485560Wp0hiv1r10box338914b
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

CONTENTS Contents
CONTENTS Contents Symbols 5 Introduction 6 Players (White first) and event Opening Page 1 Gelfand – Dreev, Tilburg 1993 Semi-Slav Defence [D48] 8 2 Benjamin – Anand, Groningen PCA 1993 Sicilian Defence [B63] 13 3 Karpov – Morovi‡, Las Palmas (1) 1994 Queen’s Gambit Declined [D32] 20 4 Adams – Agdestein, Oslo (2) 1994 Alekhine Defence [B02] 25 5 Yusupov – Dokhoian, Bundesliga 1993/4 Queen’s Gambit Declined [D31] 31 6 Gelfand – Hertneck, Munich 1994 Benko Gambit [A57] 37 7 Kasparov – P. Nikoli‡, Horgen 1994 French Defence [C18] 43 8 Karpov – Salov, Buenos Aires 1994 Sicilian Defence [B66] 50 9 Timman – Topalov, Moscow OL 1994 King’s Indian Defence [E87] 56 10 Shirov – Piket, Aruba (4) 1995 Semi-Slav Defence [D44] 60 11 Kasparov – Anand, Riga 1995 Evans Gambit [C51] 66 12 J. Polgar – Korchnoi, Madrid 1995 Caro-Kann Defence [B19] 71 13 Kramnik – Piket, Dortmund 1995 Catalan Opening [E05] 76 14 Kramnik – Vaganian, Horgen 1995 Queen’s Indian Defence [E12] 82 15 Shirov – Leko, Belgrade 1995 Ruy Lopez (Spanish) [C92] 88 16 Ivanchuk – Topalov, Wijk aan Zee 1996 English Opening [A26] 93 17 Khalifman – Short, Pärnu 1996 Queen’s Indian Defence [E12] 98 18 Kasparov – Anand, Amsterdam 1996 Caro-Kann Defence [B14] 104 19 Kasparov – Kramnik, Dos Hermanas 1996 Semi-Slav Defence [D48] 111 20 Timman – Van der Wiel, Dutch Ch 1996 Sicilian Defence [B31] 117 21 Svidler – Glek, Haifa 1996 French Defence [C07] 123 22 Torre – Ivanchuk, Erevan OL 1996 Sicilian Defence [B22] 128 23 Tiviakov – Vasiukov, Russian Ch 1996 Ruy Lopez (Spanish) [C65] 134 24 Illescas – -

Preface We Are Pleased to Present This Collection of Scholarly Articles of the International Scientific-Practical Conference «T
SHS Web of Conferences 8 9 , 00001 (2020) https://doi.org/10.1051/shsconf/20208900001 Conf-Corp 2020 Preface We are pleased to present this collection of scholarly articles of the International Scientific-Practical Conference «Transformation of Corporate Governance Models under the New Economic Reality» (CC-2020). The conference was held in Ural State University of Economics, Yekaterinburg, Russia, on November 20, 2020. The key topics of the Conference were: o A shift in the corporate governance paradigm in the context of the technological transformation and the coronavirus crisis; o Boards of Directors as drivers of business transformation in the new post-pandemic reality; o Modernization of the stakeholder approach in the development of corporate governance models, understanding of the interests of stakeholders and evaluation of their contribution to the formation of the value and social capital of the business; o The impact of new technologies (big data, artificial intelligence, neural networks) on the development and efficiency of corporate governance systems; o Coordination of the corporate governance system with new business formats: ecosystem, platform, distributed companies; o The impact of digitalization on the formation of strategic corporate interests of a company; o CSR and corporate strategies: problems of transformation to achieve sustainable development. The conference was attended in an online format by almost 70 participants from leading universities in 10 countries: Russia, Italy, Hungary, Poland, Bulgaria, Belarus, Uzbekistan, Moldova, Kazakhstan, DPR. The geography of Russian participants is also extensive - Moscow, St. Petersburg, Novosibirsk, Kazan, Saratov, Khanty-Mansiysk, Elista, Omsk, Kemerovo, Ryazan, Nizhny Novgorod, Grozny and other cities. The conference was held with the informational support of the Russian Institute of Directors, NP "Elite Club of Corporate Conduct". -

