SARS-Cov-2 Test Positivity Rate in Reno, Nevada: Association With
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
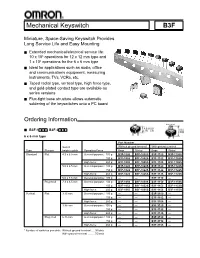
Mechanical Keyswitch B3F
Mechanical Keyswitch B3F Miniature, Space-Saving Keyswitch Provides Long Service Life and Easy Mounting ■ Extended mechanical/electrical service life: 10 x 106 operations for 12 x 12 mm type and 1 x 106 operations for the 6 x 6 mm type ■ Ideal for applications such as audio, office and communications equipment, measuring instruments, TVs, VCRs, etc. ■ Taped radial type, vertical type, high force type, and gold-plated contact type are available as series versions ■ Flux-tight base structure allows automatic soldering of the keyswitches onto a PC board Ordering Information Flat Projected ■ B3F-1■■■, B3F-3■■■ 6 x 6 mm type Part Number Switch Without ground terminal With ground terminal Type Plunger height x pitch Operating Force Bags Sticks* Bags Sticks* Standard Flat 4.3 x 6.5 mm General-purpose: 100 g B3F-1000 B3F-1000S B3F-1100 B3F-1100S 150 g B3F-1002 B3F-1002S B3F-1102 B3F-1102S High-force: 260 g B3F-1005 B3F-1005S B3F-1105 B3F-1105S 5.0 x 6.5 mm General-purpose: 100 g B3F-1020 B3F-1020S B3F-1120 B3F-1120S 150 g B3F-1022 B3F-1022S B3F-1122 B3F-1122S High-force: 260 g B3F-1025 B3F-1025S B3F-1125 B3F-1125S 5.0 x 7.5 mm General-purpose: 100 g — — B3F-1110 — Projected 7.3 x 6.5 mm General-purpose: 100 g B3F-1050 B3F-1050S B3F-1150 B3F-1150S 150 g B3F-1052 B3F-1052S B3F-1152 B3F-1152S High-force: 260 g B3F-1055 B3F-1055S B3F-1155 B3F-1155S Vertical Flat 3.15 mm General-purpose: 100 g — — B3F-3100 — 150 g — — B3F-3102 — High-force: 260 g — — B3F-3105 — 3.85 mm General-purpose: 100 g — — B3F-3120 — 150 g — — B3F-3122 — High-force: 260 g — — B3F-3125 — Projected 6.15 mm General-purpose: 100 g — — B3F-3150 — 150 g — — B3F-3152 — High-force: 260 g — — B3F-3155 — * Number of switches per stick: Without ground terminal ... -
Herefore, Incentives Typically Offered and Used for Development Would Be Replaced with the EB-5 Investment
Revised – 9/18/17 CITY OF YPSILANTI REGULAR COUNCIL MEETING CITY COUNCIL CHAMBERS – ONE SOUTH HURON ST. YPSILANTI, MI 48197 TUESDAY, SEPTEMBER 19, 2017 7:00 p.m. I. CALL TO ORDER – II. ROLL CALL – Council Member Bashert P A Council Member Robb P A Mayor Pro-Tem Brown P A Council Member Vogt P A Council Member Murdock P A Mayor Edmonds P A Council Member Richardson P A III. INVOCATION – IV. PLEDGE OF ALLEGIANCE – “I pledge allegiance to the flag, of the United States of America, and to the Republic for which it stands, one nation, under God, indivisible, with liberty and justice for all.” V. AGENDA APPROVAL – VI. INTRODUCTIONS – VII. AUDIENCE PARTICIPATION – VIII. REMARKS BY THE MAYOR – IX. PUBLIC HEARING – International Village - Water Street A. Resolution No. 2017-208, approving purchase agreement. B. Open public hearing C. Resolution No. 2017-209, close public hearing X. PRESENTATIONS – Discussion of Easement Agreement with Michigan Advocacy Program on 15 N. Washington. XI. ORDINANCES – FIRST READING – Ordinance No. 1294 An ordinance to rezone 75 Catherine from Core Neighborhood to Production, Manufacturing & Distribution. A. Resolution No. 2017-210, determination B. Open public hearing C. Resolution No. 2017-211, close public hearing 1 XII. CONSENT AGENDA – Resolution No. 2017-212 1. Resolution No. 2017–213, approving minutes of August 22 and September 5, 2017. 2. Resolution No. 2017-214, approving the issuance of a blanket permit for window signs of any size for the month of October for businesses that participate with the Eastern Michigan University’s “Follow the Green & White Road” homecoming spirit project. -
NCUA 5300 Call Report Account Descriptions Page 1 of 42 Effective
