R Harries Engd Thesis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Unmanned Air Vehicle Features, Applications and Technologies Version 25
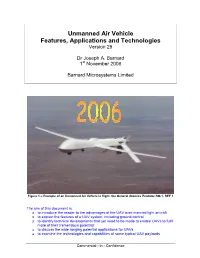
Unmanned Air Vehicle Features, Applications and Technologies Version 25 Dr Joseph A. Barnard 1st November 2006 Barnard Microsystems Limited Figure 1 = Example of an Unmanned Air Vehicle in flight: the General Atomics Predator RQ-1. REF 1 The aim of this document is: to introduce the reader to the advantages of the UAV over manned light aircraft to explain the features of a UAV system, including ground control to identify technical developments that yet need to be made to enable UAVs to fulfil more of their tremendous potential to discuss the wide ranging potential applications for UAVs to examine the technologies and capabilities of some typical UAV payloads Commercial - in - Confidence Executive Summary The Unmanned Air Vehicle (UAV) is a robot plane containing a flight control computer, precision navigation (GPS and an Inertial Measurement Unit) and flight control electronics, a low vibration engine (such as a Wankel engine), and a payload such as a high resolution camera. The UAV represents a new, cost effective and more environmentally responsible approach to aerial reconnaissance and geophysical survey work. This document discusses the wide-ranging applications of the UAV, typical attributes of which are: Typical Unmanned Air Vehicle versus a Cessna Skylane Payload 1 … 100 Kg 91 Kg Speed min … max 30 … 150 Kph 91 … 276 Kph Altitude min … max 20 m … 25 Km 100 m … 5.5 Km Max flight duration 5 … 40 hours 11.8 hours Max flight range 150 … 3,000 Km 1,793 Km Purchase price typically $ 35,000 for 10 Kg PL $ 268,750 Operating cost typically $ 26 / hr for 10 Kg PL $ 300 / hr Crash damage 74 Kg Æ 105 KJ KE for 10 Kg PL 1,243 Kg Æ 5,145 KJoule KE Advantages of the UAV over a manned aircraft The UAV can fly day-after-day, night-after-night, in dangerous weather conditions for up to 30 hours at a time on an accurate flight path under computer control. -

The Aerospace Industry and Air Transport in Wales
The Aerospace Industry and Air Transport in Wales Abstract This paper provides background briefing on the aerospace industry and air transport in Wales. It considers the aerospace market, including the maintenance, repair and overhaul (MRO) sector, the key players in the aerospace industry in Wales, and skills and training issues faced by the aerospace sector. It also looks at air transport, airports and policies relating to the development of air transport in Wales. May 2005 Members’ Research Service / Gwasanaeth Ymchwil yr Aelodau Members’ Research Service: Research Paper Gwasanaeth Ymchwil yr Aelodau: Papur Ymchwil The Aerospace Industry and Air Transport in Wales Neil Cox May 2005 Paper number: 05/0641/NC © Crown copyright 2005 Enquiry no: 05/0641/NC Date: 19 May 200 This document has been prepared by the Members’ Research Service to provide Assembly Members and their staff with information and for no other purpose. Every effort has been made to ensure that the information is accurate, however, we cannot be held responsible for any inaccuracies found later in the original source material, provided that the original source is not the Members’ Research Service itself. This document does not constitute an expression of opinion by the National Assembly, the Welsh Assembly Government or any other of the Assembly’s constituent parts or connected bodies. Members’ Research Service: Research Paper Gwasanaeth Ymchwil yr Aelodau: Papur Ymchwil Members’ Research Service: Research Paper Gwasanaeth Ymchwil yr Aelodau: Papur Ymchwil Contents 1. Introduction .......................................................................................................... 1 2. Aerospace Market................................................................................................. 2 3. Maintenance, Repair and Overhaul (MRO) Market............................................. 3 4. Aerospace Industry in Wales............................................................................... 4 5. -
Marketing Guide and Directory 2014 Edition
