Eosinophil-Associated Processes Underlie Differences in Clinical
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pathway in the Thymus by a CD24-Dependent Autoreactive T
Autoreactive T Cells Escape Clonal Deletion in the Thymus by a CD24-Dependent Pathway This information is current as Joseph W. Carl, Jr., Jin-Qing Liu, Pramod S. Joshi, Hani Y. of September 27, 2021. El-Omrani, Lijie Yin, Xincheng Zheng, Caroline C. Whitacre, Yang Liu and Xue-Feng Bai J Immunol 2008; 181:320-328; ; doi: 10.4049/jimmunol.181.1.320 http://www.jimmunol.org/content/181/1/320 Downloaded from References This article cites 54 articles, 18 of which you can access for free at: http://www.jimmunol.org/content/181/1/320.full#ref-list-1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication by guest on September 27, 2021 *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2008 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Autoreactive T Cells Escape Clonal Deletion in the Thymus by a CD24-Dependent Pathway1 Joseph W. Carl, Jr.,* Jin-Qing Liu,* Pramod S. -

Natural Killer T Cells Are Required for the Development of a Superantigen-Driven T Helper Type 2 Immune Response in Mice
IMMUNOLOGY ORIGINAL ARTICLE Natural killer T cells are required for the development of a superantigen-driven T helper type 2 immune response in mice Auro Nomizo,1 Edilberto Postol,2 Summary Raquel de Alencar,2 Fabı´ola We show, here, that one single injection or weekly injections of staphylo- Cardillo2 and Jose´ Mengel2 coccal enterotoxin B (SEB), starting in 1-day-old newborn mice, induced 1Department of Clinical Analysis, Toxicology a powerful immune response with a T helper type 2 (Th2) pattern, as and Bromatology, Faculty of Pharmaceutical Sciences of Ribeira˜o Preto, University of Sa˜o judged by the isotype and cytokine profile, with the production of large Paulo, Ribeira˜o Preto, and 2Department of amounts of SEB-specific immunoglobulin G1 (IgG1), detectable levels of Immunology, Institute of Biomedical Sciences, SEB-specific IgE and increased production of interleukin-4 by spleen cells. University of Sa˜o Paulo, Sa˜o Paulo, SP, Brazil These protocols also induced an increase in the levels of total IgE in the serum. Memory of SEB was transferred to secondary recipients by using total spleen cells from primed animals. The secondary humoral response in transferred mice was diminished if spleen cells from SEB-treated mice were previously depleted of CD3+ or Vb8+ T cells or NK1.1+ cells. In vivo depletion of NK1.1+ cells in adult mice resulted in a marked reduction in the SEB-specific antibody response in both the primary and secondary doi:10.1111/j.1365-2567.2005.02215.x immune responses. Additionally, purified NK1.1+ T cells were able to per- Received 11 April 2005; revised 23 May 2005; form SEB-specific helper B-cell actions in vitro and in vivo. -
Of T Cell Tolerance
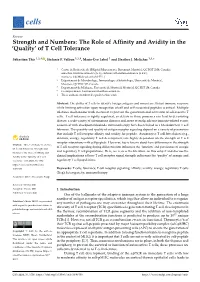
cells Review Strength and Numbers: The Role of Affinity and Avidity in the ‘Quality’ of T Cell Tolerance Sébastien This 1,2,† , Stefanie F. Valbon 1,2,†, Marie-Ève Lebel 1 and Heather J. Melichar 1,3,* 1 Centre de Recherche de l’Hôpital Maisonneuve-Rosemont, Montréal, QC H1T 2M4, Canada; [email protected] (S.T.); [email protected] (S.F.V.); [email protected] (M.-È.L.) 2 Département de Microbiologie, Immunologie et Infectiologie, Université de Montréal, Montréal, QC H3C 3J7, Canada 3 Département de Médecine, Université de Montréal, Montréal, QC H3T 1J4, Canada * Correspondence: [email protected] † These authors contributed equally to this work. Abstract: The ability of T cells to identify foreign antigens and mount an efficient immune response while limiting activation upon recognition of self and self-associated peptides is critical. Multiple tolerance mechanisms work in concert to prevent the generation and activation of self-reactive T cells. T cell tolerance is tightly regulated, as defects in these processes can lead to devastating disease; a wide variety of autoimmune diseases and, more recently, adverse immune-related events associated with checkpoint blockade immunotherapy have been linked to a breakdown in T cell tolerance. The quantity and quality of antigen receptor signaling depend on a variety of parameters that include T cell receptor affinity and avidity for peptide. Autoreactive T cell fate choices (e.g., deletion, anergy, regulatory T cell development) are highly dependent on the strength of T cell receptor interactions with self-peptide. However, less is known about how differences in the strength Citation: This, S.; Valbon, S.F.; Lebel, of T cell receptor signaling during differentiation influences the ‘function’ and persistence of anergic M.-È.; Melichar, H.J. -

