Some Causes of Delay in Labour; with Special Reference to the Function of the Cervical Spine of the Fcetus.”
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Ug Abuse and Dependence
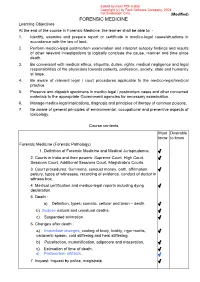
Edited by Foxit PDF Editor Copyright (c) by Foxit Software Company, 2004 For Evaluation Only. (Modified) FORENSIC MEDICINE Learning Objectives At the end of the course in Forensic Medicine, the learner shall be able to: - 1. Identify, examine and prepare report or certificate in medico-legal cases/situations in accordance with the law of land. 2. Perform medico-legal postmortem examination and interpret autopsy findings and results of other relevant investigations to logically conclude the cause, manner and time since death. 3. Be conversant with medical ethics, etiquette, duties, rights, medical negligence and legal responsibilities of the physicians towards patients, profession, society, state and humanity at large. 4. Be aware of relevant legal / court procedures applicable to the medico-legal/medical practice. 5. Preserve and dispatch specimens in medico-legal / postmortem cases and other concerned materials to the appropriate Government agencies for necessary examination. 6. Manage medico-legal implications, diagnosis and principles of therapy of common poisons. 7. Be aware of general principles of environmental, occupational and preventive aspects of toxicology. Course contents Must Desirable know to know Forensic Medicine (Forensic Pathology) 1. Definition of Forensic Medicine and Medical Jurisprudence. √ 2. Courts in India and their powers: Supreme Court, High Court, √ Sessions Court, Additional Sessions Court, Magistrate’s Courts. 3. Court procedures: Summons, conduct money, oath, affirmation, √ perjury, types of witnesses, recording of evidence, conduct of doctor in witness box, 4. Medical certification and medico-legal reports including dying √ declaration. 5. Death : a) Definition, types; somatic, cellular and brain – death. √ b) Sudden natural and unnatural deaths. √ c) Suspended animation. √ 6. -
DOA Stories and Questions
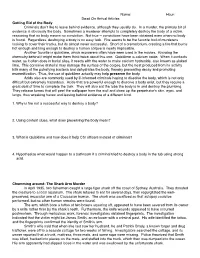
Name:_________________ Hour:_______ Dead On Arrival Articles Getting Rid of the Body !Criminals don"t like to leave behind evidence, although they usually do. In a murder, the primary bit of evidence is obviously the body. Sometimes a murderer attempts to completely destroy the body of a victim, reasoning that no body means no conviction. Not true -- convictions have been obtained even when no body is found. Regardless, destroying a body is no easy task. Fire seems to be the favorite tool of murderers looking to cover their tracks, but its almost never successful. Short of a crematorium, creating a fire that burns hot enough and long enough to destroy a human corpse is nearly impossible. !Another favorite is quicklime, which murderers often have seen used in the movies. Knowing the chemistry behind it might make them think twice about this one. Quicklime is calcium oxide. When it contacts water, as it often does in burial sites, it reacts with the water to make calcium hydroxide, also known as slaked lime. This corrosive material may damage the surface of the corpse, but the heat produced from its activity kills many of the putrefying bacteria and dehydrates the body, thereby preventing decay and promoting mummification. Thus, the use of quicklime actually may help preserve the body. !Acids also are commonly used by ill-informed criminals hoping to dissolve the body, which is not only difficult but extremely hazardous. Acids that are powerful enough to dissolve a body exist, but they require a great deal of time to complete the task. -

