Final Report: Maximizing Use of Existing Data to Strengthen Program
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Food Insecurity and Undernutrition in Nepal
SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics Acknowledgements The completion of both this and the earlier feasibility report follows extensive consultation with the National Planning Commission, Central Bureau of Statistics (CBS), World Food Programme (WFP), UNICEF, World Bank, and New ERA, together with members of the Statistics and Evidence for Policy, Planning and Results (SEPPR) working group from the International Development Partners Group (IDPG) and made up of people from Asian Development Bank (ADB), Department for International Development (DFID), United Nations Development Programme (UNDP), UNICEF and United States Agency for International Development (USAID), WFP, and the World Bank. WFP, UNICEF and the World Bank commissioned this research. The statistical analysis has been undertaken by Professor Stephen Haslett, Systemetrics Research Associates and Institute of Fundamental Sciences, Massey University, New Zealand and Associate Prof Geoffrey Jones, Dr. Maris Isidro and Alison Sefton of the Institute of Fundamental Sciences - Statistics, Massey University, New Zealand. We gratefully acknowledge the considerable assistance provided at all stages by the Central Bureau of Statistics. Special thanks to Bikash Bista, Rudra Suwal, Dilli Raj Joshi, Devendra Karanjit, Bed Dhakal, Lok Khatri and Pushpa Raj Paudel. See Appendix E for the full list of people consulted. First published: December 2014 Design and processed by: Print Communication, 4241355 ISBN: 978-9937-3000-976 Suggested citation: Haslett, S., Jones, G., Isidro, M., and Sefton, A. (2014) Small Area Estimation of Food Insecurity and Undernutrition in Nepal, Central Bureau of Statistics, National Planning Commissions Secretariat, World Food Programme, UNICEF and World Bank, Kathmandu, Nepal, December 2014. -
Nepal's 9 Minimum Characteristics of a Disaster Resilient Community
Flagship 4 Handbook Nepal’s 9 Minimum Characteristics of a Disaster Resilient Community Published July 2013 Flagship 4: Integrated Community Based Disaster Risk Reduction/Management Flagship 4 is led by Government of Nepal’s Ministry of Federal Affairs and Local Development in partnership with the International Federation of Red Cross and Red Crescent Societies Flagship 4 is part of the Nepal Risk Reduction Consortium. An electronic version of this handbook can be downloaded from www.flagship4.nrrc.org.np The handbook is available in both English and Nepali Copies of the handbook and other documents can be obtained from IFRC’s Flagship 4 coordinator i Nepal’s 9 Minimum Characteristics Nepal’s 9 Minimum Characteristics of a Disaster Resilient Community of a Disaster Resilient Community About This Handbook Glossary of Terms Community Based Disaster Risk Reduction / Management Since the inception of the 9 minimum Handbook contents CBDRR/M characteristics of a disaster resilient community CDMC Community Disaster Management Committee in Nepal, there have been many questions Case studies by Government, implementing agencies, One attempt to provide guidance on DDC District Development Committee researchers, and community members on how operationalising the characteristics has DDMC District Disaster Management Committee to operationalise these characteristics. These been to collect a number of case studies questions have led to the formation of this from implementing agencies in Nepal. DDRC District Disaster Response Committee handbook which contains more information Each case study corresponds to a specific DEECC District Energy, Environment and Climate Change Division about each characteristic and examples of how characteristic and outlines how the they can be applied in interventions. -

Strengthening the Role of Civil Society and Women in Democracy And
HARIYO BAN PROGRAM Monitoring and Evaluation Plan 25 November 2011 – 25 August 2016 (Cooperative Agreement No: AID-367-A-11-00003) Submitted to: UNITED STATES AGENCY FOR INTERNATIONAL DEVELOPMENT NEPAL MISSION Maharajgunj, Kathmandu, Nepal Submitted by: WWF in partnership with CARE, FECOFUN and NTNC P.O. Box 7660, Baluwatar, Kathmandu, Nepal First approved on April 18, 2013 Updated and approved on January 5, 2015 Updated and approved on July 31, 2015 Updated and approved on August 31, 2015 Updated and approved on January 19, 2016 January 19, 2016 Ms. Judy Oglethorpe Chief of Party, Hariyo Ban Program WWF Nepal Baluwatar, Kathmandu Subject: Approval for revised M&E Plan for the Hariyo Ban Program Reference: Cooperative Agreement # 367-A-11-00003 Dear Judy, This letter is in response to the updated Monitoring and Evaluation Plan (M&E Plan) for the Hariyo Program that you submitted to me on January 14, 2016. I would like to thank WWF and all consortium partners (CARE, NTNC, and FECOFUN) for submitting the updated M&E Plan. The revised M&E Plan is consistent with the approved Annual Work Plan and the Program Description of the Cooperative Agreement (CA). This updated M&E has added/revised/updated targets to systematically align additional earthquake recovery funding added into the award through 8th modification of Hariyo Ban award to WWF to address very unexpected and burning issues, primarily in four Hariyo Ban program districts (Gorkha, Dhading, Rasuwa and Nuwakot) and partly in other districts, due to recent earthquake and associated climatic/environmental challenges. This updated M&E Plan, including its added/revised/updated indicators and targets, will have very good programmatic meaning for the program’s overall performance monitoring process in the future. -
