Psychosocial Intervention for Earthquake Survivors
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PROPOSED HYDROELECTRIC PROJECT TAMAKOSHI 3 (TA3) August 2009 1
Information Brochure 01 PROPOSED HYDROELECTRIC PROJECT TAMAKOSHI 3 (TA3) August 2009 1 Information on the Proposed Tamakoshi 3 (TA3) Hydroelectric Project The Proponent/Developer for the project with new boundaries between SN Power is a growing international renewable Tamakoshi-Singati confl uence, and about 100 m energy company with projects in Asia, Latin upstream of the Tamakoshi bridge, at Kirnetar America and Africa. SN Power is a long-term was obtained on March 6th 2009. The TA-2 and industrial investor and is committed to social TA-3 projects have now been combined into one, and environmental sustainability throughout its i.e. the Tamakoshi 3 (TA3). The installed capacity business. The company’s current portfolio includes of the amended licence is 600 MW. hydropower projects in Nepal (Khimti Hydropower TA3 Project is located in Dolakha and Ramechhap Plant), India, the Phillipines, Sri Lanka, Chile, Peru districts. The proposed project will utilize the and Brazil. SN Power was established in 2002 fl ow of Tamakoshi River to generate electricity as a Norwegian limited company owned by by diverting the river at Betane and discharging Stratkraft, Norway’s largest utility company, and the water back into the river near Kirnetar. The Norfund, Norwegian state’s investment fund for project is under the optimization process and private companies in developing countries. In the various options are under evaluation. course of seven years, SN Power has established a strong platform for long-term growth. SN Power The project is a Peak Run-of-River (PROR) type is headquartered in Oslo, Norway. project. It is proposed to build a 102 m high dam near Betane to create a reservoir. -

Nepal Electricity Authority
NEPAL ELECTRICITY AUTHORITY ENVIRONMENTAL AND SOCIALMANAGEMENT PLAN OF SUPPLY AND INSTALLATION OF DISTRIBUTION PROJECTS (33KV TRANSMISSION LINE) UNDER THE GRID SOLAR AND ENERGY EFFICIECY PROJECT VOLUME II Prepared and Submitted by: Environment and Social Studies Department Kharipati, Bhaktapur Phone No.: 01-6611580, Fax: 01-6611590 Email: [email protected] September, 2018 SIDP Abbreviations and Acronyms ABBREVIATIONS AND ACRONYMS BS : Bikram Sambat (Nepali Era) DADO : District Agriculture Development Office DCC : District Coordination Committee DFO : District Forest Office DoED : Department of Electricity Development ESMF : Environment and Social Management Framework ESMP : Environment and Social Management Plan EPR : Environment Protection Rules, 1997 ESSD : Environment and Social Studies Department GoN : Government of Nepal GSEEP : Grid Tied and Solar Energy Efficiency Project GRC : Grievance Redress Cell GRM : Grievance Redress Mechanism HHs : Households IEE : Initial Environmental Examination MoEWRI : Ministry of Energy, Water Resource and Irrigation MoFE : Ministry of Forest and Environment NEA : Nepal Electricity Authority PAS : Project Affected Settlement PMO : Project Management Office SIDP : Supply and Installation of Distribution Project WB : World Bank Units ha : Hectare km : Kilometer kV : Kilo Volt m2 : Square meter ESMP Report i NEA-ESSD SIDP Table of Contents Table of Contents ABBREVIATIONS AND ACRONYMS ........................................................................................ I 1 INTRODUCTION ............................................................................................................ -
Detailed Project Report