Forensic Medicine and Toxicology
FORENSIC MEDICINE AND TOXICOLOGY CURRICULUM OF SYLLABUS UNDER THE NEW REGULATIONS FOR THE MBBS. COURSES OF STUDIES EFFECTIVE FROM THE SESSION: 2017-18 . 3RD SEMESTER: 1.INTRODUCTION (1hr) a. Definitions: forensic medicine, state medicine, legal medicine, medical jurisprudence, medical ethics, medical etiquette b. Various branches of forensic science. c. History and evolution of forensic medicine from ancient period to modern period 2.LEGAL PROCEDURE (2hr) a. Definition: bill, act, code, court, law, statutory law b. Major codes and acts: Indian Penal Code (IPC), Criminal Procedure Code (Cr.PC), Indian Evidence Act c. Different Courts of Law, their structure and functions: Supreme Court, High Court, Sessions Court, Judicial Magistrate Courts d. Offences: cognizable/non-cognizable, bailable/non-bailable, warrant case, summon case e. Different types of punishments authorized by law f. Inquest: definition, types and procedure of different inquests [police inquest, magistrate inquest (executive and judicial magistrate inquest), coroner’s inquest, medical examiner’s system] g. Summon: definition, types, salient features h. Conduct money i. Medical evidence: definition, types (documentary and oral), documentary evidence (defn, types of medical documentary evidences), special emphasis on ‘how to record dying declaration’, oral evidence (defn, exception to oral evidence), direct evidence, indirect evidence (circumstantial and hearsay) j. Chain of custody k. Witness: definition, types, hostile witness and perjury l. Procedure of recording of evidence in Court of law: starting from receiving a summon, oath taking, examination in chief, cross examination, re-examination, question by the Judge, checking the written form of oral evidence by the doctor, Court attendance certificate m. Conduct and duties of a doctor in witness box n. -

A Denial the Death of Kurt Cobain the Seattle Police Department
A Denial The Death of Kurt Cobain The Seattle Police Department Substandard Investigation & The Repercussions to Justice by Bree Donovan A Capstone Submitted to The Graduate School-Camden Rutgers, The State University, New Jersey in partial fulfillment of the requirements for the degree of Masters of Arts in Liberal Studies Under the direction of Dr. Joseph C. Schiavo and approved by _________________________________ Capstone Director _________________________________ Program Director Camden, New Jersey, December 2014 i Abstract Kurt Cobain (1967-1994) musician, artist songwriter, and founder of The Rock and Roll Hall of Fame band, Nirvana, was dubbed, “the voice of a generation”; a moniker he wore like his faded cardigan sweater, but with more than some distain. Cobain‟s journey to the top of the Billboard charts was much more Dickensian than many of the generations of fans may realize. During his all too short life, Cobain struggled with physical illness, poverty, undiagnosed depression, a broken family, and the crippling isolation and loneliness brought on by drug addiction. Cobain may have shunned the idea of fame and fortune but like many struggling young musicians (who would become his peers) coming up in the blue collar, working class suburbs of Aberdeen and Tacoma Washington State, being on the cover of Rolling Stone magazine wasn‟t a nightmare image. Cobain, with his unkempt blond hair, polarizing blue eyes, and fragile appearance is a modern-punk-rock Jesus; a model example of the modern-day hero. The musician- a reluctant hero at best, but one who took a dark, frightening journey into another realm, to emerge stronger, clearer headed and changing the trajectory of his life. -

Lawyer's Guide to Forensic Medicine
LAWYER’S GUIDE TO FORENSIC MEDICINE CP Cavendish Publishing Limited London • Sydney LAWYER’S GUIDE TO FORENSIC MEDICINE Second Edition Bernard Knight, CBE, MD, DSc (Hon), LLD (Hon), BCh, MRCP, FRCPath, Dip Med Jur Barrister of Gray’s Inn Emeritus Professor of Forensic Pathology, University of Wales College of Medicine CP Cavendish Publishing Limited London • Sydney Published in Great Britain 1998 by Cavendish Publishing Limited, The Glass House, Wharton Street, London WC1X 9PX, United Kingdom. Telephone: +44 (0) 171 278 8000 Facsimile: +44 (0) 171 278 8080 E-mail: [email protected] Visit our Home Page on http://www.cavendishpublishing.com First published by William Heinemann Medical Books 1982 © Knight, Bernard 1998 First edition 1982 Second edition 1998 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording, scanning or otherwise, except under the terms of the Copyright Designs and Patents Act 1988 or under the terms of a licence issued by the Copyright Licensing Agency, 90 Tottenham Court Road, London W1P 9HE, UK, without the permission in writing of the publisher. Knight, Bernard Lawyer’s Guide to Forensic Medicine – 2nd edn 1. Medical jurisprudence I. Title 614.1 ISBN 1 85941 159 2 Printed and bound in Great Britain PREFACE The 16 years that have elapsed since the first edition of this book have seen many changes which require significant updating of the text. Some entries have been deleted and others added, to reflect the changing priorities in the interface between medicine and the law. -

