. Describe the presentation of hip joint pathology in children. 2. Know how to treat most rotational and angular deformities. 3. Describe the hallmark of clubfoot that helps to differentiate it from isolated metatarsus adductus. 4. Explain why screening for developmental dysplasia of the hip should be performed. 5. Describe foot problems that can be markers for a neurologic disorder. Overview Growing children are susceptible to a variety of developmental lower extremity disorders of varying degrees of seriousness. Because children are growing and developing and are not simply smaller versions of adults, it can be difficult to treat some conditions, but in other cases, there is leeway in the results of treatment not available to adults. Long-term outcome is of utmost importance for pediatric patients because their bones, joints, and muscles optimally should remain functional and pain-free during childhood and throughout their lives. Treatment should disrupt daily life as little as possible to minimize the social and psychological toll of the illness. Common lower extremity problems in children can be grouped broadly into four categories: rotational deformities, angular deformities, foot deformities, and hip disorders. This article covers the major conditions in each group. Pediatricians and other primary care clinicians can expect to encounter these disorders in their practices. A working knowledge of the basics of these disorders will help in appropriate diagnosis, treatment, counseling, and referral of patients. Rotational Deformities The developmental rotational deformities, intoeing and outtoeing, probably are the most common childhood musculoskeletal entities that prompt parents to consult a physician. -

“NEONATOLOGY ORTHOPAEDICS” Alvin H
GROWTH AND EARLY DEVELOPMENT OF THE MUSCULOSKELETAL SYSTEM “NEONATOLOGY ORTHOPAEDICS” Alvin H. Crawford, M.D., F.A.C.S. MUSCULOSKELETAL NEONATOLOGY 1. Malformation * localized area of morphogenesis – cleft lip 2. Deformation *alteration of structure kyphoscoliotic tibia 3. Disruptive defects *structural defect of normal part B.E. amputation PRENATAL Defect in formation single/multiple POSTNATAL u Normal structure Genetics/CNS Environmental, trauma, infection, hypoxia, metabolic Unknown DEFORMATION u Extrinsic – constraining forces • Uterine – additional fetus • Bicornuate • Fibroids u Tight muscles – Primip u Bony lumbar spine u Small pelvis u Fetal posture u Position of comfort – (postnatally) NEONATE EXTREMITIES u Deformation u Disruptive defects u Position Fixed mobile u Malformation VARIABLES u Size Paternal age ??? u Parity Multiple births u Hydramnios Breech u Rupture Uterine abnormalities URGENT PROBLEMS u Infection (femoral, umbilical hernia, septic arthritis, osteomyelitis, complication u Gangrene (IV’s cut down) u Avascular bands u Skin closure (myelos) CONGENITAL PROBLEMS OF SOFT TISSUE u Arthrogryposis u Congenital contractural arachnodactyly u Marfans syndrome u Ehlers Danlos syndrome u Hemihypertrophy u Popliteal pterygium syndrome u Muscle diseases u Malignant neoplasms DEFORMITIES OF UPPER EXTREMITY u Shoulder u Classification of congenital malformations u Elbow and forearm u Hand and finger deformities u Thumb DEFORMITIES OF THE HIP AND PROXIMAL FEMUR u PFFD u Developmental dislocation of the hip u Extrophy of the -

Expanded Indications for Guided Growth in Pediatric Extremities
Current Concept Review Expanded Indications for Guided Growth in Pediatric Extremities Teresa Cappello, MD Shriners Hospitals for Children, Chicago, IL Abstract: Guided growth for coronal plane knee deformity has successfully historically been utilized for knee val- gus and knee varus. More recent use of this technique has expanded its indications to correct other lower and upper extremity deformities such as hallux valgus, hindfoot calcaneus, ankle valgus and equinus, rotational abnormalities of the lower extremity, knee flexion, coxa valga, and distal radius deformity. Guiding the growth of the extremity can be successful and is a low morbidity method for correcting deformity and should be considered early in the treatment of these conditions when the child has a minimum of 2 years of growth remaining. Further expansion of the application of this concept in the treatment of pediatric limb deformities should be considered. Key Concepts: • Guiding the growth of pediatric physes can successfully correct a variety of angular and potentially rotational deformities of the extremities. • Guided growth can be performed using a variety of techniques, from permanent partial epiphysiodesis to tem- porary methods utilizing staples, screws, or plate and screw constructs. • Utilizing the potential of growth in the pediatric population, guided growth principals have even been success- fully applied to correct deformities such as knee flexion contractures, hip dysplasia, femoral anteversion, ankle deformities, hallux valgus, and distal radius deformity. Introduction Guiding the growth of pediatric orthopaedic deformities other indications and uses for guided growth that may is represented by the symbol of orthopaedics itself, as not have wide appreciation. the growth of a tree is guided as it is tethered to a post (Figure 1). -