1 Government of Nepal Ministry of Federal Affairs and Local Development Central Level Project Implementation Unit Earthquake Emergency Assistance Project Lalitpur, Nepal Earthquake Emergency Assistance Project (ADB Loan 3260-NEP) Detailed Project Report Devitar – Phulasipokhari Section of Devitar – Doramba – Paseban - Kolibagar Road CH: 0+000 – 16+140.40 Km Ramechhap Section II: Detail Engineering Survey, Design and Estimate Volume 1: Main Report (Final) August 2016 Prepared by: Joint Venture of Gaurav Integrated Development Associates Nepal P. Ltd, NEST (P) Ltd. and JAARSA Engineering Consultancy (P) Ltd, Kathmandu, Nepal on behalf of AF-Iteco Ltd. Switzerland ACKNOWLEDGEMENT Gaurav Integrated Development Associates Nepal (P) Ltd/NEST (P) Ltd/Jaarsa Engineering Consultancy (P) Ltd. JV, the Consultant would like to extend its gratitude to Decentralized Rural Infrastructure and Livelihood Project – Additional Financing (DRILP-AF), Central Implementation Support Consultant (CISC), Ekantakuna, Lalitpur, Nepal for providing an opportunity of Preparation of Detailed Project Reports for Rehabilitation and Reconstruction of Devitar – Phulasipokhari Section of Devitar – Doramba – Paseban – Kolibagar Road, Ramechhap. Also, we would like to acknowledge all the members of CISC for their kind co-operation. We would further like to acknowledge DDG, SDE of DoLIDAR, Mr. Vijaya Muni Bajracharya, DTO, Er. Dilli Raj Adhikari of DDC Ramechhap, CISC team, Engineer Saroj Acharya DTO,, Sub Engineer, the local people of the project area and all the individuals involved in with this project for their kind co-operation and help at every step during the preparation of this report. Last but not least, team would like to thank technical and supporting staffs of Gaurav Integrated Development Associates Nepal (P) Ltd/NEST (P) Ltd/Jaarsa Engineering Consultancy (P) Ltd. -

Download Document
Gold standard for the global goals Monitoring report June 2017, version 1 Page 1 of 40 Title of the project Smokeless Cook Stoves for Rural Districts of Nepal Gold Standard project id GS 1191 Version number of the monitoring report 3 Completion date of the monitoring report 15/06/2020 Date of project design certification 01/01/2014 Start date of crediting period 01/01/2013 Duration of this monitoring period Period 3 from 01/05/2018 to 31/07/2019 Duration of previous monitoring period Period 2 from 01/04/2014 to 25/04/2015 Project representative(s) Dr. Reinhard Hallermayer, “Die Ofenmacher e.V.”, Germany Anita Badal, Swastha Chulo Nepal Host Country Nepal Certification pathway (activity certification/impact certification) Impact Statements & Products (VER Project Certification) SDG Contributions targeted (as per 1 – Climate Action (SDG 13) approved PDD) 2 - Good health and well-being (SDG 3) 3 - Affordable and Clean Energy (SDG 7) 4 – Gender Equality (SDG 5) Gold Standard statement/product certification sought GS VER (GSVER/ADALYs/RECs etc.) Selected methodology(ies) AMS II. G., version 3 Estimated amount of annual average SDG 13: 7,648 tonnes CO2 certified SDG impact (as per approved PDD) SDG 3: 8,503 ICS SDG 7: 8,503 ICS SDG 5: 0 women Total amount of certified SDG impact (as SDG 13: 6,696 tonnes CO2 per approved methodology) achieved in this SDG 3: 8,537 ICS monitoring period SDG 7: 8,537 ICS SDG 5: 7 women Page 2 of 40 SECTION A. Description of project A.1. Purpose and general description of project The objective of the project is the installation of mud brick cook stoves in individual households in three rural districts of Nepal in order to substitute the traditional fireplaces for cooking without discharge of the smoke into the environment. -