Hijikata Tatsumi's Sabotage of Movement and the Desire to Kill The
Death and Desire in Contemporary Japan Representing, Practicing, Performing edited by Andrea De Antoni and Massimo Raveri Hijikata Tatsumi’s Sabotage of Movement and the Desire to Kill the Ideology of Death Katja Centonze (Universität Trier, Deutschland; Waseda University, Japan) Abstract Death and desire appear as essential characteristics in Hijikata Tatsumi’s butō, which brings the paradox of life and death, of stillness and movement into play. Hijikata places these con- tradictions at the roots of dance itself. This analysis points out several aspects displayed in butō’s death aesthetics and performing processes, which catch the tension between being dead and/or alive, between presence and absence. It is shown how the physical states of biological death are enacted, and demonstrated that in Hijikata’s nonhuman theatre of eroticism death stands out as an object aligned with the other objects on stage including the performer’s carnal body (nikutai). The discussion focuses on Hijikata’s radical investigation of corporeality, which puts under critique not only the nikutai, but even the corpse (shitai), revealing the cultural narratives they are subjected to. Summary 1 Deadly Erotic Labyrinth. – 2 Death Aesthetics for a Criminal and Erotic Dance. – 3 Rigor Mortis and Immobility. – 4 Shibusawa Tatsuhiko. Performance as Sacrifice and Experience. – 5 Pallor Mortis and shironuri. – 6 Shitai and suijakutai. The Dead are Dancing. – 7 The Reiteration of Death and the miira. – 8 The shitai under Critique. Death and the nikutai as Object. – 9 Against the Ideology of Death. Keywords Hijikata Tatsumi. Butō. Death. Eroticism. Corporeality. Acéphale. Anti-Dance. Body and Object. Corpse. Shibusawa Tatsuhiko. -

Buried but Alive?
Buried but Alive? Interpreting Post-depositional Bone Movement, Anxieties over Death and Premature Burial BY SIAN ANTHONY Abstract The young, beautiful and wealthy widow Giertrud Birgitte Bodenhoff was buried in Assistens cemetery, Copenhagen on 23 July 1798 but was she dead? Family stories claimed she had been buried alive but was found by grave-robbers who then killed her to conceal their crime. Her skeleton was exhumed in 1953 and the unexpected position of it within the coffin was used to confirm the stories, which echo many similar narratives that betray anxieties over death and premature burial. With advances in archaeological methods and forensic taphonomy, this conclusion requires reinterpretation. The burial environment is not static and the body and later the skeleton can move while undergoing the de- cay process. The position of the skeleton in burials excavated in the same cemetery from 2009–11 is used to review the Bodenhoff story. How does decomposition move the bones within a well-preserved coffin? Can some typical movements of bones in coffins be identified in Assistens to advance greater understanding of what happens underground in the coffin? Introduction Gothic literature and popular culture are full collected as evidence that premature burial of premature burials, but the fear of being was a common phenomenon (e.g. Tebb & buried alive is also a long-held fascination Vollum 1896). The behaviour of people, as in the western world, with stories attested told in the stories, suggests a malleable sense from the Classical period onwards. There of death where it is a reversible and porous was a particular peak of interest in the 18th state (Ariès 1981, 609) in contrast to a finite and 19th centuries (Bondesen 2001, 77 medical state. -