NCUA 5300 Call Report Account Descriptions Account Code Account Description Page 002 Amount of Leases Receivable 6 003 Loans Held for Sale 1 007 Land and Building 2 008 Other Fixed Assets 2 009 Total Other Assets 2 009A Accrued Interest on Loans 2 009B Accrued Interest on Investments 2 009C All Other Assets 2 009D Total Intangible Assets 2 009D1 Identifiable Intangible Assets 2 009D2 Goodwill 2 009E Non-Trading Derivative Assets, net 2 010 TOTAL ASSETS 2 010 TOTAL ASSETS 12 010 TOTAL ASSETS 13 010A Average of Daily Assets over the calendar quarter 12 010B Average of the three month-end balances over the calendar quarter 12 010C The average of the current and three preceding calendar quarter-end balances 12 011A Other Notes, Promissory Notes and Interest Payable < 1 Year 3 011B1 Other Notes, Promissory Notes and Interest Payable 1 - 3 Years 3 011B2 Other Notes, Promissory Notes and Interest Payable > 3 Years 3 011C Total Other Notes, Promissory Notes and Interest Payable 3 013 Total Shares 3 013A Total Shares < 1 Year 3 013B1 Total Shares 1 - 3 Years 3 013B2 Total Shares > 3 Years 3 014 TOTAL LIABILITIES, SHARES, AND EQUITY 4 018 Total Shares and Deposits 3 018A Total Shares and Deposits < 1 Year 3 018B1 Total Shares and Deposits 1 - 3 Years 3 018B2 Total Shares and Deposits > 3 Years 3 020A Total number of Delinquent Loans 30 to 59 Days 8 020B Total Delinquent Loans 30 to 59 Days 8 020C Amount of All Other Non-Real Estate Loans 30 to 59 days delinquent 8 020C1 Amount of New Vehicle Loans Delinquent 30 to 59 days 8 020C2 Amount of Used -

Electric Actuators Vsi-1000 Series
ELECTRIC ACTUATORS TM VSI-1000 SERIES DESCRIPTION VSI-1000 Series Electric Actuators are used on Kele KBV Series butterfly valves to provide two-position (with or without battery backup) or proportional control in a NEMA 4X housing. The VSI-1000 Series comes standard on 8" and larger non-spring return assemblies and on 5" and larger two- position spring return assemblies. They can be ordered on smaller valve assemblies as an option. Standard fea- tures include 2 SPDT fully adjustable auxiliary switches KBV-2-6-E2SO (two-position only), manual override crank, and an inter- assembly includes nal heater to prevent condensation in outdoor installa- VSI-BB1020 actuator tions. SPECIFICATIONS FEATURES Power 120 VAC standard •Lightweight, compact design Models 1005 to 1020 12/24 VDC optional • Two-position or modulating control Models 1005 to 1040 24 VAC optional • Two-position battery-backed models Torque range 347-17,359 in-lb • NEMA 4X watertight, corrosion-resistant housing Motor 120 VAC, 1 phase, 60 Hz; • Integral position indicator enclosed, non-ventilated, high • Space heater standard starting torque, reversible induc- • Two 1/2" conduit connections tion, Class E insulation • Detachable manual override crank Thermal overload Auto reset, embedded • Terminal strip wiring Travel limit switches Cam operated, adjustable SPDT • Worm gear drive, no electro-mechanical brake for open/close stop required • Mounting orientation in any direction Position indicator High-visibility graduated dial • 4-20 mA or 500Ω optional feedback signal Conduit connections -

Norman Identity and Historiography in the 11Th-12Th Centuries
Butler Journal of Undergraduate Research Volume 5 2019 The Comedia Normannorum: Norman Identity and Historiography in the 11th-12th Centuries Patrick Stroud Wabash College Follow this and additional works at: https://digitalcommons.butler.edu/bjur Recommended Citation Stroud, Patrick (2019) "The Comedia Normannorum: Norman Identity and Historiography in the 11th-12th Centuries," Butler Journal of Undergraduate Research: Vol. 5 , Article 10. Retrieved from: https://digitalcommons.butler.edu/bjur/vol5/iss1/10 This Article is brought to you for free and open access by the Undergraduate Scholarship at Digital Commons @ Butler University. It has been accepted for inclusion in Butler Journal of Undergraduate Research by an authorized editor of Digital Commons @ Butler University. For more information, please contact [email protected]. BUTLER JOURNAL OF UNDERGRADUATE RESEARCH, VOLUME 5 THE COMEDIA NORMANNORUM: NORMAN IDENTITY AND HISTORIOGRAPHY IN THE 11TH-12TH CENTURIES PATRICK STROUD, WABASH COLLEGE MENTOR: STEPHEN MORILLO Introduction—How Symbols and Ethnography Tie to Historical Myth Since the 1970s, historians have tried many different methodologies for exploring texts. Because multiple paradigms tempt the historian’s gaze, medieval texts can often befuddle readers in their hagiographies and chronologies. At the same time, these texts also give the historian a unique opportunity in the form of cultural insight. In his 1995 work Making History: The Normans and their Historians in Eleventh-Century Italy, Kenneth Baxter Wolf discusses a text’s role in medieval historiography. A professor of History at Pomona College, Wolf divides historical commentary on medieval primary sources into two ends of a spectrum. While one end worries itself on the accuracy and classical “truth” of a source, the other end, postmodern historiography, uses historical records “to tell us how the people who wrote them conceived of the events occurring in the world around them.”1 The historian treats a medieval text as a launching pad for cultural analysis. -