Ramechhap HRRP General Coordination Meeting,11Th Dec 2018
HRRP District Coordination Meeting Minutes Meeting Purpose: HRRP General Coordination Meeting Meeting Date: 11/12/2018 (11th Dec 2018) Meeting Time: 11am – 2pm Meeting Location: Devkota Chowk, Manthali DTO Meeting Hall, Ramechhap Meeting Facilitator: Prakash Bishwakarma Minutes Taken By: Prakash Bishwakarma / Javeed Mohamad Summary of Total: 16 Female:1 Male: 15 participants: Discussion: (Items/Knowledge Shared) GMaLi/HRRP Ramechhap General coordination meeting was chaired by Mr. Krishna lal Piya – GMALI Office Chief, Ramechhap and chief guest was Mr. Shanti prasad Paudel Provincial member of parliament province 3. Agenda: ➢ Welcome/Introduction ➢ Follow up of previous month’s meeting discussion and parking lot ➢ POs update – please share your update packs (PPT) so that can be shared in the meeting minute ➢ AOB Discussion ➢ Welcome and Introduction: Mr. Prakash Bishwakarma- District Coordinator- HRRP welcomed all the participants participated in the General coordination meeting and had a round of the introduction with each other. He also shared the objective and agenda of the General coordination meeting to be discussed in the meeting. ➢ HRRP updates: Mr. Prakash Bishwakarma- District coordinator have a presentation on What HRRP is doing and What HRRP is? Housing Recovery and Reconstruction Platform (HRRP) is working in Nepal to support Government of Nepal (NRA, MOUD/DUDBC, MOFALD) in coordination, Strategic planning, facilitating cooperation with the national and international organizations, the private sector, and public associations involve in recovery and reconstruction after Earthquake in Nepal. In the following ways HRRP Work. -General Coordination -Technical Coordination -Information Management o Collecting 5w data o Manage Training Database o Generate Maps ➢ Partners Update In Ramechhap District there are 6 partner’s organization are actively working in the district based on the reporting to GMALI/HRRP. -

Food Insecurity and Undernutrition in Nepal
SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics Acknowledgements The completion of both this and the earlier feasibility report follows extensive consultation with the National Planning Commission, Central Bureau of Statistics (CBS), World Food Programme (WFP), UNICEF, World Bank, and New ERA, together with members of the Statistics and Evidence for Policy, Planning and Results (SEPPR) working group from the International Development Partners Group (IDPG) and made up of people from Asian Development Bank (ADB), Department for International Development (DFID), United Nations Development Programme (UNDP), UNICEF and United States Agency for International Development (USAID), WFP, and the World Bank. WFP, UNICEF and the World Bank commissioned this research. The statistical analysis has been undertaken by Professor Stephen Haslett, Systemetrics Research Associates and Institute of Fundamental Sciences, Massey University, New Zealand and Associate Prof Geoffrey Jones, Dr. Maris Isidro and Alison Sefton of the Institute of Fundamental Sciences - Statistics, Massey University, New Zealand. We gratefully acknowledge the considerable assistance provided at all stages by the Central Bureau of Statistics. Special thanks to Bikash Bista, Rudra Suwal, Dilli Raj Joshi, Devendra Karanjit, Bed Dhakal, Lok Khatri and Pushpa Raj Paudel. See Appendix E for the full list of people consulted. First published: December 2014 Design and processed by: Print Communication, 4241355 ISBN: 978-9937-3000-976 Suggested citation: Haslett, S., Jones, G., Isidro, M., and Sefton, A. (2014) Small Area Estimation of Food Insecurity and Undernutrition in Nepal, Central Bureau of Statistics, National Planning Commissions Secretariat, World Food Programme, UNICEF and World Bank, Kathmandu, Nepal, December 2014. -