"FINAL DESTINATION" Originally Called "FLIGHT 180"
"FINAL DESTINATION" Originally Called "FLIGHT 180" By James Wong and Glen Morgan January 15, 1999 Awaiting......each of us; a cold...dark...lonely place. Deny its finality. Deride its totality. Dread the inescapable inevitability......it will arrive. The BLACK SILENT SCREEN senses this moment before a distant blues harp introduces a contemporary band's cover of Blood, Sweat, and Tears' campy, yet haunting, gospel, "And When I Die." As the Introduction closes, RESONATES... A FLASH OF LIGHTING! A CRACK OF THUNDER! CUT TO: INT. ALEX'S BEDROOM - NIGHT - CLOSE - BED An airline ticket is tossed INTO FRAME beside a suitcase; "EURO-AIR. FLIGHT #180. New York City (JFK) - Paris, Charles de Gaulle (CDG.) Departure: Thursday 13May. 16H25 - Arrival: Friday 14May. 05H40." "And When I Die" Continues throughout the MAIN TITLES: AN OLD TABLE FAN swivels beside and open window. Outside, a humid spring THUNDER STORM drops warm, ominous rain. The figure of a seventeen year old boy, ALEX BROWNING, packing for a trip, passing the fan... THE BED A Paris guidebook is tossed atop the plane ticket. CAMERA PUSHES IN ON THE BOOK as the fan's breezes flip through the pages. THE TABLE FAN turns, head swiveling away from the bed. TIGHTER - THE GUIDEBOOK PAGES stop flipping, REVEALING A GULLOTINE from the Reign of Terror. As an American passport is dropped beside the guidebook... THE TABLE FAN swivels, returning towards the guidebook on the bed. THE GUIDEBOOK PAGES FLIP. FLIP. FLIP. Alex's faint shadow continues moving about the room. The fan head swivels away, allowing the pages to settle.. -

FORENSIC MEDICINE QP Code
[LK 546] FEBRUARY 2017 Sub. Code : 5067 M.B.B.S. DEGREE EXAMINATION SECOND YEAR PAPER VII – FORENSIC MEDICINE Q.P. Code: 525067 Time: Three hours Maximum : 40 Marks I. Elaborate on: (1 x 10 = 10) 1. Define and classify injury. Describe the types and medico legal importance of abrasions. II. Write notes on: (4 x 5 = 20) 1. Inquest. 2. Post-mortem hypostasis. 3. Intracranial hemorrhage. 4. Antidotes. III. Short answers on: (5 x 2 = 10) 1. Tattoo marks. 2. Professional death sentence. 3. Necrophilia. 4. Dry drowning. 5. Cardiac poisons. ******** [LL 546] AUGUST 2017 Sub. Code : 5067 M.B.B.S. DEGREE EXAMINATION SECOND YEAR PAPER VII – FORENSIC MEDICINE Q.P. Code: 525067 Time: Three hours Maximum : 40 Marks I. Elaborate on: (1 x 10 = 10) 1. Define and classify asphyxia. Write in detail about the types and post-mortem findings of hanging. II. Write notes on: (4 x 5 = 20) 1. Witnesses. 2. Hallucination. 3. Laceration. 4. Hydrocyanic acid poisoning. III. Short answers on: (5 x 2 = 10) 1. Cadaveric spasm. 2. Avulsion. 3. Whiplash injury. 4. Bestiality. 5. Lysergic acid diethylamide (LSD). ******** [LM 546] FEBRUARY 2018 Sub Code: 5067 M.B.B.S. DEGREE EXAMINATION SECOND YEAR PAPER VII – FORENSIC MEDICINE Q.P. Code: 525067 Time: Three hours Maximum : 40 Marks I. Elaborate on: (1 x 10 = 10) 1. Elaborate the signs, symptoms, treatment, autopsy findings and medicolegal aspects of carbon monoxide poisoning. II. Write notes on: (6 x 4 = 24) 1. Subpoena. 2. Virtual autopsy. 3. Sudden death. 4. Diatoms test. 5. The medical termination of pregnancy act 1971. -
Resuscitation Policy and Recognition of Life Extinct
RESUSCITATION POLICY AND RECOGNITION OF LIFE EXTINCT South Central Ambulance Service NHS Foundation Trust Unit 7 & 8, Talisman Business Centre, Talisman Road, Bicester, Oxfordshire, OX26 6HR This Policy is to be read in conjunction with Operational Policies and Procedures No 7 - SCAS Attendance at Sudden Death in Adults (Appendix 8) DOCUMENT INFORMATION Author: Dave Sherwood, Assistant Director of Patient Care Professor Charles Deakin, Divisional Medical Director Resuscitation Lead Reviewed 22nd January 2020 Mark Ainsworth-Smith Jennifer Saunders Number CSPP No. 3 Consultation & Approval: Staff Consultation Process: (21 days) ends 19th Oct 2007 Clinical Review Group: 2nd July 2020 Quality and Safety Committee: 5th June 2010 Board Ratification: N/A This document replaces: SCAS Recognition of Life Extinct Policy Version 1 June 2007 Notification of Policy Release: All Recipients e-mail Staff Notice Boards Intranet Equality Impact Assessment Stage 1 Assessment undertaken – no issues identified Date of Issue: July 2020 Next Review: July 2022 Version: 7 Contents DOCUMENT INFORMATION ............................................................................................................................. 2 1. INTRODUCTION .................................................................................................................................. 3 2.0 DUTIES ................................................................................................................................................. 3 3.0 TRAINING STRATEGY ....................................................................................................................... -