Anatomy, Physical Examination and Imaging of Thoracic and Lumbosacral Spine
Anatomy, Physical Examination and Imaging of Thoracic and Lumbosacral Spine NGUYỄN THÀNH NHÂN LEARNING OBJECTIVES Understand: * Basic anatomy of the spine * Thoracic and Lumbar spine anatomy Understand basic imaging of X ray, CT Scan and MRI Identify and assess functions of the structures in clinical aspect: * Identify structures: inspection, palpation * Assess: Thoracic - Lumbar spine movements Understand: dermatomes, * SLR test, Bragard’s test, Neri’s test, … CONTENT Basic anatomy of the spine Thoracic - Lumbosacral spine anatomy Imaging of Thoracic - Lumbar spine Physical examination of Thoracic and Lumbar spine Anatomy Basic anatomy of the spine - The vertebral column consists of 33 vertebrae, - 5 segments: cervical, thoracic, lumbar, sacral, and coccygeal. - There are 7 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 4 coccygeal vertebrae. - The two major exceptions are C1 (atlas) and C2 (axis) - Atlantoaxial joint - cervical rotation Anatomy Basic anatomy of the spine [1] Anatomy Basic anatomy of the spine [1] Anatomy Basic anatomy of the spine - The spinal cord - Conus medullaris: L1 - L2 - There are 8 cervical, 12 thoracic, 5 lumbar, and 5 sacral pairs, and 1 coccygeal pair of spinal nerves. - The sacral spinal nerves make up the cauda equina The neural anatomy is such that the spinal cord resides within the bony canal between C1 and L1 and/or L2. The filum terminale extends from the conus and attaches to the coccyx.[1] Anatomy Basic neurology of the spine - Gray matter + Spinal neurons (lower motor neurons), + Interneurons -

Mortier Group, Acrocapitofemoral Clinical
201 LETTER TO JMG Acrocapitofemoral dysplasia: an autosomal recessive skeletal dysplasia with cone shaped epiphyses in the hands and hips G R Mortier,PPGKramer, A Giedion, F A Beemer ............................................................................................................................. J Med Genet 2003;40:201–207 enetic disorders of the skeleton or skeletal dysplasias uncomplicated and the delivery uneventful. Around the age of are a clinically diverse and genetically heterogeneous 7 years, short stature was noted. She had normal psychomotor group of connective tissue disorders affecting skeletal development but experienced emotional problems related to G 1–4 morphogenesis and development. More than 200 different her short stature. The parents are healthy but consanguineous entities have been described.5 Despite the growing availability of molecular testing for several of these disorders, the diagno- sis of a skeletal dysplasia still relies primarily on a thorough clinical and radiographic study of the patient.6 Some particu- lar radiographic signs can be very helpful in establishing the diagnosis. One such example is the presence of cone shaped epiphyses.7 In most instances, cone shaped epiphyses repre- sent the initial stage of premature epimetaphyseal fusion resulting in growth arrest and shortening of the bone involved. Analysis of the site and shape of cone shaped epiphyses, in particular of the phalanges, can be helpful in the diagnosis of skeletal dysplasias.8–10 Based on the observation of four patients, we delineate a new skeletal dysplasia with autosomal recessive inheritance. Because all cases show cone shaped epiphyses in the hands and a radiographically characteristic involvement of the proximal femoral epiphyses, we propose naming this condi- tion acrocapitofemoral dysplasia. -

Synophyrs, Curly Eyelashes and Ptyrigium Colli in A
Open Access Case report Synophyrs, curly eyelashes and Ptyrigium colli in a girl with Desbuquois dysplasia: a case report and review of the literature Ali Al Kaissi1,2*, Klaus Klaushofer1 and Franz Grill2 Addresses: 1Ludwig Boltzmann Institute of Osteology, at the Hanusch Hospital of WGKK and, AUVA Trauma Centre Meidling, 4th Medical Department, A-1140 Vienna, Heinrich Collin-Str. 30, Vienna 2Orthopaedic Hospital of Speising, Paediatric Department, A-1130 Vienna, Speisinger Str. 109, Austria Email: AAK* - [email protected]; KK - [email protected]; FG - [email protected] * Corresponding author Received: 19 May 2009 Accepted: 2 September 2009 Published: 16 September 2009 Cases Journal 2009, 2:7873 doi: 10.4076/1757-1626-2-7873 This article is available from: http://casesjournal.com/casesjournal/article/view/7873 © 2009 Al Kaissi et al.; licensee Cases Network Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Introduction: Desbuquois dysplasia is a rare, but well described syndrome with remarkable clinical and radiographic variability ranging from mild skeletal involvement with normal intelligence to those with early fatal outcome. Case presentation: Distinctive radiographic features of Desbuquois dysplasia-typical hand type have been documented in a 3-year-old girl. Synophyrs, curly eyelashes and ptyrigium colli were additional findings. Conclusion: The phenotypic variability of Desbuquois syndrome might be an element of diagnostic confusion. However, distinctive radiographic features should urgently requiring attention and are virtually diagnostic.