Early Recovery Cluster | Dolakha District
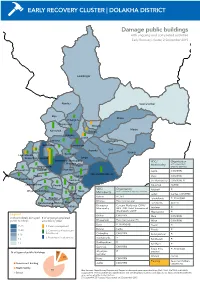
EARLY RECOVERY CLUSTER | DOLAKHA DISTRICT Damage public buildings with ongoing and completed activities Early Recovery cluster, 2 September 2015 Lamabagar Alambu Gaurishankar Bigu Khare Chilangkha Khopachagu Worang Marbu Kalinchok Bulung Babare Laduk Lapilang Changkhu Sundrawati Lamidanda Jhyanku Suri Syama Boch Sunkhani Lakuridanda Suspa Kshyamawati Jungu Bhimeswor Municipality VDC/ Organisation Chhetrapa Municipality with completed/ Magapauwa Kabre ongoing activities Bhusaphedi Katakuti Namdru Japhe CWV/RRN JIRI MUNICIPALITY Phasku Mirge Jhule CWV/RRN Dodhapokhari Gairimudi Jiri Municipality CWV/RRN, PI Bhirkot Sailungeshwar Pawati Kalinchok ACTED VDC/ Organisation Katakuti PI Ghyangsukathokar Jhule Hawa Municipality with completed/ongoing activities Japhe Laduk Caritas, CWV/RRN Babare ACTED Bhedpu Chyama Lakuridanda PI, RI/ANSAB Bhedpu Plan International Dandakharka Melung Malu Lamidanda ACTED Shahare Bhimeswor Concern Worldwide (CWV)/ Municipality RRN. IOM, Relief International Lapilang PI (RI)/ANSAB, UNDP Magapauwa PI Legend Bhirkot CWV/RRN Malu CWV/RRN # of completely damaged # of ongoing/completed public buildings activities by pillar Bhusaphedi Plan International (PI) Mirge CWV/RRN Boch PI, RI/ANSAB 21-28 1. Debris management Pawati PI Bulung Carita 11-20 2. Community infrastructure Phasku PI & livelihood 6-10 Chilangkha CWV/RRN Sailungeshwar PI 3. Restoration local services 3-5 Dandakharka PI Sundrawati PI Dodhapokhari PI 4% 1-2 Sunkhani PI Gairimudi CWV/RRN 12% Suspa Kshy- PI, RI/ANSAB Ghyangsu- PI amawati % of type of public buildngs 7% kathokar 14% Worang Caritas Hawa CWV/RRN Government building Planning Save the Children, Japhe CWV/RRN Government building Health facility UNDP/UNV Health facility School 79% Map Sources: Nepal Survey Department, Report on damaged government buildings, DoE, MoH, MoFALD and MoUD, 84% School August 2015. -
Map of Dolakha District Show Ing Proposed Vdcs for Survey
Annex 3.6 Annex 3.6 Map of Dolakha district showing proposed VDCs for survey Source: NARMA Inception Report A - 53 Annex 3.7 Annex 3.7 Summary of Periodic District Development Plans Outlay Districts Period Vision Objectives Priorities (Rs in 'ooo) Kavrepalanchok 2000/01- Protection of natural Qualitative change in social condition (i) Development of physical 7,021,441 2006/07 resources, health, of people in general and backward class infrastructure; education; (ii) Children education, agriculture (children, women, Dalit, neglected and and women; (iii) Agriculture; (iv) and tourism down trodden) and remote area people Natural heritage; (v) Health services; development in particular; Increase in agricultural (vi) Institutional development and and industrial production; Tourism and development management; (vii) infrastructure development; Proper Tourism; (viii) Industrial management and utilization of natural development; (ix) Development of resources. backward class and region; (x) Sports and culture Sindhuli Mahottari Ramechhap 2000/01 – Sustainable social, Integrated development in (i) Physical infrastructure (road, 2,131,888 2006/07 economic and socio-economic aspects; Overall electricity, communication), sustainable development of district by mobilizing alternative energy, residence and town development (Able, local resources; Development of human development, industry, mining and Prosperous and resources and information system; tourism; (ii) Education, culture and Civilized Capacity enhancement of local bodies sports; (III) Drinking -