Tibetan Studies in Russia: a Brief Historical Account
Annuaire de l'École pratique des hautes études (EPHE), Section des sciences religieuses Résumé des conférences et travaux 126 | 2019 2017-2018 Religions tibétaines Tibetan studies in Russia: a brief historical account Alexander Zorin Electronic version URL: https://journals.openedition.org/asr/2498 DOI: 10.4000/asr.2498 ISSN: 1969-6329 Publisher Publications de l’École Pratique des Hautes Études Printed version Date of publication: 15 September 2019 Number of pages: 63-70 ISBN: 978-2909036-47-2 ISSN: 0183-7478 Electronic reference Alexander Zorin, “Tibetan studies in Russia: a brief historical account”, Annuaire de l'École pratique des hautes études (EPHE), Section des sciences religieuses [Online], 126 | 2019, Online since 19 September 2019, connection on 06 July 2021. URL: http://journals.openedition.org/asr/2498 ; DOI: https:// doi.org/10.4000/asr.2498 Tous droits réservés : EPHE Religions tibétaines Alexander ZORIN Directeur d’études invité Institut des Manuscrits Orientaux, Académie des Sciences de la Russie, Saint-Pétersbourg Tibetan studies in Russia: a brief historical account IBETOLOGY is one of the oldest branches of Oriental studies in Russia that used to Tbe closely connected with foreign and inner policy of the Russian State starting from the late 17th century. The neighborhood with various Mongolian politia and gradual spread of Russian sovereignty upon some of them caused the necessity of studying and using Tibetan along with Mongolian, Oirat, Buryat languages and also, from the 18th century, studying Tibetan Buddhism as the dominant religion of these people. Huge collections of Tibetan texts and Tibetan arts were gradually gathered in St. Petersburg and some other cities, and the initiator of this process was Peter the Great, the first Russian emperor. -
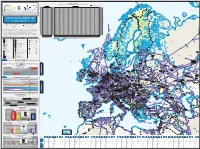
System Development Map 2019 / 2020 Presents Existing Infrastructure & Capacity from the Perspective of the Year 2020
7125/1-1 7124/3-1 SNØHVIT ASKELADD ALBATROSS 7122/6-1 7125/4-1 ALBATROSS S ASKELADD W GOLIAT 7128/4-1 Novaya Import & Transmission Capacity Zemlya 17 December 2020 (GWh/d) ALKE JAN MAYEN (Values submitted by TSO from Transparency Platform-the lowest value between the values submitted by cross border TSOs) Key DEg market area GASPOOL Den market area Net Connect Germany Barents Sea Import Capacities Cross-Border Capacities Hammerfest AZ DZ LNG LY NO RU TR AT BE BG CH CZ DEg DEn DK EE ES FI FR GR HR HU IE IT LT LU LV MD MK NL PL PT RO RS RU SE SI SK SM TR UA UK AT 0 AT 350 194 1.570 2.114 AT KILDIN N BE 477 488 965 BE 131 189 270 1.437 652 2.679 BE BG 577 577 BG 65 806 21 892 BG CH 0 CH 349 258 444 1.051 CH Pechora Sea CZ 0 CZ 2.306 400 2.706 CZ MURMAN DEg 511 2.973 3.484 DEg 129 335 34 330 932 1.760 DEg DEn 729 729 DEn 390 268 164 896 593 4 1.116 3.431 DEn MURMANSK DK 0 DK 101 23 124 DK GULYAYEV N PESCHANO-OZER EE 27 27 EE 10 168 10 EE PIRAZLOM Kolguyev POMOR ES 732 1.911 2.642 ES 165 80 245 ES Island Murmansk FI 220 220 FI 40 - FI FR 809 590 1.399 FR 850 100 609 224 1.783 FR GR 350 205 49 604 GR 118 118 GR BELUZEY HR 77 77 HR 77 54 131 HR Pomoriy SYSTEM DEVELOPMENT MAP HU 517 517 HU 153 49 50 129 517 381 HU Strait IE 0 IE 385 385 IE Kanin Peninsula IT 1.138 601 420 2.159 IT 1.150 640 291 22 2.103 IT TO TO LT 122 325 447 LT 65 65 LT 2019 / 2020 LU 0 LU 49 24 73 LU Kola Peninsula LV 63 63 LV 68 68 LV MD 0 MD 16 16 MD AASTA HANSTEEN Kandalaksha Avenue de Cortenbergh 100 Avenue de Cortenbergh 100 MK 0 MK 20 20 MK 1000 Brussels - BELGIUM 1000 Brussels - BELGIUM NL 418 963 1.381 NL 393 348 245 168 1.154 NL T +32 2 894 51 00 T +32 2 209 05 00 PL 158 1.336 1.494 PL 28 234 262 PL Twitter @ENTSOG Twitter @GIEBrussels PT 200 200 PT 144 144 PT [email protected] [email protected] RO 1.114 RO 148 77 RO www.entsog.eu www.gie.eu 1.114 225 RS 0 RS 174 142 316 RS The System Development Map 2019 / 2020 presents existing infrastructure & capacity from the perspective of the year 2020. -