Annual Report Submitted to USAID So the Details of Those Activities Are Not Reported Here
From Combatants to Peacemakers Program Project Final Report October, 2015 to March 31, 2017 Award No: AID-367-F-15-00002 Under USAID/DCHA/CMM APS-OAA-14-000003 Submitted to: United States Agency for International Development (USAID) Democracy and Governance Office Maharajgunj, Kathmandu, Nepal Tel: +977-01-42340000 Submitted by: Forum for Protection of Public Interest (Pro Public) Gautambuddha Marg, Anamnagar P.O.Box: 14307 Telephone: +977-01-4268681, 4265023 Fax: +977-01-4268022 1 Disclaimer: All these activities were made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of Pro Public and do not necessarily reflect the views of USAID or the United States Government. 2 Abbreviations BC Brahmin Chhetri CBO Community Based Organization CDO Chief District Officer CPN Communist Party of Nepal CSO Civil Society Organization DDC District Development Committee DF Dialogue facilitation ECs Ex-Combatants FGD Focus Group Discussion GESI Gender and Social Inclusion GIZ Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) GmbH KII Key Informant Interview LPC Local Peace Committee NC Nepali Congress NPTF Nepal Peace Trust Fund OCA Organizational Capacity Assessment OPI Organizational Performance Index PLA People Liberation Army Pro Public Forum for the Protection of Public Interest SDG Social Dialogue Group STPP Strengthening the Peace Process UCPN United Communist Party of Nepal UML United Marxist Leninist UNDP United Nations Development Program USAID United States Agency for International Development VDC Village Development Committee WCF Ward Citizen Forum 3 Acknowledgement This project completion report covers the overall implementation of the USAID-funded Combatants to Peacemakers (C2P) project (October 2015 to March 2017). -
STRIDE Service Coverage Assessment USAID, Nepal
STRIDE Service Coverage Assessment USAID, Nepal Order number: AID-367-O-16-00004 March 12, 2017 Anders Eklund Worldwide Rehabilitation Ltd. EXECUTIVE SUMMARY Nepal, like other countries in the region, has a substantial number of people who need physical rehabilitation. The 10-year civil conflict and the earthquake in April 2015 contributed to increasing that need. The Strengthening Rehabilitation in District Environs (STRIDE) program seeks to ensure that sustainable, accessible and quality physical rehabilitation services and community-based follow-up are provided for people with physical disabilities. The program is funded by the United States Agency for International Development (USAID) and implemented by Handicap International (HI) with sub-awards to five physical rehabilitation centers (PRCs) in four of the country's five regions. It was launched in January 2010 and is now in its second three-year extension (ending in January 2019). STRIDE plays an important role in the Nepali rehabilitation sector. To date, STRIDE PRCs have successfully provided physical rehabilitation services to more than 40,000 persons, including the delivery of more than 7200 prostheses and orthoses, 1200 wheelchairs and 4300 mobility aids. Services are normally center-based, but are also provided through outreach rehabilitation camps and field visits (so far reaching 52 of Nepal's 75 districts), with community disability workers (CDWs) conducting follow-up in the field. The main question that the present service coverage assessment sets out to answer is to what degree the physical rehabilitation services in Nepal, and in particular those of the five STRIDE PRCs, are able to meet the country's rehabilitation needs. -

Hariyo Ban Program Ii Threats and Vulnerabilities
HARIYO BAN PROGRAM II (2016-2021) THREATS AND VULNERABILITIES ASSESSMENT OF PARKS AND CORRIDORS OF TERAI ARC LANDSCAPE Prepared by: WWF in partnership with CARE, FECOFUN and NTNC P.O. Box 7660 Kathmandu, Nepal 21 April 2017 © WWF 2017 All rights reserved Any reproduction of this publication in full or in part must mention the title and credit WWF. Published by WWF Nepal PO Box: 7660 Baluwatar, Kathmandu, Nepal T: +977 1 4434820, F: +977 1 4438458 [email protected] , www.wwfnepal.org/hariyobanprogram Disclaimer This Threats and Vulnerabilities Assessment of Parks and Corridors in Terai Arc Landscape is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government. Contents INTRODUCTION ........................................................................................................................................................5 METHODOLOGY ........................................................................................................................................................6 Chitwan National Park and Buffer Zone ...................................................................................................................7 Threat Ratings of Chitwan National Park and Buffer Zone...................................................................................8 Barandabhar Corridor ........................................................................................................................................... -