2020 Ambient Air Monitoring Network 5-Year Assessment
State of Hawaii 2020 Ambient Air Monitoring Network 5-Year Assessment Prepared by: State of Hawaii Department of Health Environmental Management Division Clean Air Branch July 1, 2020 Document No. CABMA-5YRA-2020-v01 Table of Contents List of Tables .......................................................................................................... iii List of Figures .......................................................................................................... iii Abbreviations and Definitions .................................................................................. iv I. Executive Summary ................................................................................................. 1 A. Purpose of Assessment .................................................................................... 1 B. Ambient Air Monitoring Networks ...................................................................... 1 C. Summary of 2015 Findings ............................................................................... 1 II. Introduction .............................................................................................................. 3 III. Current Air Monitoring in the State of Hawaii ........................................................... 4 IV. Climate, Population and Emission Source Characteristics ...................................... 7 A. Climate and Topography ................................................................................... 7 B. Population ...................................................................................................... -
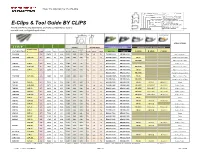
E-Clips & Tool Guide by CLIPS
Phone: 714 809-0194 | Fax: 714 373-4808 3 F = 4" (19.0 mm) XX = LENGTH in 100ths/inch A = 7 / /16" (11.0 mm) A-H = CLIP WIDTH 11 7 E = /16" (17.5 mm) H = /8" (22.0 mm) A-H ZZ = OPENING in 100th s/inch (BLANK) = COLD ROLLED STEEL XX TYPE OF PACKAGING 1006-1010 A = ALUMINUM S–STRIPS CLP–STRIPS C = CUSHIONED (PAPER LINING INSIDE) R–ROLLS CCP–ROLLS G = GALVANIZED L = 4 MIL PVC VINYL COATING E-Clips & Tool Guide BY CLIPS B–BULK (INSIDE) S = STAINLESS STEEL (430) MATERIAL (BLANK) or P = POLYCORD Encore and Hartco clip equivalents, pack/ship configurations, tools to ZZ DESIGNATIONS 74 H 18 S G T = TAPED COLLATION D = DETENT use with each, and typical applications W D PARTS SUPPORT ONLY H APPLICATIONS S T R I P INCHES MILLIMETERS ECLIPSER 2000 SERIES GENUINE HARTCO CLINCH TOOLS HARTCO Clip DEPT ENCORE E-Clip # # #/STRIP CLIPS/CTN LBS/CTN KGS/CTN HEIGHT WIDTH H HEIGHT WIDTH DEPTH ENCORE HARTCO A SERIES B SERIES C SERIES** 52A14SG – 58 15,834 25 11.4 0.32 0.40 0.20 8.2 10 5.1 EA2000-1234 HR2000-1234 0 0 0 Cages, Traps & Wires 64A18SG CLP-15G 47 10,857 24 10.9 0.41 0.43 0.26 10.4 11 6.6 EA2000-1020S HR2000-1020S HR-45i 0 0 Housing Panels, Cages, Cables 64A18SG CLP-15G 47 10,857 24 10.9 0.41 0.43 0.26 10.4 11 6.6 EA2000-1929 HR2000-1929 HR-45TN 0 0 Tight Access Cages & Traps 68H18S CLP-22 47 4,700 22 10.0 0.47 0.86 0.26 11.9 22 6.6 EA2000-6075 HR2000-6075 0 0 0 Bedding, Furniture 71A16SAL CLP-13AL 47 9,400 22 10.0 0.45 0.43 0.26 11.4 11 6.6 EA2000-1929 HR2000-1929 HR-45TN 0 0 Tight Access Cages & Traps 71A18S CLP-13 47 9,400 22 10.0 0.45 0.43 0.26 -

Peter the Hermit: Straddling the Boundaries of Lordship, Millennialism, and Heresy Stanley Perdios Iowa State University