Unmanned Vehicle Systems (UVS) COMPONENTS Aircraft - Ground - Sea - Space Systems, Subsystems, Components, Materials and Other Infrastructure Equipment and Services Marketing Guide and Directory 2014 Edition Preface This Marketing Guide on "Components for Unmanned Vehicles" is a companion volume to a recently published "UAV Marketing Directory" which was devoted to aerial systems. In addition, this report includes not only aerial but also ground, maritime, submarine, and satellite unmanned systems. Over 1,000 companies, organizations such as educational, research, development and testing and economic development organizations are included covering 100 different categories. An index is provided which places companies in various categories. The majority of companies included are component, materials, and subsystems equipment suppliers but also includes companies providing services, consulting, training, publishing, and other infrastructure suppliers. It is essentially a complete source of information on unmanned systems. Since there is no market study on all the unmanned systems types, a Foreword is included in the report which is taken from the latest version of the DOD Roadmap on Unmanned Systems. This is the only estimate of the unmanned systems market available today. Even though the sequestration and recent budget cuts are now being implemented, the Roadmap does provide a good indication of market trends at least for the government markets. The data collected and included in this report has been obtained by Information Gatekeepers, Inc. (IGI) from the best sources available including tradeshows, conferences, publications, advertisements, press releases, and internet sources. The index of products has been prepared based on company descriptions provided. Placement of companies in the various categories has been assigned by IGI. -
Representative UK Robotics and Autonomous Systems (RAS) Infrastructure
Science Landscape Seminar Series: Representative UK Robotics and Autonomous Systems (RAS) Infrastructure Notes to reader This document is to inform discussion only and is subject to the following caveats: • Inclusion, non-inclusion or otherwise is not intended to reflect on the standing of any organisation or infrastructure. • We did not include classified defence and intelligence assets. • Assignment of Research Areas, Eight Great Technologies and Industrial Strategy sectors was based on desk research and may be subject to error. Categories are designed to inform the general discussion and not reflect on individual organisations or infrastructure. Absence of icons in category tables indicates that (in the project team’s opinion) a piece of infrastructure cannot be easily categorised. • If any mistakes have been made, please inform the seminar secretariat on [email protected]. 1 Logo key Location Research Area Eight Great Industrial Strategy Technologies UK Arts and Energy Life Science humanities Storage EU Biological and Big Data Aerospace medical sciences Global Earth sciences Satellites Professional Business Services Engineering Robotics and Education Autonomous Funding Systems Research Physical, Synthetic Nuclear Councils mathematical Biology and computer sciences Departmental Social and Regenerative Oil and Gas economic Medicine sciences Private Sector Agri-Science Automotive Charity Advanced Offshore Materials Wind Academic Quantum Information Technologies Economy European Construction Agri-tech 2 List of infrastructure -

Projekt UAST – 42 TESTGEBIETE INTERNATIONAL
Projekt UAST – 42 TESTGEBIETE INTERNATIONAL Testgebiet - ID 01 02 03 Testgebiet - LAND (IOC) BEL (Belgien) DEN (Dänemark) ESP (Spanien) Testgebiet - REGION Sint Truiden, Limburg Odense (Peninsula Funen west of Kopenhagen) Katalonien (Barcelona) Name (full) Droneport NV UAS Test Center Denmark BCN Drone Test Center Name (short) Droneport WEB (formal & background) www.droneport.eu/en/testsite www.uastestcenter.com/airspace/approved-airspace/technical-specifications www.barcelonadronecenter.com https://de.wikipedia.org/wiki/Flughafen_Odense http://www.catuav.com https://en.wikipedia.org/wiki/Sint-Truiden_Air_Base Gründung 2013 2015 2012 DronePort CATUAV UAS Test Center Denmark (Stadt / Flughafen Sint Truiden) (private company by Jordi Santacana, earth observation with UAS) Staatliche / Regionale Beteiligung X (LRA - Limburg Regional Airport) X (Hans Christian Anderson Airport, City of Odense) Universität X (University of Southern Denmark) Forschungseinrichtung/organisation Produzenten X (CAT UAV) Verbände / Cluster / NPO X (SDU UAS Center, UAS Test Center Denmark) Reiner Betreiber Testgebiet X Sonstiges (Ehem.) Militäreinrichtung (grün) / oder (ehemaliger) ziviler Flughafen (blau) Ehem. Military airfield of St. Truiden (bis 1996) Hans Christian Andersen Airport (EKOD) oder Mischform/Kooperation (Grün-Blau) Luftraum - LATERAL: Maximale Ausdehnung (in km²) 84 km2 (größtes Gebiet) 867 km2 (3 Gebiete) 25 km2 Luftraum - Stückelung in mehrere Gebiete? 