R U S S I a North Caucasus: Travel Advice
YeyskFOREIGN AND COMMONWEALTH OFFICE BRIEFING NOTES ROSTOVSKAYA OBLAST’ Krasnyy Yar Ozero Astrakhan’ North Caucasus:Sal’sk Munych-Gudilo Travel Advice Elista ASTRAKHANSKAYA Primorsko-Akhtarsk Yashkul’ OBLAST’ Sea of RESPUBLIKA KALMYKIYA- Krasnogvardeyskoye KHAL’MG TANGCH Tikhoretsk Divnoye Azov KRASNODARSKIY KRAY Chograyskoye Vodokhranilishche Slavyansk-na-Kubani Kropotkin Lagan’ RUSSIASvetlograd Krasnodar Anapa Krymsk Blagodarnyy Tshchikskoye Armavir Stavropol’ Vodokhranihshche Kuma RESPUBLIKA Kuban’ STAVROPOL’SKIY KRAY ADYGEYA Novorossiysk Belorechensk Budennovsk Labinsk Nevinnomyssk Kizlyarskiy Maykop Zaliv Ostrov Tyuleniy Kochubey Cherkessk CASPIAN Tuapse Georgiyevsk Pyatigorsk Ostrov Chechen’ Kislovodsk Kizlyar Karachayevsk CHECHENSKAYA SEA KARACHAYEVO- Prokhladnyy Mozdok RESPUBLIKA (CHECHNYA) Sochi C CHERKESSKAYA RESPUBLIKA Nal’chik A Mount RESPUBLIKA Gudermes BLACK KABARDINO- INGUSHETIYA Groznyy El’brus Khasavyurt BALKARSKAYA Nazran Argun U RESPUBLIKA ABKHAZIA Ardon Magas SEA RESPUBLIKA Urus-Martan Makhachkala SEVERNAYA Vladikavkaz Kaspiysk COSETIYA-ALANIYA (NORTH OSSETIA) Buynaksk RESPUBLIKA A DAGESTAN International Boundary Khebda Autonomous Republic Boundary S Russian Federal Subject Boundary GEORGIA Derbent National Capital U Administrative Centre Other Town Advise against all travel Major Road AJARIA TBILISI S Rail Advise against all but essential travel 0 50miles See our travel advice before travelling 0 100kilometres TURKEY AZERBAIJAN FCO 279 Edition 1 (September 2011) Users should note that this map has been designed for briefing purposes only and it should not be used for determining the precise location of places or features. This map should not be considered an authority on the delimination of international boundaries or on the spelling of place and feature names. Maps produced for I&TD Information Management Depertment are not to be taken as necessarily representing the views of the UK government on boundaries or political status © Crown Copyright 2011. -