VBST Short List
1 आिेदकको दर्ा ा न륍बर नागररकर्ा न륍बर नाम थायी जि쥍ला गा.वि.स. बािुको नाम ईभेꅍट ID 10002 2632 SUMAN BHATTARAI KATHMANDU KATHMANDU M.N.P. KEDAR PRASAD BHATTARAI 136880 10003 28733 KABIN PRAJAPATI BHAKTAPUR BHAKTAPUR N.P. SITA RAM PRAJAPATI 136882 10008 271060/7240/5583 SUDESH MANANDHAR KATHMANDU KATHMANDU M.N.P. SHREE KRISHNA MANANDHAR 136890 10011 9135 SAMERRR NAKARMI KATHMANDU KATHMANDU M.N.P. BASANTA KUMAR NAKARMI 136943 10014 407/11592 NANI MAYA BASNET DOLAKHA BHIMESWOR N.P. SHREE YAGA BAHADUR BASNET136951 10015 62032/450 USHA ADHIJARI KAVRE PANCHKHAL BHOLA NATH ADHIKARI 136952 10017 411001/71853 MANASH THAPA GULMI TAMGHAS KASHER BAHADUR THAPA 136954 10018 44874 RAJ KUMAR LAMICHHANE PARBAT TILAHAR KRISHNA BAHADUR LAMICHHANE136957 10021 711034/173 KESHAB RAJ BHATTA BAJHANG BANJH JANAK LAL BHATTA 136964 10023 1581 MANDEEP SHRESTHA SIRAHA SIRAHA N.P. KUMAR MAN SHRESTHA 136969 2 आिेदकको दर्ा ा न륍बर नागररकर्ा न륍बर नाम थायी जि쥍ला गा.वि.स. बािुको नाम ईभेꅍट ID 10024 283027/3 SHREE KRISHNA GHARTI LALITPUR GODAWARI DURGA BAHADUR GHARTI 136971 10025 60-01-71-00189 CHANDRA KAMI JUMLA PATARASI JAYA LAL KAMI 136974 10026 151086/205 PRABIN YADAV DHANUSHA MARCHAIJHITAKAIYA JAYA NARAYAN YADAV 136976 10030 1012/81328 SABINA NAGARKOTI KATHMANDU DAANCHHI HARI KRISHNA NAGARKOTI 136984 10032 1039/16713 BIRENDRA PRASAD GUPTABARA KARAIYA SAMBHU SHA KANU 136988 10033 28-01-71-05846 SURESH JOSHI LALITPUR LALITPUR U.M.N.P. RAJU JOSHI 136990 10034 331071/6889 BIJAYA PRASAD YADAV BARA RAUWAHI RAM YAKWAL PRASAD YADAV 136993 10036 071024/932 DIPENDRA BHUJEL DHANKUTA TANKHUWA LOCHAN BAHADUR BHUJEL 136996 10037 28-01-067-01720 SABIN K.C. -
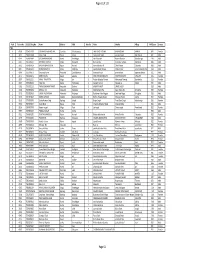
TSLC PMT Result
Page 62 of 132 Rank Token No SLC/SEE Reg No Name District Palika WardNo Father Mother Village PMTScore Gender TSLC 1 42060 7574O15075 SOBHA BOHARA BOHARA Darchula Rithachaupata 3 HARI SINGH BOHARA BIMA BOHARA AMKUR 890.1 Female 2 39231 7569013048 Sanju Singh Bajura Gotree 9 Gyanendra Singh Jansara Singh Manikanda 902.7 Male 3 40574 7559004049 LOGAJAN BHANDARI Humla ShreeNagar 1 Hari Bhandari Amani Bhandari Bhandari gau 907 Male 4 40374 6560016016 DHANRAJ TAMATA Mugu Dhainakot 8 Bali Tamata Puni kala Tamata Dalitbada 908.2 Male 5 36515 7569004014 BHUVAN BAHADUR BK Bajura Martadi 3 Karna bahadur bk Dhauli lawar Chaurata 908.5 Male 6 43877 6960005019 NANDA SINGH B K Mugu Kotdanda 9 Jaya bahadur tiruwa Muga tiruwa Luee kotdanda mugu 910.4 Male 7 40945 7535076072 Saroj raut kurmi Rautahat GarudaBairiya 7 biswanath raut pramila devi pipariya dostiya 911.3 Male 8 42712 7569023079 NISHA BUDHa Bajura Sappata 6 GAN BAHADUR BUDHA AABHARI BUDHA CHUDARI 911.4 Female 9 35970 7260012119 RAMU TAMATATA Mugu Seri 5 Padam Bahadur Tamata Manamata Tamata Bamkanda 912.6 Female 10 36673 7375025003 Akbar Od Baitadi Pancheswor 3 Ganesh ram od Kalawati od Kalauti 915.4 Male 11 40529 7335011133 PRAMOD KUMAR PANDIT Rautahat Dharhari 5 MISHRI PANDIT URMILA DEVI 915.8 Male 12 42683 7525055002 BIMALA RAI Nuwakot Madanpur 4 Man Bahadur Rai Gauri Maya Rai Ghodghad 915.9 Female 13 42758 7525055016 SABIN AALE MAGAR Nuwakot Madanpur 4 Raj Kumar Aale Magqar Devi Aale Magar Ghodghad 915.9 Male 14 42459 7217094014 SOBHA DHAKAL Dolakha GhangSukathokar 2 Bishnu Prasad Dhakal -

District Profile - Dolakha (As of 10 May 2017) HRRP