5 Gebiete (manche im Aufbau) 3 Gebiete (alle drei auch BVLOS) 1 Gebiet Luftraum - VERTIKAL: Max. -

Back from the Battlefield: Domestic Drones in the UK
BACK FROM THE BATTLEFIELD DOMESTIC DRONES IN THE UK May 2014 Statewatch This report is published by Statewatch Statewatch is a non-profit-making voluntary group founded and Drone Wars UK under in 1991. It is comprised of lawyers, academics, journalists, ISBN 978 1 8744 8126 0. researchers and community activists with a network of contributors drawn from 17 countries. Statewatch encourages Personal usage as private the publication of investigative journalism and critical individuals/“fair dealing” is allowed. research in Europe in the fields of the state, justice and home affairs, civil liberties, accountability and openness. Usage by those working for organisations is allowed provided the More information: organisation holds an appropriate www.statewatch.org | [email protected] licence from the relevant reprographic 0207 697 4266 rights organisation (eg. Copyright PO Box 1516, London, N16 0EW Licensing Agency in the UK), with such usage being subject to the terms and conditions of that licence and to local Drone Wars UK copyright law. Drone Wars UK is a small British NGO, founded in the Neither Statewatch nor Drones Wars spring of 2010, to undertake research, education and UK hold a corporate view; the opinions campaigning on the use of Unmanned Aerial Vehicles and expressed are solely those of the author. the wider issue of remote warfare. Drone Wars UK has become recognised internationally as a credible and reliable Author source of information on the use of drones and unmanned Chris Jones technology. The research and information produced by Drone [email protected] Wars UK is used by journalists, NGOs, lawyers, human rights organisations, campaigners and the general public. -
Armed Drones and the 'Playstation' Mentality
Convenient Killing • Armed Drones and the ‘Playstation’ Mentality 1 Convenient Killing Armed Drones and the ‘Playstation’ Mentality 2 “Equally discomfiting is the “PlayStation mentality” that surrounds drone killings. Young military personnel raised on a diet of video games now kill real people remotely using joysticks. Far removed from the human consequences of their actions, how will this generation of fighters value the right to life? How will commanders and policymakers keep themselves immune from the deceptively antiseptic nature of drone killings? Will killing be a more attractive option than capture? Will the standards for intelligence-gathering to justify a killing slip? Will the number of acceptable ‘collateral’ civilian deaths increase?” Philip Alston and Hina Shamsi, ‘A Killer above the law’, The Guardian, 02.08.10 Convenient Killing • Armed Drones and the ‘Playstation’ Mentality 3 Contents Executive Summary ..................................................................................... 4 Introduction ...................................................................................................... 5 Background ...................................................................................................... 6 The Human Cost ............................................................................................. 8 Production and Proliferation ................................................................... 11 The UK and Drones ................................................................................... -
Complete Guide Drones By