Postmortem Changes and Time of Death
POSTMORTEM CHANGES AND TIME OF DEATH Quotations "The time of death is sometimes extremely important. It is a question almost invariably asked by police officers, sometimes with a touching faith in the accuracy of the estimate. Determining the time of death is extremely difficult, and accuracy is impossible". (Ref. 8 at p. 115.) "No problem in forensic medicine has been investigated as thoroughly as that of determining the time of death on the basis of post mortem findings. Apart from its obvious legal importance, its solution has been so elusive as to provide a constant intellectual challenge to workers in many sciences. In spite of the great effort and ingenuity expended, the results have been meagre". (Ref. 15 at p. 33.) "Repeated experience teaches the investigator to be wary of relying on any single observation for estimating the time of death (or "duration of the post mortem interval"), and he wisely avoids making dogmatic statements based on an isolated observation". (Ref. 12 at p. 151.) "Considering the variables which influence the rate of body heat loss, the best one can say about the reliability of algor mortis as a post mortem clock is that it permits a rough approximation of the time of death. Errors in over-estimating and under-estimating the post mortem interval based on body cooling are common, even in the face of considerable experience by those making the estimate. Body temperature as an indicator of the post mortem interval should be correlated with all other phenomenon and observations utilised in establishing the time of death". (Ref. -

Whence This Severance of the Head?”: the Osteology and Archaeology of Human Decapitation in Britain
UNIVERSITY OF WINCHESTER FACULTY OF HUMANITIES AND SOCIAL SCIENCES “Whence this Severance of the Head?”: The Osteology and Archaeology of Human Decapitation in Britain KATIE TUCKER Thesis submitted for the degree of Doctor of Philosophy January 2012 UNIVERSITY OF WINCHESTER ABSTRACT FACULTY OF HUMANITIES AND SOCIAL SCIENCES Doctor of Philosophy “Whence this Severance of the Head?”: The Osteology and Archaeology of Human Decapitation in Britain Katie Tucker Decapitation burials (burials in which the cranium and mandible are displaced from correct anatomical position and replaced elsewhere in the grave) are a relatively common minority burial practice in Romano-British cemeteries. They have usually been ascribed to a post-mortem funerary ritual with various different motives being postulated. However, these interpretations seem to have largely been based on assumption rather than evidence from the archaeological context or the human remains, only small numbers of which have been subjected to detailed skeletal analysis. Decapitated burials are also found in the early medieval period, and, conversely, these are normally concluded to be the victims of judicial execution, an interpretation that is only very rarely used when discussing Romano-British examples. This thesis examines the archaeological and osteological data from a large sample of Romano- British decapitated burials and compares them with the wider Romano-British cemetery population, in order to better understand the differences between decapitated individuals and the rest of the population, in terms of burial practice, demographics, and ante-mortem health status. The evidence for decapitation in the Neolithic, Bronze and Iron Ages, early medieval, medieval and post-medieval periods was also examined, with the analysis of samples of decapitated individuals being undertaken where possible, in order to provide comparanda for the Romano- British examples, and assess whether there is any evidence for continuity in the practice between the periods.