Association for Russian Centers for the Religious Studies the 5Th Congress of Russian Scholars of Religion November 26–28
Религиоведение. 2020. № 1 Religiovedenie [Study of Religion]. 2020. No. 1 DOI: 10.22250/2072-8662.2020.1.152-154 Association for Russian Centers for the Religious Studies The 5th Congress of Russian Scholars of Religion November 26–28, 2020 Saint Petersburg The State Museum of the History of Religion “RELIGION AND ATHEISM IN 21st CENTURY” Association for Russian Centers for the Religious Studies announces The 5th Congress of Russian Scholars of Religion. The 5th Congress continues the series of scholarly events being started at the 1st Congress (St-Petersburg, 2012) and afterwards kept up at the 2nd (St. Petersburg, 2014), the 3d (Vladimir, 2016) and the 4th (Blagoveshchensk, 2018) Congresses. The Congresses provides an interdisciplinary platform to discuss a great variety of problems, trends and phenomena in the field of contemporary Religious Studies, being the complex research area, methodologically based on humanities, social sciences and also, particularly during the last decades, on natural science. Previous Congresses took in participants from many cities of Russia, including Moscow, St. Petersburg, Arkhangelsk, Barnaul, Blagoveshchensk, Chita , Elista, Kazan, Khabarovsk, Krasnoyarsk, Murmansk, Nizhny Novgorod, Novgorod Veliky, Novosibirsk, Omsk, Oryol, Perm, Ryazan, Saratov, Sevastopol, Tambov, Tomsk, Tyumen, Ufa, Vladimir, Vladivostok, Volgograd, Voronezh, Yakutsk, Yaroslavl, Yekaterinburg. The scholars from Armenia, Azerbaijan, Belarus, China, Denmark, Germany, Kazakhstan, Kyrgyzstan, Latvia, Lithuania, Poland, Slovakia, Sweden, Ukraine and United Kingdom have traditionally contributed to the Congresses work. The Organizing Committee of the 5th Congress of Russian Scholars of Religion is happy to welcome all the scholars interested in Religious Studies from Russian Federation and other countries. Young scholars, postgraduate and graduate students are especially encouraged to contribute to the 5th Congress work. -

REFERENCES 1. Ochir-Goryaeva M.A. 2008. Arkheologicheskie
REFERENCES 1. Ochir-Goryaeva M.A. 2008. Arkheologicheskie pamyatniki volgo-manychskikh stepey (svod pamyatnikov, issledovannykh na territorii Respubliki Kalmykiya v 1929–1997 gg.). [Archaeological monuments of the Volga-Manych steppes (the list of architectural monuments, explored on the territory of the Republic of Kalmykia in 1929–1997)]. Elista, Gerel Publishers: 298 p. (In Russian). 2. Zlatkin I.Ya. 1964. Istoriya Dzhungarskogo khanstva (1635–1758). [The history of the Dhungar khanate (1635–1758)]. Moscow, Nauka Publ.: 482 p. (In Russian). 3. Moiseev V.A. 1998. Rossiya i Dzhungarskoe khanstvo v XVIII veke (ocherk vneshnepoliticheskikh otnosheniy). [Russia and the Dzungar khanate in the 18th century (essay of foreign policy relations)]. Barnaul, Altai state University Publ.: 174 p. (In Russian). 4. Gurevich B.P. 1985. [The nature of the political status of the Dzungar khanate and its interpretation in the historiography of China]. In: IV Mezhdunarodnyy kongress mongolovedov. T. 1. [Proceedings of the IVth International Congress of Mongolists. Vol. I]. Ulanbaatar: 186–191. (In Russian and In Mongolian). 5. Tepkeev V.T. 2012. Kalmyki v severnom Prikaspii vo vtoroy treti XVII v.[Kalmyks in the North Caspian in the second third of the XVII century]. Elista, Dzhangar Publ.: 378 p. (In Russian). 6. Istoriya Kalmykii s drevneyshikh vremen do nashikh dney. V 3 t. [History of Kalmykia from ancient times to the present day. In three volumes. Vol. 3]. 2009. Elista, Gerel Publishing House: 848 p. (vol. 1); 840 p. (vol. 2); 752 p. (vol. 3). (In Russian). 7. Maksimov K.N. 2010. Velikaya Otechestvennaya voyna: Kalmykiya i kalmyki. 2-e izd., dop. -

