Vet FHT 2007 Oct 2008 Mar.Pdf (8.042Mb)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Prepubertal Gonadectomy in Male Cats: a Retrospective Internet-Based Survey on the Safety of Castration at a Young Age
ESTONIAN UNIVERSITY OF LIFE SCIENCES Institute of Veterinary Medicine and Animal Sciences Hedvig Liblikas PREPUBERTAL GONADECTOMY IN MALE CATS: A RETROSPECTIVE INTERNET-BASED SURVEY ON THE SAFETY OF CASTRATION AT A YOUNG AGE PREPUBERTAALNE GONADEKTOOMIA ISASTEL KASSIDEL: RETROSPEKTIIVNE INTERNETIKÜSITLUSEL PÕHINEV NOORTE KASSIDE KASTREERIMISE OHUTUSE UURING Graduation Thesis in Veterinary Medicine The Curriculum of Veterinary Medicine Supervisors: Tiia Ariko, MSc Kaisa Savolainen, MSc Tartu 2020 ABSTRACT Estonian University of Life Sciences Abstract of Final Thesis Fr. R. Kreutzwaldi 1, Tartu 51006 Author: Hedvig Liblikas Specialty: Veterinary Medicine Title: Prepubertal gonadectomy in male cats: a retrospective internet-based survey on the safety of castration at a young age Pages: 49 Figures: 0 Tables: 6 Appendixes: 2 Department / Chair: Chair of Veterinary Clinical Medicine Field of research and (CERC S) code: 3. Health, 3.2. Veterinary Medicine B750 Veterinary medicine, surgery, physiology, pathology, clinical studies Supervisors: Tiia Ariko, Kaisa Savolainen Place and date: Tartu 2020 Prepubertal gonadectomy (PPG) of kittens is proven to be a suitable method for feral cat population control, removal of unwanted sexual behaviour like spraying and aggression and for avoidance of unwanted litters. There are several concerns on the possible negative effects on PPG including anaesthesia, surgery and complications. The aim of this study was to evaluate the safety of PPG. Microsoft excel was used for statistical analysis. The information about 6646 purebred kittens who had gone through PPG before 27 weeks of age was obtained from the online retrospective survey. Database included cats from the different breeds and –age groups when the surgery was performed, collected in 2019. -
The Cat Show
THE BREEDS Pixiebob Longhair Pixiebob Shorthair ACFA recognizes 57 breeds. They are: Persian Peterbald Abyssinian RagaMuffin American Bobtail Longhair Ragdoll THE American Bobtail Shorthair Russian Blue American Curl Longhair Russian Shorthair American Curl Shorthair Scottish Fold American Shorthair Selkirk Rex Longhair American Wirehair Selkirk Rex Shorthair Australian Mist Siamese Balinese Siberian CAT Bengal Singapura Birman Snowshoe Bombay Somali British Shorthair Sphynx Burmese Tonkinese Chantilly Turkish Angora SHOW Chartreux Turkish Van Cornish Rex Cymric Devon Rex FOR INFORMATION Egyptian Mau European Burmese on registering your cat, entering your Exotic Shorthair Havana Brown cat in an ACFA show, finding a Highland Fold breeder of a specific breed or anything Himalayan else concerning cats or cat shows Japanese Bobtail Longhair contact: Japanese Bobtail Shorthair Korat La Perm American Cat Fanciers Association Longhair Exotic P.O. Box 1949 Maine Coon Cat Nixa, MO 65714-1949 Manx PH: 417-725-1530 Nebelung email: [email protected] Norwegian Forest Cat Ocicat Web Page: www.acfacat.com Oriental Longhair Oriental Shorthair Welcome to our cat show. We hope you THE JUDGING AWARDS AND RIBBONS will enjoy looking at all the cats we have on display. We have pedigreed cats and household Each day there will be four or more rings Each cat competes in its class against other cats pet cats being exhibited. These cats are judged of the same sex, color and breed. The cat by professional judges licensed by the running concurrently. Each judge acts independently of the others and every cat selected as best in the class receives a blue American Cat Fanciers Association. -

Reds, Creams and Inbetweens Dr Kerry Fowler Msc Phd Grad Dip Ed Published in NSW CFA Catching up 5(3/4):5-6(2003)
Reds, Creams and Inbetweens Dr Kerry Fowler MSc PhD Grad Dip Ed Published in NSW CFA Catching Up 5(3/4):5-6(2003) Background Current registration systems in most Australian cat councils work on the concept that two solid cats cannot produce a tabby kitten. In the main this policy is absolutely correct however in the case of the orange or ‘O’ gene cats ie creams, reds and the less vibrant reds known as ‘gingers’ and ‘marmalades’, sticking to this hard and fast rule often results in no end of controversy and confusion. Breeders are obliged to register red or cream tabby marked kittens from solid parents as red or cream selfs and in turn judges are required to assess them as such despite some of these red or cream kittens and cats having an abundance of clear tabby markings. Being a sex-linked gene, the ‘O’ gene coat colour issues extend to tortoiseshells, blue-creams and tricolours. This article identifies some of the misunderstanding surrounding breeding and judging ‘O’ gene cats including cameos and apricots, and draws on current genetic knowledge, registration policies and show standards from other councils to help resolve some of the re-occurring questions. Genetic principles In order to help put some of the debate and perplexity aside it is worth keeping in mind that there are four basic genetic rules that help us to understand the appearance of red or cream tabbies and solids. First, the tabby pattern gene is present in all cats including solid or self cats. Second, the tabby pattern is only revealed when the dominant agouti gene product or protein is present. -