Proapoptotic Protein Bim Is Differentially Required During Thymic Clonal Deletion to Ubiquitous Versus Tissue-Restricted Antigens
Proapoptotic protein Bim is differentially required during thymic clonal deletion to ubiquitous versus tissue-restricted antigens Alexander Y. W. Suen and Troy A. Baldwin1 Department of Medical Microbiology and Immunology, University of Alberta, Edmonton, AB, Canada T6G 2S2 Edited by Michael J. Bevan, University of Washington, Seattle, WA, and approved December 8, 2011 (received for review September 8, 2011) Positive and negative selection of thymocytes in the thymus are positively selected by high-affinity antigen encounter in the thy- critical for the development of a mature and self-tolerant T-cell mus (6). One such example are T-regulatory (Treg) cells, which repertoire. The proapoptotic Bcl-2 family member Bim is important are believed to require high-affinity interactions to develop in the for negative selection by inducing apoptosis in thymocytes receiv- medulla (7). It remains unknown what drives this distinction ing a strong signal through their antigen receptor. However, in the between negative selection and Treg development, although case of ubiquitous self-antigens (UbA), Bim is not required for the secondary signals, such as TGF-β, may play a role in overcoming clonal deletion of self-reactive thymocytes, suggesting the exis- cell death (8). tence of nonapoptotic clonal deletion mechanisms. Unlike UbA, Although it is unclear how the same TCR can transduce a sig- clonal deletion to tissue-restricted antigens (TRAs) requires posi- nal for positive or negative selection, differential mitogen-acti- tive selection and CCR7-mediated migration to the medulla. This vated protein kinase signaling appears to play a role, ultimately led us to hypothesize that Bim is required for the latter. -
T-Cell Tolerance by Prof. Anand Prakash
PROF. ANAND PRAKASH Department of Biotechnology Mahatma Gandhi Central University Motihari Bihar • Immature T-Cells enter in the thymus after differentiating in the bone marrow. • These T-cells undergo maturation and develop TCRs through Somatic Recombination. Bone Marrow Precursors of the T-Cells enter from Bone marrow to THYMUS thymus T Cell Maturation starts Expression of TCR s • DEVELOPMENT OF T-CELL RECEPTORS (TCRs) Some of T-Cells in the thymus develop receptors which are useless with no antigen specificity and while others develop TCRs with • specificity for self antigens and non-self antigens. Thymocytes having TCRs with low affinity for auto antigens, displayed in the MHC class I and II, undergo positive selection and further differentiate to become part of adaptive immunity, whereas the one with non-functional receptors die off because of • negligence. Clonal deletion of T-cells with useless TCRs and high affinity receptors along with clonal diversion for development of “Treg”, are the major processes operative in the thymus towards elimination or regulation of self-reactive T cells. INSIDE THE THYMUS THE T-CELLS UNDERGO AN ELABORATE SCREENING PROCEDURE3 THROUGH FOLLOWING MECHANISMS • • • T CELLS RECOGNIZE ANTIGEN DERIVED PEPTIDES PRESENTED BY MHC MOLECULES MHC Class II MHC Class I Antigen Infected or Presenting Tumour Cell Cell CD8 Peptide CD4 CD4+ CD8+ Helper Cell Cytotoxic T Cell T Cell Receptor T Cell Receptor T CELLS RECOGNIZE ANTIGEN DERIVED PEPTIDES PRESENTED BY MHC MOLECULES Inside Thymus THYMIC T -CELL FATE IS DETERMINED BY STRENGTH OF TCR-MHC/PEPTIDE INTERACTION Thymic MHC stromal Cell Thymic T Cell TCR + CD4 CD8 • NEGATIVE SELECTION Negative selection occurs at the Double positive stage in the thymic cortex, or at the Single Positive stage in the thymic medulla. -