The House of Soviets in Elista: Russian Constructivism and the Process of the Construction of Socialist Society
National Taiwan Normal University Graduate Institute of Art History 國立台灣師範大學藝術史研究所 Master’s Degree Thesis 碩士論文 The House of Soviets in Elista: Russian Constructivism and the Process of the Construction of Socialist Society Advisor: Candida Syndikus 指導教授: 辛蒂庫絲 博士 Graduate Student: Basan Kuberlinov 研究生: 巴桑 June 2015 中華民國 104 年 7 月 Table of Contents English Abstract………………………………………………………………………...3 Chinese Abstract………………………………………………………………………..4 1. Introduction…………………………………………………………………………5 2. State of Research……………………………………………………………………7 3. The Building History……………………………………………………………….10 a. Prehistory and Planning Process………………………………………………10 b. Construction………………………………………………………………........18 c. Destruction and Rebuilding……………………………………………………19 4. Defining a building type and its style……………………………………………...21 a. The Formal Analysis…………………………………………………………..21 b. Constructivist Houses of Soviets and the Development of a Building Type.......27 c. Golosov’s House of Soviets…………………………………………………….34 5. The Issue of Style in the House of Soviets in Elista……………………………….37 a. Constructivism, Style or Method?...................................................................... 37 b. The Origins of Iliya Golosov’s style and his Theory of the Construction……...45 of Architectural Organisms 6. The House of Soviets in Elista and Constructivism in the Context of Soviet Everyday life and Ideology…………………………………………………………54 a. The Theoretical Conception of Constructivism………………………………...54 b. Everyday life, Ideology and Theater……………………………………………60 c. The Tower……………………………………………………………………….76 -

Giant Maps Europe
KILOMETERS KILOMETERS 70° 55° 50°W 45° 40° 80° 35° 30° 25° 20° 15° 10° 5°W 0° 5°E 10° 15° 20° 25° 30° 35° 40° 45° 50° 55° 60° 65° 70° 75° 80° 85° 90° 95°E 100°E 400 300 200 100 400 300 200 100 0 0 75° 80° 75° 70° STATUTE MILES STATUTE STATUTE MILES STATUTE Ostrova Belaya Zemlya A 400 300 200 100 400 300 200 100 0 0 Ostrov Rudolph AZIMUTHAL EQUIDISTANT PROJECTION EQUIDISTANT AZIMUTHAL AZIMUTHAL EQUIDISTANT PROJECTION EQUIDISTANT AZIMUTHAL Ost Ostrov Graham rov Bell Ostrov Vize (London) J No shoes or writing utensils on map on utensils writing or shoes No ack son Meridian of Greenwich E Zemlya Wilczek n E NE W A Ostrov N NW D A N a Salisbury F Arctic Ocean Ostrov Hall I SE SW r S e O I D) c c S NW N Ostrov Arthur N t E Ostrov A S S O A NE ) i S T c Zemlya George Hooker T L SW N F W SE E E A 55° 65° A R A S A Burkhta Tikhaya F J O 65° Zemlya Alexandra A Y Z Russia L N L A N Sjuøyane E M F R U Z ( Ostrov Victoria N Lågøya Kvitøya N Storøya D T Danskøya R A I Nordaustlandet 95°E C E L Denmark A Nuuk L B Ny Ålesund A (Godth˚ab) E A E L Spitsbergen Norway Kongsøya R 50° A Prins Karls Forland Svenskøya Y L A Kong Karls R L Longyearbyen Barentsøya Land Ostrov Pankrat'yeva A E V Barentsburg E K A M A ( S G E Edgeøya S E D Z 90° K N A A Sørkappøya Hopen L E A 45° S Y N E L S C A IR E T C E N IC T E V E C B A R R A R O A R C T IC G Bjørnøya N C IR (Bear Island) 85° C L E E D e Ostrov n m a r k Belush'ya Guba S t Vaygach r a i 60° 40° t Jan Mayen E Norway Ostrov Mezhdusharskiy Vorkuta 60° A a y E h Cape a Nort k B s r N S H Berlev˚ag Kolguyev ' Ob e a E Island 80° iða i S mm l Ob fj l´o ør e e örð f øy rf a A ur na a es a E u´ Lop t E Varanger Pen. -

Download Article
Atlantis Highlights in Material Sciences and Technology (AHMST), volume 1 International Symposium "Engineering and Earth Sciences: Applied and Fundamental Research" (ISEES 2019) Air Transport in Chechen Republic: Retrospective, Condition and Development Potential [email protected] Ustaev A.L. Department of Economic and Social Geography Chechen State University Mukaeva L.A. Economic Research Laboratory Department of Economic and Social Geography Kh. Ibragimov Complex Institute of the Russian Academy Chechen State University of Sciences Grozny, Russia Grozny, Russia [email protected] Soltakhmadova L.T. Department of Economic and Social Geography Chechen State University Grozny, Russia [email protected] Abstract – The article sudies step-by-step development of air In 1990, the share of the air transport accounted for 17% of transport in the Chechen Republic. The urgency of resumption of the passenger traffic in Chechen-Ingushetia. The pilots of the both local and interregional flights is underlined. Besides, the Chechen Republic carried out a great deal of work to help article describes the impact of competition between airlines as well physicians, oil workers, forestry and agriculture, as well as to as cost related trends, the profitability of air tarnsportation, the dust the reservoirs in order to combat malaria. The pilots of the possibility of reducing airline tariffs in conditions of limited Republic treated the forests and fields with pesticides and solvent demand of residents of the Chechen Republic. There were mineral fertilizers from the air each year the area of which was defined the opportunities for the inclusion of Grozny airport into over 1 million hectares (of which 400 hectares were in the the system of international communications. -