Hariyo Ban Program
HARIYO BAN PROGRAM Semiannual Performance Report July 2019 – December 2019 (Cooperative Agreement No: AID-367-A-16-00008) Submitted to: THE UNITED STATES AGENCY FOR INTERNATIONAL DEVELOPMENT NEPAL MISSION Maharajgunj, Kathmandu, Nepal Submitted by: WWF in partnership with CARE, FECOFUN and NTNC P.O. Box 7660, Kathmandu, Nepal Submitted on: 01 February 2020 Table of Contents EXECUTIVE SUMMARY..................................................................................................................viii 1. INTRODUCTION ..................................................................................................................... 1 1.1. Goal and Objectives ........................................................................................................... 1 1.2. Overview of Beneficiaries and Stakeholders ..................................................................... 1 1.3. Working Areas ................................................................................................................... 2 2. SEMI-ANNUAL PERFORMANCE .......................................................................................... 4 2.1. Biodiversity Conservation .................................................................................................. 4 2.2. Climate Change Adaptation ............................................................................................. 20 2.3. Gender Equality and Social Inclusion ............................................................................. 29 2.4. Governance -
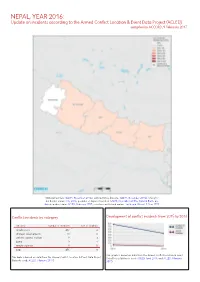
NEPAL, YEAR 2016: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 9 February 2017
NEPAL, YEAR 2016: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 9 February 2017 National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; China/In- dia border status: CIA, 2006; geodata of disputed borders: GADM, November 2015a; Natural Earth, un- dated; incident data: ACLED, February 2017; coastlines and inland waters: Smith and Wessel, 1 May 2015 Conflict incidents by category Development of conflict incidents from 2015 to 2016 category number of incidents sum of fatalities riots/protests 432 4 strategic developments 11 0 violence against civilians 9 3 battle 3 1 remote violence 1 0 total 456 8 This graph is based on data from the Armed Conflict Location & Event This table is based on data from the Armed Conflict Location & Event Data Project Data Project (datasets used: ACLED, April 2016, and ACLED, February (datasets used: ACLED, February 2017). 2017). NEPAL, YEAR 2016: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 9 FEBRUARY 2017 LOCALIZATION OF CONFLICT INCIDENTS Note: The following list is an overview of the incident data included in the ACLED dataset. More details are available in the actual dataset (date, location data, event type, involved actors, information sources, etc.). In the following list, the names of event locations are taken from ACLED, while the administrative region names are taken from GADM data which serves as the basis for the map above. In Central, 207 incidents killing 1 person were reported. The following locations were affected: Bhaktapur, Bharatpur, Bidur, Birganj, Bishrampur, Brahmapuri, Chandranigahapur, Chandrapur, Charikot, Chautara, Dharhari, Dhulikhel, Dhunche, Gamhariya Birta, Gaur, Gokarneshwar, Jaleswar, Janakpur, Kalaiya, Kamalamai, Kathmandu, Kirtipur, Kritipur, Madi, Mahottari, Malangwa, Patan, Rasuwa Ghadhi, Sanepa. -

Saath-Saath Project
Saath-Saath Project Saath-Saath Project THIRD ANNUAL REPORT August 2013 – July 2014 September 2014 0 Submitted by Saath-Saath Project Gopal Bhawan, Anamika Galli Baluwatar – 4, Kathmandu Nepal T: +977-1-4437173 F: +977-1-4417475 E: [email protected] FHI 360 Nepal USAID Cooperative Agreement # AID-367-A-11-00005 USAID/Nepal Country Assistance Objective Intermediate Result 1 & 4 1 Table of Contents List of Acronyms .................................................................................................................................................i Executive Summary ............................................................................................................................................ 1 I. Introduction ........................................................................................................................................... 4 II. Program Management ........................................................................................................................... 6 III. Technical Program Elements (Program by Outputs) .............................................................................. 6 Outcome 1: Decreased HIV prevalence among selected MARPs ...................................................................... 6 Outcome 2: Increased use of Family Planning (FP) services among MARPs ................................................... 9 Outcome 3: Increased GON capacity to plan, commission and use SI ............................................................ 14 Outcome -

Facility Based Assessment for Reproductive Health Commodities and Services