Iowa State University Capstones, Theses and Graduate Theses and Dissertations Dissertations 2012 peter the hermit: straddling the boundaries of lordship, millennialism, and heresy Stanley Perdios Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/etd Part of the European History Commons, and the Religion Commons Recommended Citation Perdios, Stanley, "peter the hermit: straddling the boundaries of lordship, millennialism, and heresy" (2012). Graduate Theses and Dissertations. 12431. https://lib.dr.iastate.edu/etd/12431 This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. Peter the Hermit: Straddling the boundaries of lordship, millennialism, and heresy by Stelios Vasilis Perdios A thesis submitted to the graduate faculty in partial fulfillment of the requirements for the degree of MASTER OF ARTS Major: History Program of Study Committee: Michael D. Bailey, Major Professor John W. Monroe Jana Byars Kevin Amidon Iowa State University Ames, Iowa 2012 Copyright © Stelios Vasilis Perdios, 2012. All Rights reserved. ii Table of Contents Chapter Page Chapter One: Introduction 1 Chapter Two: The Crisis of Secular Lordship 7 Chapter Three: The Crisis of Spiritual Lordship 35 Chapter Four: Lordship on the Eve of the Millennium 65 Chapter Five: Conclusion 95 Bibliography 99 1 Chapter One: Introduction When is a hermit not a hermit? When he is Peter the Hermit who led the Popular Crusade in the year 1096. -

3.2 Precipitation Or Dry-Wet Reconstructions
Climate change in China during the past 2000 years: An overview Ge Quansheng , Zheng Jingyun Institute of Geographic Sciences and Natural Resources Research, Chinese Academy of Sciences, Beijing 100101, China Email: [email protected] Outline 1 Introduction 2 Historical Documents as Proxy 3 Reconstructions and Analyses 4 Summary and Prospects 1. Introduction: E Asia2K Climate System Socio-economic System •typical East Asian •dense population and rapid monsoon climate economic development • significant seasonal and • be susceptible to global inter-annual and inter- warming and extreme decadal variability climate events Climate change study in the past 2ka in East Asian is both beneficial and advantageous. • various types of natural proxy • Plenty of historical documents Fig. Active regional working groups under as proxy the past 2ka theme (PAGES 2009) 2. Historical Documents as Proxy Type Period Amount Chinese classical 1,531 kinds, 137 BC~1470 AD documents 32,251 volumes More than 8,000 1471~1911 (The Ming Local gazettes books (部), 110, and Qing Dynasty) 000 volumes Memos to the About 120,000 1736~1911 emperor pieces Archives of the 1912~1949 20,000 volumes Republic of China More than 200 Private diaries 1550~ books (部) Chinese classical documents AD 833, North China plain: Extreme drought event was occurred, crops were shriveling, no yields, people were in hungry…. Fig. Example for Ancient Chinese writings Local gazettes The 28th year of the Daoguang reign (1848 AD), the 6th (lunar) month, strong wind and heavy rain, the Yangtze River overflowed; the 7th month, strong wind Fig. Gazettes of Yangzhou Prefecture and thunder storm, field published in 1874 AD and houses submerged. -

Body Wave Analyses of Strain Seismograms Observed at Erimo, Hokkaido, Japan
Title Body Wave Analyses of Strain Seismograms Observed at Erimo, Hokkaido, Japan Author(s) KASAHARA, Minoru; SASATANI, Tsutomu Citation Journal of the Faculty of Science, Hokkaido University. Series 7, Geophysics, 8(1), 83-108 Issue Date 1986-02-26 Doc URL http://hdl.handle.net/2115/8754 Type bulletin (article) File Information 8(1)_p83-108.pdf Instructions for use Hokkaido University Collection of Scholarly and Academic Papers : HUSCAP Jour. Fac. Sci., Hokkaido Univ., Ser. VII (Geophysics), Vol. 8, No.1, 83-108, 1986. Body Wave Analyses of Strain Seismograms Observed at Erimo, Hokkaido, Japan Minoru Kasahara Research Center for Earthquake Prediction, Faculty of Science, Hokkaido University, Sapporo 060, Japan and Tsutomu Sasatani Department of Geophysics, Faculty of Science, Hokkaido University, Sapporo 060, Japan (Received November 25, 1985) Abstract At the Erimo Geophysical Observatory (EGO) a digital recording system has been introduced on July, 1976 into the Earth strain measurements in order to use the fused quartz extensometer of 30 m long as a seismometer. The