Understanding the Immune System: How It Works
Understanding the Immune System How It Works U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES NATIONAL INSTITUTES OF HEALTH National Institute of Allergy and Infectious Diseases National Cancer Institute Understanding the Immune System How It Works U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES NATIONAL INSTITUTES OF HEALTH National Institute of Allergy and Infectious Diseases National Cancer Institute NIH Publication No. 03-5423 September 2003 www.niaid.nih.gov www.nci.nih.gov Contents 1 Introduction 2 Self and Nonself 3 The Structure of the Immune System 7 Immune Cells and Their Products 19 Mounting an Immune Response 24 Immunity: Natural and Acquired 28 Disorders of the Immune System 34 Immunology and Transplants 36 Immunity and Cancer 39 The Immune System and the Nervous System 40 Frontiers in Immunology 45 Summary 47 Glossary Introduction he immune system is a network of Tcells, tissues*, and organs that work together to defend the body against attacks by “foreign” invaders. These are primarily microbes (germs)—tiny, infection-causing Bacteria: organisms such as bacteria, viruses, streptococci parasites, and fungi. Because the human body provides an ideal environment for many microbes, they try to break in. It is the immune system’s job to keep them out or, failing that, to seek out and destroy them. Virus: When the immune system hits the wrong herpes virus target or is crippled, however, it can unleash a torrent of diseases, including allergy, arthritis, or AIDS. The immune system is amazingly complex. It can recognize and remember millions of Parasite: different enemies, and it can produce schistosome secretions and cells to match up with and wipe out each one of them. -

Clonal Deletion of Autoreactive B Lymphocytes in Bone Marrow
Proc. Nati. Acad. Sci. USA Vol. 86, pp. 8039-8043, October 1989 Immunology Clonal deletion of autoreactive B lymphocytes in bone marrow chimeras (immunological tolerance/transgenic mice/histocompatibility complex) DAVID NEMAZEE*t AND KURT BUERKIt *Basel Institute for Immunology, Postfach CH-4005, Basel, Switzerland; and tPrecinical Research, Sandoz, Ltd., CH-4002, Basel, Switzerland Communicated by Philippa Marrack, July 24, 1989 (receivedfor review June 17, 1989) ABSTRACT To study the fate of developing B cells in the mice that either did or did not bear the H-2k antigens to which presence and absence of the autoantigens to which they react, the transgenic antibody reacts (H-2Kk and H-2Dk). chimeric mice were constructed by ij'ecting bone marrow cells A potential difficulty with studying tolerance to H-2k in our from mice transgenic for rearranged immunoglobulin genes system with genetic crosses was that, because the B cells in encoding an anti-H-2Kk antibody into irradiated recipients that the tolerant animals also bore H-2 class I antigens, it was not did or did not express the H-2Kk antigen. In the presence of clear whether it was necessary for the H-2k antigens to be H-2Kk, the anti-H-2Kk-specific B cells were deleted from the coexpressed on the transgenic B cells themselves to achieve spleen and lymph nodes, whereas in its absence, anti-H-2Kk tolerance. In this report we describe the tolerance phenotype cells were abundant. B cells bearing a low level of membrane of irradiation bone marrow chimeras in which anti-H-2k immunoglobulin with the anti-H-2Kk idiotype were found in the transgenic B cells that lack the H-2k antigens develop in hosts bone marrows of H-2Kk recipients, suggesting that clonal that bear or do not bear H-2k antigens. -