Facility Based Assessment for Reproductive Health Commodities and Services FINAL REPORT United Nations Population Fund (UNFPA) Shanta Bhawan Road, Jhamsikhel Lalitpur, Nepal Submitted By Nepal Development Research Institute Shree Durbar Tole, Pulchowk, Lalitpur, Nepal Submission date: 16th March 2015 i This report is a product of research on "Facility Based Assessment for Reproductive Health Commodities and Services “carried out by Nepal Development Research Institute with the financial support of United Nations Population Fund (UNFPA) from October 2014 to January 2015 Study Team • Dr. Basu Dev Pandey, Team Leader • Prof. Naveen Shrestha, Senior Consultant Expert • Dr. Jaya Kumar Gurung, Project Coordinator • Dr. Rabita Mulmi, Field Survey Coordinator • Ms. Saruna Ghimire, Consultant Expert • Ms. Sona Shakya , Senior Research Associate Report By: Nepal Development Research Institute Shree Durbar Tole, Pulchowk, Lalitpur www.ndri.org.np ii Acknowledgement It is a great pleasure for Nepal Development Research Institute (NDRI) to accomplish this research in collaboration with concern departments of Government of Nepal and UNFPA/Nepal. We thank UNFPA for entrusting NDRI and making congenial environment for this research work. It's immense pleasure to acknowledge the representatives of Nepal Government's agencies particularly Dr. Senendra Raj Upreti, Director General , Department of Health services, Dr. Bhim Singh Tinkari, Director of Logistic Management Division (LMD), Dr. Pushpa Chaudhari, Director, Family Health Division (FHD), Bhogendra Raj Dotel, Senior Public Health Administrator, Mr. Gyan Bahadur BC, Planning Officer (LMD), Krishna Ghimire, Joint Secretary (LMD), Upendra Dhungana (LMD) for their invaluable cooperation into various ways; valuable inputs in the inception phase of project, important contribution in training to field researchers, arranging the district and regional level health facilities for their cooperation, and providing suggestions in the draft report. -

Assessment of Poaching and Illegal Wildlife Trafficking in Banke- Kamdi Complex
Assessment of Poaching and Illegal Wildlife Trafficking in Banke- Kamdi Complex Submitted to: Hariyo Ban Program Baluwatar, Kathmandu, Nepal Submitted by: People’s Help Group (PHG) Kathmandu, Nepal July, 2017 © WWF Nepal 2017 All rights reserved Disclaimer: This report is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents of this report are the responsibility of People’s Help Group (PHG) and do not necessarily reflect the views of USAID or the United States Government. Executive Summary Wildlife crime is a serious issue in conservation particularly of the threatened species of wild flora and fauna globally. Several endangered species such as Asian big cats, elephants and rhinoceros are at the verge of extinction if the current trend of wildlife crime is not retarded. The illegal wildlife trade is among the leading causes for rapid wildlife species decline worldwide (McMurray, 2008). Similarly, Nepal cannot be exception to this situation; the country has been known as transit for illegal wildlife trade and a source for some of the illegally traded species such as rhino horns, tiger and leopard pelts and pangolin scales. Despite various efforts to control wildlife crime, such crime still exists sporadically and in low volume in the country. The Banke-Kamdi complex is located in the (Mid-western region, State No.6) and covers part of Banke, Dang and Salyan districts. This Complex comprises of Banke National Park (BaNP), its Buffer Zone and Kamdi forest corridor. At present, Kamdi Corridor is under the Banke District Forest and is one of the most important biological corridors of Tarai Arc Landscape. -
BIODIVERSITY, PEOPLE and CLIMATE CHANGE Final Technical Report of the Hariyo Ban Program, First Phase
BIODIVERSITY, PEOPLE AND CLIMATE CHANGE Final Technical Report of the Hariyo Ban Program, First Phase Volume Two Detailed Annexes HARIYO BAN PROGRAM This final technical report for Hariyo Ban Program Phase One is submitted to the United States Agency for International Development Nepal Mission by World Wildlife Fund Nepal in partnership with CARE, the Federation of Community Forest Users Nepal and the National Trust for Nature Conservation, under Cooperative Agreement Number AID-367-A-11-00003. © WWF Nepal 2017 All rights reserved Citation Please cite this report as: WWF Nepal. 2017. Biodiversity, People and Climate Change: Final Technical Report of the Hariyo Ban Program, First Phase. WWF Nepal, Hariyo Ban Program, Kathmandu, Nepal. Cover photo credit © Karine Aigner/WWF-US Disclaimer: This report is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of WWF and do not necessarily reflect the views of USAID or the United States Government. 7 April, 2017 Table of Contents ANNEX 5: HARIYO BAN PROGRAM WORKING AREAS ......................................................................... 1 ANNEX 6: COMMUNITY BASED ANTI-POACHING UNITS FORMED/REFORMED ................................. 4 ANNEX 7: SUPPORT FOR INTEGRATED SUB-WATERSHED MANAGEMENT PLANS ........................... 11 ANNEX 8: CHARACTERISTICS OF PAYMENTS FOR ECOSYSTEM SERVICES SCHEMES PILOTED ......... 12 ANNEX 9: COMMUNITY ADAPTATION PLANS OF ACTION PREPARED .............................................