Complete Guide by Drones The air, sea, land defence decision-maker’s technology reference monitor. Established 1976 monitor. technology reference sea, land defence decision-maker’s The air, INTERNATIONAL: Supplement to issue 3/2008 Premonition or Logical Assumption? .V. Roe (Avro), Breguet, Curtiss, given in the earlier editions of Armada’s supple- Caproni, Convair, Dewoitine, Douglas, ments on drones, and we would not fall too short A Grumman, McDonnell, Fairchild, of the number of military aircraft manufacturers Fairey, Focke-Wulf, Handley-Page, Heinkel, of yesteryear. Laughead (Lockheed brothers’ original name), Ford, Hurel-Dubois, Messerschmitt, Maurane, The development of military aviation only North American, Nieuport, Latécoère, Polikar- started to soar during the Great War and went on pov, Republic, Rockwell, Sopwith, Saunders- to grow to the above-mentioned telephone Roe, Spad, De Havilland, Supermarine, Vought – directory situation until the Second World War. these illustrious names now belong to a long Then consolidations (as euphemistically put) gone past. The list is much longer and could fill a started to take place. Extraordinarily, the devel- phone directory, maybe two. opment of drones followed the same application pattern as that of piloted aircraft at the begin- Today, how many names are left in the defence ning of the last century. The first aircraft were aviation world? Fingers of only two hands suffice used as observation “apparatuses” (aircraft were to reckon them: Boeing, Dassault, Saab, Lock- initially referred to as “apparatus” in early main- heed Martin, Embraer, MiG, Eads, Sukhoi, BAE tenance manuals), particularly to spot enemy Systems, a few trainer aircraft manufacturers artillery movements. -
Unmanned Aircraft Systems Uavs Design, Development and Deployment
P1: OTE/OTE/SPH P2: OTE FM JWBK459-Austin March 19, 2010 12:44 Printer Name: Yet to Come UNMANNED AIRCRAFT SYSTEMS UAVS DESIGN, DEVELOPMENT AND DEPLOYMENT Reg Austin Aeronautical Consultant A John Wiley and Sons, Ltd., Publication P1: OTE/OTE/SPH P2: OTE FM JWBK459-Austin March 19, 2010 12:44 Printer Name: Yet to Come P1: OTE/OTE/SPH P2: OTE FM JWBK459-Austin March 19, 2010 12:44 Printer Name: Yet to Come UNMANNED AIRCRAFT SYSTEMS P1: OTE/OTE/SPH P2: OTE FM JWBK459-Austin March 19, 2010 12:44 Printer Name: Yet to Come Aerospace Series List Path Planning Strategies for Cooperative Tsourdos et al August 2010 Autonomous Air Vehicles Introduction to Antenna Placement & Installation Macnamara April 2010 Principles of Flight Simulation Allerton October 2009 Aircraft Fuel Systems Langton et al May 2009 The Global Airline Industry Belobaba April 2009 Computational Modelling and Simulation of Diston April 2009 Aircraft and the Environment: Volume 1 - Platform Kinematics and Synthetic Environment Handbook of Space Technology Ley, Wittmann, Hallmann April 2009 Aircraft Performance Theory and Practice for Pilots Swatton August 2008 Surrogate Modelling in Engineering Design: Forrester, Sobester, Keane August 2008 A Practical Guide Aircraft Systems, 3rd Edition Moir & Seabridge March 2008 Introduction to Aircraft Aeroelasticity And Loads Wright & Cooper December 2007 Stability and Control of Aircraft Systems Langton September 2006 Military Avionics Systems Moir & Seabridge February 2006 Design and Development of Aircraft Systems Moir & Seabridge June -

Police Aviation News July 2006
Police Aviation News July 2006 ©Police Aviation Research Number 123 July 2006 IPAR Police Aviation News July 2006 2 PAN – POLICE AVIATION NEWS is published monthly by INTERNATIONAL POLICE AVIATION RESEARCH 7 Windmill Close, Honey Lane, Waltham Abbey, Essex EN9 3BQ UK +44 1992 714162 Editor Bryn Elliott Bob Crowe www.bobcroweaircraft.com Digital Downlink www.bms-inc.com FLIR Systems www.flir.com L3 Wescam www.wescam.com Power in a box www.powervamp.com Turning the blades www.turbomeca.com Airborne Law Enforcement Association www.alea.org European Law Enforcement Association www.pacenet.info Sindacato Personale Aeronavigante Della Polizia www.uppolizia.it Bundesvereinigung fliegendes Personal der Polizei (BfPP) www.bfpp.de LAW ENFORCEMENT ARGENTINA MENDOZA: Two new helicopters for the police were to have been delivered to the Provin- cial Police last month. Both helicopters of an as yet unidentified type were acquired some time ago but have been delayed in Brazil by customs. [Journada] FRANCE SECURITE CIVILE: In the wake of a fatal accident in the Pyrenees of a Securite Civile Eurocopter EC145 early