District Profile - Dolakha (as of 10 May 2017) HRRP This district profile outlines the current activities by partner organisations (POs) in post-earthquake recovery and reconstruction. It is based on 4W and secondary data collected from POs on their recent activities pertaining to housing sector. Further, it captures a wide range of planned, ongoing and completed activities within the HRRP framework. For additional information, please refer to the HRRP dashboard. FACTS AND FIGURES Population: 280,8741 48 VDCs and 2 municipalities Damage Status - Private Structures Type of housing walls Dolakha National Mud-bonded bricks/stone 92% 41% Cement-bonded bricks/stone 5% 29% Damage Grade (3-5) 56,293 Other 3% 30% Damage Grade (1-2) 4,346 % of households who own 94% 85% Total 60,6392 their housing unit (Census 2011)1 NEWS & UPDATES 1. NRA Dolakha is planning to do survey of buildings which were missed out or where people were not convinced by the previous survey. NRA is planning to use the same DLPIU Engineers for the survey. The start date is yet to be finalized because of the election. 2. Bhimeshwor Municipality ward 1 (new) Bosimpa has been identified as one major village to resettle and they are planning to resettle 82 HH to Panipokhari. This is also taken as major pilot resettlement project in Dolakha. HRRP Dolakha HRRP © PARTNERS SUMMARY AND HIGHLIGHTS3 Partner Organisation Implementing Partner(s) BC PLAN 2,338 1,645 CA CEEPAARD,HURADEC SHORT TRAINING CARITAS - L POURAKHI VOCATIONAL TRAINING 599 5,398 CARITAS-N (Targets Achieved) CW RRN -

Ttamak Koshi 3 Hyd Droel Ectric C Pro Oject
TAMAKOSHI 3 HYDROELECTRIC PROJECT EXECUTIVE SUMMARY - VOLUME XI Document for Disclosure Final Report – November 30, 2009 SWECO Norge AS Lysaker, P O Box 400 Oslo, NORWAY Telephone +47 67 12 80 00 www.sweco.no Abbreviations and Acronyms ACBP Awareness and Capacity Building Plan ADB Asian Development Bank CF Community Forest CFUG Community Forest User Group CITES Convention of International Trade in Endangered Species CSR Corporate Social Responsibility DFO District Forest Office DOED Department of Electricity Development EHSP Environment, Health and Safety Plan EIA Environmental Impact Assessment EMP Environmental Management Plan EMU Environmental Management Unit EPA Environmental Protection Agency EPR Environmental Protection Rules GLOF Glacial Lake Outburst Floods GON Government of Nepal GRU Grievance Redressal Unit GW Giga-watt GWh Giga-watt per hour HEP Hydroelectric Project HH/hh Household ICAMDP Immediate Catchment Area Management and Development Plan IFC International Financial Corporation IUCN International Union for the Conservation of Nature LSEP Livelihood Support and Enhancement Program m asl meters above sea level MOE Ministry of Energy MoEn Ministry of Environment MoWR Ministry of Water Resources MT Million Tons MW Mega Watt NEA National Electricity Authority PAF Project Affected Families PAP Project Affected Persons PCDP Public Consultation and Disclosure Plan PS Performance Standards RAP Resettlement Action Plan RRP Resettlement and Rehabilitation Plan SBA Safeguard Buffer Area SchEMS School of Environmental Management and Sustainable Development SEMD Social and Environmental Management Division SNP SN Power SPAF Severely Project Affected Families SPS Safeguard Policy Statement TA3HEP Tamakoshi 3 Hydroelectric Project TOR Terms of Reference VDC Village Development Committee WBG World Bank Group WHO World Health Organization Table of Content Page nos 1 Project Proponent and Organization Responsible for Preparing the EIA Report .........................................................