Ing Back-To-Back with the SOUTH WEST BRITISH SHORTHAIR CAT CLUB
THE SOUTH WESTERN COUNTIES CAT CLUB Schedule of the 66th Championship Show (Held under licence and rules of the G.C.C.F) Running Back-to-Back with THE SOUTH WEST BRITISH SHORTHAIR CAT CLUB 2 – in – 1 ALL Section 3 and HOUSEHOLD PET cats will have the opportunity to obtain 2 certificates at 1 venue by entering both shows WELLSPRINGS LEISURE CENTRE CHEDDON ROAD, TAUNTON. TA2 7QP on Saturday 28th September 2019 JOINT SHOW MANAGER JOINT SHOW MANAGER Miss Lesley Tricker Mrs Susan Newman 131 King Arthur’s Road, Beacon Heath, Totara Lodge, Whitehill Road, Exeter, EX4 9DS Highweek, Newton Abbot, TQ12 1QD Email: [email protected] [email protected] Tel: 01392 677855 Tel: 01626 334242 ENTRIES CLOSE: 3RD SEPTEMBER 2019 ALL ENTRIES MUST BE RECEIVED BY THIS DATE NO ENTRIES CAN BE WITHDRAWN AFTER THIS DATE UPGRADE CLASSES UNTIL 5.00 P.M. ON 8TH SEPTEMBER 2019 SOUTH WESTERN COUNTIES CAT CLUB Affiliated To The GCCF Founded 1931 PRESIDENT: Mrs D Harper VICE PRESIDENTS: Mr John Burley & Mrs S Newman CHAIRPERSON: Miss L Tricker HON. TREASURER: Mrs R Fisher HON. SECRETARY: Mrs M Hutchings COMMITTEE: Miss A Evans,Ms M Haas, Miss S Moyle, Mr R O’Halloran, Mrs S O’Halloran, Miss C Phillips PEDIGREE JUDGES Mrs S Bower, Mrs J Bradley, Mrs M Buckeridge, Mr R Davies, Mrs S Dalton-Hobbs, Mrs E Fryer, Mrs K Kempsell, Miss C Lewis, Mr G Martin, Mrs L Martin, Mrs J Pounds, Mrs S Rainbow-Ockwell, Mrs S Rose, Mrs B Shingleton, Mrs S Tokens, Miss C White, Mrs J Williams ______________________________________________________________________________ BEST -

THE INTERNATIONAL CAT ASSOCIATION, INC. 2014 Annual Board Meeting August 27 – 29, 2014: Worcester, Massachusetts
THE INTERNATIONAL CAT ASSOCIATION, INC. 2014 Annual Board Meeting August 27 – 29, 2014: Worcester, Massachusetts The following Board members were present: President, Vickie Fisher Northwest Director, Ellen Crockett Vice President, Bobbie Tullo South Central Director, Wendy Klamm Great Lakes Director, Mike Vasquez Southern Europe Director, Damien Bourreau Mid Pacific Director, Jay Bangle Southeast Director, Laurie Patton Northeast Director, Francine Hicks Southwest Director, Alexandra Chisholm Northern Europe Director, Ralph Stadter Western Europe Director, Phil Cornwell Mid Atlantic Director, Susan Adler joined by phone. Motoko Oizumi (Asia Director) and Luiz Paulo Faccioli (South America Director) were absent. Lesley Hart from the Executive Office, Marylou Anderson (Judging Administrator), and Roeann Fulkerson (Marketing Director) were also present. ** Meeting started on Wednesday, August 27,, 2014 at 9am** The President opened up discussion on future meetings, should they be electronic or face to face, specifically the upcoming January meeting. 1: Motion made by Patton and seconded by Vasquez to approve the January 23-25, 2015 meeting in Harlingen. Motion carried. Adler and Bourreau abstained. Bangle, Cornwell, Klamm, and Stadter opposed. The President asked if there were any changes to the minutes from the last meeting. 2: Motion made by Adler for unanimous consent to remove the language regarding "Japanese court has already ruled upon the constitutional issues". Without objection. The board discussed the current state of the Minskin breed. 3: Motion made by Hicks for unanimous consent to appoint Rachel Gouvia to working breed chair for Minskin. Without objection. Discussion on Amend standing rule 106.4 presented by Vasquez. 4: Motion made by Vasquez and seconded by Bangle to amend standing rule 106.4 Rules/Genetics committee shall have a chairperson, members as needed and a board member who works with the committee as a liaison director. -