1 Curriculum Vitae Inoue, Takehiko December 2017 Gastwissenschaftler Lehrstuhl Für Russland-/Asienstudien Ludwig-Maximilians-Un
Curriculum Vitae Inoue, Takehiko Gastwissenschaftler Lehrstuhl für Russland-/Asienstudien December 2017 Ludwig-Maximilians-Universität München Postdoctoral Research Fellow Japan Society for the Promotion of Science [email protected] Education 2014 Hokkaido University, Sapporo, Japan, Ph.D. in History and Area Studies 2011 Kalmyk State University, Elista, Russia, Research student (for a year) 2009 Saint-Petersburg State University, Saint-Petersburg, Russia, Research student (for 7 months) 2008 Moscow State University, Moscow, Russia, Research student (for two months) 2006 Kalmyk State University, Elista, Russia, Research student (for a year) 2005 Hokkaido University, M. A. in History and Area Studies 2003 Hokkaido University, B. A. in Occidental History Employment 2016-18 JSPS Postdoctoral Research Fellow, Sendai, Japan 2015 Part-time Lecturer (Economic History), Sapporo University, Sapporo, Japan 2014-15 Postdoctoral Research Fellow, Hokkaido University, Sapporo, Japan 2014-15 Part-time Lecturer (Occidental Economic History), Sapporo Gakuin University, Ebetsu, Japan 2013 Research Fellow, Japan Society for the Promotion of Science (PD) 2013 Research Fellow, Japan Society for the Promotion of Science (DC2) 2011 Research Fellow, Japan Russia Youth Exchange Center Grants and 2016-19 Grant-in-Aid for Young Scientists (B) (KAKENHI) “Research on the Fellowships Relationship between the Buddhist Monks in the Russian Empire and the National Elites in South and Southeast Asia” (Japan) 2016-18 Grant-in-Aid for JSPS Fellows (KAKENHI) “Research on -

The 5Th Congress of Russian Scholars of Religion November 26–28, 2020 Saint Petersburg the State Museum of the History of Religion
Association for Russian Centers for the Religious Studies The 5th Congress of Russian Scholars of Religion November 26–28, 2020 Saint Petersburg The State Museum of the History of Religion “RELIGION AND ATHEISM IN 21st CENTURY” Association for Russian Centers for the Religious Studies announces The 5th Congress of Russian Scholars of Religion. The 5th Congress continues the series of scholarly events being started at the 1st Congress (St. Petersburg, 2012) and afterwards kept up at the 2nd (St. Petersburg, 2014), the 3d (Vladimir, 2016) and the 4th (Blagoveshchensk, 2018) Congresses. The Congresses provides an interdisciplinary platform to discuss a great variety of problems, trends and phenomena in the field of contemporary Religious Studies, being the complex research area, methodologically based on humanities, social sciences and also, particularly during the last decades, on natural science. Previous Congresses took in participants from many cities of Russia, including Moscow, St. Petersburg, Arkhangelsk, Barnaul, Blagoveshchensk, Chita, Elista, Kazan, Khabarovsk, Krasnoyarsk, Murmansk, Nizhny Novgorod, Novgorod Veliky, Novosibirsk, Omsk, Oryol, Perm, Ryazan, Saratov, Sevastopol, Tambov, Tomsk, Tyumen, Ufa, Vladimir, Vladivostok, Volgograd, Voronezh, Yakutsk, Yaroslavl, Yekaterinburg. The scholars from Armenia, Azerbaijan, Belarus, China, Denmark, Germany, Kazakhstan, Kyrgyzstan, Latvia, Lithuania, Poland, Slovakia, Sweden, Ukraine and United Kingdom have traditionally contributed to the Congresses work. The Organizing Committee of