last month [see under accidents] there were reports in the French media that there was significant disquiet among Securite Civile staff about the safety of the aircraft type in the mountain rescue environment. The same article suggested that were also perceived problems with the recent acquisition of fixed wing Bombardier Q400 in a fire fighting role. Pilots were stating that the aircraft was unproven in the role and therefore likely to be returned to the manufacturer if found to be wanting. Although the allegations were not stating that either of the aircraft was dangerous it was be- ing suggested that there were questionable aspects relating to both, especially after two allegedly similar accidents to the EC145. -
Tout En Pagemaker
Issue 2008/08 April 20, 2008 This publication is produced by Blyenburgh & Co for UVS International and is supplied free-of-charge. It has as purpose to help raise the level of global awareness relative to ongoing research & development, relevant technologies, production and sales, as well as current & future applicatons of unmanned vehicle systems (air, ground & naval). It has a controlled circulation of 6234 nominal addressees, consisting of UVS International members (2011), government (343), military (1142) & diplomatic corp (16) representatives, regulatory authorities (309), stakeholder associations (77) & researchers & academics (2061) in 68 countries involved with unmanned vehicles systems. As many of the defence industry and governmental recipients cannot access web sites from their office computers, this News Flash contains the entire text of the articles & press releases. All recipients of the UVS News Flash are encouraged to supply UVS International with their press releases & announcements and to forward the UVS News Flash to their contacts & relations. Recipients of this publication no longer desiring to receive it are requested to inform UVS International by email indicating «De-subscribe from News Flash» in the object box & indicating their complete name + affiliation + email address in the email text. MARK YOUR AGENDA UAS ATM INTEGRATION UAS LAUNCH & RECOVERY EUROCONTROL Workshop ASNE Technical Conference & Exhibition Brussels, Belgium Annapolis, Maryland, USA May 7 & 8, 2008 May 19 & 20, 2008 www.eurocontrol.int/UAS_workshop -
Comparison of Selected UAS Test Areas in Europe and America Regarding Practical Aspects for Developers
Master thesis Comparison of Selected UAS Test Areas in Europe and America regarding Practical Aspects for Developers Submitted by: Alexander LAPPI, BSc Registration Number: 1210587028 Academic Supervisor: Ing. Andreas HINZE Company Supervisor: Raoul FORTNER, MSc (AAI) Date of submission: 13 September 2017 i Affidavit I hereby affirm in lieu of an oath that the present Master’s thesis entitled “Comparison of selected UAS test areas in Europe and America regarding practical aspects for developers” has been written by myself without the use of any resources other than those indicated, quoted and referenced. Graz, 13 September 2017 Alexander Lappi, BSc ii Preface The six months which I spent at the Austrian Aeronautics Industries Group (AAI) from March to August 2017 did not only result in this thesis, but also in an uncountable amount of experiences and memories, which I would hardly have made elsewhere. My employment at this company offered me to get the chance to have a unique, close and practical view on the Austrian Aeronautics Industries, especially within the interviews as a part of the study UAST, which were conducted with numerous companies from different niches and gave me as a student an outstanding possibility for planning my future career. I would like to thank Secretary General KR Ing. Franz Hrachowitz for giving me the opportunity to work for the AAI, Mrs. Schmöllerl for her sunny personality which eased numerous intensive office days, and especially Raoul Fortner, MSc, who hired me to work for the AAI and was furthermore constantly zealous to maximize the value I could gain from this employment – Not only by fully incorporating me into the project UAST and taking me to numerous events and memorable business trips, but also by unhesitatingly and intensively supporting me during the creation of this thesis as my company supervisor Thanks to Ing.