body wave parts of the strain seismograms from 14 earthquakes with magnitudes ranging from 4.7 to 7.7 recorded by the system were compared with the synthetic strain seismograms generat ed by a point shear dislocation in an infinite homogeneous medium. The waveform and amplitude of the observed strain seismogram could be well explained by the synthetic one calculated for appropriate source parameters deduced from the conven tional method. Based on this result it can be shown that the period of the observed S-wave approximately represents the source process time of an earthquake and the S-wave amplitude is proportional to the seismic moment of the event. -

Series 1000 Electric Actuators Series 1000 Electric Actuators Design Features
SERIES 1000 ELECTRIC ACTUATORS SERIES 1000 ELECTRIC ACTUATORS DESIGN FEATURES Series 1000 On-Off Rotary Electric Actuator Basic Actuator: Torque Output Range: 347in-lb to 17,359in-lb Housing: NEMA 4X, watertight, corrosion-resistant, robust aluminum die cast Electric Motor: 10VAC, single phase, 60Hz totally enclosed, non-ventilated, high starting torque, reversible induction type, Class F insulation Thermal Overload Motor Protection: Auto reset thermal switch embedded in the motor winding - trips when the maximum winding temperature is exceded Position Limit Switches: x SPDT for Open and Close travel limit - easily adjustable, cam operated Position Indicator: Mechanical dome type with visiable red/yellow closed/open indicator Terminal Strip: Refer to wiring diagrams for details Conduit Entries: 1 x 1/” NPT for power and control wiring Power Gears: Alloy steel spur gears to final stage aluminum bronze worm sector gear Break: An electro-mechanical brake is NOT required. The worm gear drive prevents back driving and hunting Bearings: High quality alloy steel sleeve and ball bearings Manual Override: Handle Adjustable Mechanical Stops Ambient Temperature Range: -31°F to +150°F Certification and Approvals:CE, NEMA4, CSA, NRTL Internal Heater Optional Features • 0V AC/1/50-60Hz power • 1/4V DC 1005 through 100 • Torque Limit Switches for Close direction of travel • Feedback Potentiometer - 1000ohm • DeClutchable Handwheel Override SERIES 1000 ELECTRIC ACTUATORS ON-OFF SPECIFICATIONS Series 1000 On-Off Actuator Specifications Model 1005 1010 1020 1040 1060 1100 1150 1200 Output Torque(in-lb) 347 868 1736 347 508 8680 13,019 17,359 Output Torque(Nm) 39.3 98.06 196.13 39.7 588.4 980.66 1471 1961.3 Duty Cycle 75% 75% 50% 50% 50% 50% 50% 50% Travel Speed at 5 5 5 5 50 50 50 50 60Hz(Sec) Maximum Current .35/.18 .41/. -
DSX Modem Installation Manual
® DSX Modem Installation Manual DSX Access Systems, Inc. 10731 Rockwall Road Dallas, Texas 75238 888-419-8353 Sales, Shipping and Accounting 800-346-5288 Technical Support 214-553-6140 Phone www.dsxinc.com 214-553-6147 FAX Modem 02/05 DSX Access Systems, Inc. 10731 Rockwall Road Dallas, Texas 75238 888-419-8353 Sales, Shipping and Accounting 800-346-5288 Technical Support 214-553-6140 Phone www.dsxinc.com 214-553-6147 FAX Modem 02/05 Table of Contents Modem Operation Overview……………………………………………………………………………1 Modem recommendation…………………………………………………………………………….….2 Phone Call Description………………………………………………………………………………….2 Communication Security Password (Location Password)………………………………………………3 DSX Modem LED Operation.……………………………………………………………………….….4 Modem to PC Connections…………………………………………………………………………….. 4 Modem Power Sources………………………………………………………………………………….5 Modem Mounting in DSX Enclosures………………………………………………………………….5 Modem to DSX-1040, 1032, 1033 and 1034 Connections……………………………………………..7 Modem to DSX-1022, 1021 and 1020 via MCI………………………………………………………...8 Telephone Line Connections……………………………………………………………………………8 Initial Modem Communications Procedure for Dial-up Location………………………………………9 Modem Compatibility………………………………………………………………………………….11 Existing Modems …..………………………………………………………………………………….11 Modem Initialization Strings …..……………………………………………………………………...12 Changing the Modem Initialization String for the PC…………………………………………………13 Modem Speaker Volume…...………………………………………………………………………….13 Resetting the Modem…………………………………………………………………………………..13 Default Baud Rates…………………………………………………………………………………….13