Immune Regulation and Tolerance
Mechanisms of unresponsiveness: Immunological Ignorance Immune Regulation Normal response and Proliferation and Tolerance differentiation Mechanisms of Antigen/lymphocyte barrier unresponsiveness Mechanisms of Tissue abnormalities contributing to release and Yong-Rui Zou (Oct. 2005) autoimmunity presentation of self antigens. [email protected] Disease models Sympathetic ophthalmia, experimental allergic encephalomyelitis (EAE) Immunoregulation: A balance between activation and Mechanisms of unresponsiveness: suppression of effector cells to achieve an efficient Central tolerance in B and T cells (I): Clonal Deletion immune response without damaging the host. Self antigen presented in generative Activation (immunity) Suppression (tolerance) lymphoid Deletion of immature organs lymphocytes strongly recognizing self antigens autoimmunity immunodeficiency present in generative organs Lymphoid precursor Significance: The induction of tolerance may be Survival of clones which are only moderately exploited to prevent graft rejection, to treat autoimmune responsive to self antigens and allergic diseases, and to prevent immune responses present in generative in gene therapy. organs; forms T/B cell repertoire Important features of immunoregulation: 1. Antigen specific; affects T or B lymphocytes Science 298:1395 (2002) 2. Tolerance vs. activation? Determined by the nature of antigen and associated stimuli, and when and where the antigen is encountered Immunity 23:227 (2005) 1 Mechanisms of unresponsiveness: AIRE: Autoimmune regulator. Peripheral tolerance in B cells (I): Anergy Immunogenic signaling Tolerogenic signaling • Transcription factor. • Expressed at a high level by thymic medullar epithelium Acute Chronic cells. antigens antigens CD40L • Autosomal recessive mutation leads to autoimmune LPS polyendocrine syndrom - type 1 (APS-1). CD40 CD40 TLR4 • Inactivation of aire abolishes expression of some tissue TLR4 BCR BCR Fcγ2b specific genes in the thymic medulla. -

The Anatomy of T-Cell Activation and Tolerance Anna Mondino*T, Alexander Khoruts*, and Marc K
Proc. Natl. Acad. Sci. USA Vol. 93, pp. 2245-2252, March 1996 Review The anatomy of T-cell activation and tolerance Anna Mondino*t, Alexander Khoruts*, and Marc K. Jenkins Department of Microbiology and the Center for Immunology, University of Minnesota Medical School, 420 Delaware Street S.E, Minneapolis, MN 55455 ABSTRACT The mammalian im- In recent years, it has become clear that TCR is specific for a self peptide-class I mune system must specifically recognize a full understanding of immune tolerance MHC complex) T cell that will exit the and eliminate foreign invaders but refrain cannot be achieved with reductionist in thymus and seed the secondary lymphoid from damaging the host. This task is vitro approaches that separate the individ- tissues (3, 4). In contrast, cortical CD4+ accomplished in part by the production of ual lymphocyte from its in vivo environ- CD8+ thymocytes that express TCRs that a large number of T lymphocytes, each ment. The in vivo immune response is a have no avidity for self peptide-MHC bearing a different antigen receptor to well-organized process that involves mul- complexes do not survive and die by an match the enormous variety of antigens tiple interactions of lymphocytes with each apoptotic mechanism. Cortical epithelial present in the microbial world. However, other, with bone-marrow-derived antigen- cells are essential for the process of pos- because antigen receptor diversity is gen- presenting cells (APCs), as well as with itive selection because they display the self erated by a random mechanism, the im- nonlymphoid cells and their products. The peptide-MHC complexes that are recog- mune system must tolerate the function of anatomic features that are designed to op- nized by CD4+ CD8+ thymocytes and also T lymphocytes that by chance express a timize immune tolerance toward innocuous provide essential differentiation factors self-reactive antigen receptor. -

That Induce Chronic Inflammation Selection Leading to Autoreactive T
Thymic Involution Perturbs Negative Selection Leading to Autoreactive T Cells That Induce Chronic Inflammation This information is current as Brandon D. Coder, Hongjun Wang, Linhui Ruan and of October 3, 2021. Dong-Ming Su J Immunol 2015; 194:5825-5837; Prepublished online 8 May 2015; doi: 10.4049/jimmunol.1500082 http://www.jimmunol.org/content/194/12/5825 Downloaded from Supplementary http://www.jimmunol.org/content/suppl/2015/05/08/jimmunol.150008 Material 2.DCSupplemental http://www.jimmunol.org/ References This article cites 69 articles, 22 of which you can access for free at: http://www.jimmunol.org/content/194/12/5825.full#ref-list-1 Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists by guest on October 3, 2021 • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2015 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Thymic Involution Perturbs Negative Selection Leading to Autoreactive T Cells That Induce Chronic Inflammation Brandon D. Coder, Hongjun Wang,1 Linhui Ruan,2 and Dong-Ming Su Thymic involution and the subsequent amplified release of autoreactive T cells increase the susceptibility toward developing autoimmunity, but whether they induce chronic inflammation with advanced age remains unclear. -

The Balance Players of the Adaptive Immune System Mads Hald Andersen1,2
Published OnlineFirst February 13, 2018; DOI: 10.1158/0008-5472.CAN-17-3607 Cancer Perspective Research The Balance Players of the Adaptive Immune System Mads Hald Andersen1,2 Abstract Equilibrium between immune activation and suppression may Vaccination against genetically stable cells with regular HLA be necessary to maintain immune homeostasis, because proin- expression is an attractive way to directly target immunosuppres- flammatory effector T cells (defined as antiregulatory T cells) sive cells in addition to attracting proinflammatory cells into the counteract the functions of regulatory immune cells. These self- tumor microenvironment. Importantly, vaccination toward IDO reactive T cells recognize human leukocyte antigen (HLA)–restrict- or PD-L1 to potentiate such T cells have proven safe, with minimal ed epitopes derived from proteins expressed by regulatory immune toxicity in the clinical phase I trials conducted thus far. cells such as IDO, PD-L1, PD-L2, or arginase. The activation of Significance: Autoreactive effector T cells that specifically rec- such proinflammatory effector T cells offers a novel way to directly ognize regulatory cells might be useful to harness for cancer target the tumor microenvironment, potentially giving them immunotherapy to target the immune-suppressive tumor micro- considerable clinical value, especially in patients with cancer. environment. Cancer Res; 1–4. Ó2018 AACR. It was the recognition of suppressor T cells, now called regu- HLA-restricted derived epitopes, which are generated from intra- latory T cells (Treg), pioneered by Dr. Sakaguchi that highlighted cellular degraded antigens, are able to directly eliminate regula- the importance of regulatory cells in the maintenance of immu- tory immune cells (Fig. -

Cyclophosphamide-Induced Tolerance Induction And
Regulatory Roles of NKT Cells in the Induction and Maintenance of Cyclophosphamide-Induced Tolerance This information is current as Toshiro Iwai, Yukihiro Tomita, Shinji Okano, Ichiro of September 25, 2021. Shimizu, Yohichi Yasunami, Takashi Kajiwara, Yasunobu Yoshikai, Masaru Taniguchi, Kikuo Nomoto and Hisataka Yasui J Immunol 2006; 177:8400-8409; ; doi: 10.4049/jimmunol.177.12.8400 Downloaded from http://www.jimmunol.org/content/177/12/8400 References This article cites 32 articles, 21 of which you can access for free at: http://www.jimmunol.org/content/177/12/8400.full#ref-list-1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists by guest on September 25, 2021 • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2006 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Regulatory Roles of NKT Cells in the Induction and Maintenance of Cyclophosphamide-Induced Tolerance1 Toshiro Iwai,* Yukihiro Tomita,2* Shinji Okano,† Ichiro Shimizu,* Yohichi Yasunami,‡ Takashi Kajiwara,* Yasunobu Yoshikai,§ Masaru Taniguchi,ʈ Kikuo Nomoto,¶ and Hisataka Yasui* We have previously reported the sequential mechanisms of cyclophosphamide (CP)-induced tolerance.