Cover Spring 2018
The Scratching Post SABCCI Newsletter - Spring 2018 www.sabcci.com The Scratching Post Contents - Spring 2018 Page Editorial, Competition & Oldest Cat Fossils Found 3 The Pedigree - The Australian Mist 4 Working Cats 4 Cat Aggression - Part 2 5 Buttons & Rescue Cats For The Workplace In Japan 6 The Quiz & Cat Fun 7 The Dublin Championship Cat Show 2017 8/9 Where Did It Come From 9 The Catwalk 10/11 Cats In The News 12 Working Cats Program 13 Does Colour Influence The Personality Of A Cat ? 13/14 Health - Ringworm 14 Kits Korner 15 The Final Miaow & New York Cat Film Festival 16 www.sabcci.com SABCCI Committee Ronnie Brooks, Dionne Dixon, Sonia Early, Hugh Gibney, Gloria Hehir, Aedamair Kiely Mary O’Donaghue, Karen Sluiters, Jim Stephens, Lorna Taylor, Aimee Weldon Membership Secretary - Betty Dobbs Positions Wanted - As Cats Might Write ∗ Black and white cat seeks neck to warm. Suitable replacement for hot water bottle, does not cool down during night. ∗ Gourmet seeks position as chief food taster. Excellent taste in venison, salmon and other fine meats. Connoisseur of cream. Will indicate quality of all foods tasted with loud purring. ∗ Mother’s help seeks post, will undertake dish-licking and general purring. Willing to supervise well behaved children. No tail- pullers need apply. ∗ Retired supervisor, skilled in entertaining children seeks position as nanny/childminder. Has experience of working in large unruly household. Very tolerant, has trained large family now living overseas. 2 Editorial Welcome to our Spring 2018 issue of The -

FSCC Kitten & Neuter Show – 17 March 2019
THE FOREIGN SHORTHAIR CAT CLUB OF Sth AUST INC 4th KITTEN & NEUTER ST PATRICK’S DAY CAT SHOW Conducted under the Rules and Regulations of the Governing Council of the Cat Fancy of SA Inc FULLARTON PARK CENTRE 17th March 2019 St Patrick’s Day PROUDLY SPONSORED BY FINAL VERSION 23.03.19 2 FSCC KITTEN & NEUTER SHOW –17TH MARCH 2019 Thank you to our sponsors FSCC KITTEN & NEUTER SHOW –17TH MARCH 2019 3 THE FOREIGN SHORTHAIR CAT CLUB OF Sth AUST INC 4th KITTEN & NEUTER ST PATRICK’S DAY CAT SHOW Conducted under the Rules and Regulations of the Governing Council of the Cat Fancy of SA Inc 17TH MARCH 2019 FULLARTON PARK CENTRE 411 FULLARTON ROAD FULLARTON Judging Panel RING 1 RING 2 GROUP 1 CAROL HOSKINS (GCCFV) CLAIRE EDWARDS (GCCFSA) GROUP2 CAROL HOSKINS (GCCFV) CLAIRE EDWARDS (GCCFSA) GROUP 3 SHARA MCKAY ( CATS NSW) ELIZABETH ANDRESEN (GCCFSA) GROUP 4 SHARA MCKAY (CATS NSW) ELIZABETH ANDRESEN (GCCFSA) GROUP 5 CAROL HOSKINS (FCCV) TRIXIE PETTMAN SOUTH (GCCFSA) GROUP 6 CAROL HOSKINS (GCCFV) TRIXIE PETTMAN SOUTH (GCCFSA) RING 3 GROUP 1 – 6 KITTENS ONLY, HAZEL ROSSITER (CATS NSW) 4 FSCC KITTEN & NEUTER SHOW –17TH MARCH 2019 Thank you to our sponsors Supporting cat health Australian Natural Health ™ cat food was developed with veterinarians and animal nutritionists and is a complete and wholesome dry food for your companion’s balanced nutrition and every day feeding. Using only high quality ingredients, this high protein, grain free dry food promotes healthy digestion and is packed full of wholesome ingredients including a high concentration of quality animal protein to help with lean muscle maintenance. -

Collection of Baseline Population Data on Pet Cats Living in Sydney
Postprint This is an Accepted Manuscript of an article published in [Journal of Feline Medicine and Surgery] in June 2009. Available online at http://jfm.sagepub.com/content/11/6/449.short (paywalled) Please cite as: Toribio, J., Norris, J. M., White, J. D., Dhand, N. K., Hamilton, S. A., & Malik, R. (2009). Demographics and husbandry of pet cats living in Sydney, Australia: results of cross-sectional survey of pet ownership. Journal of Feline Medicine and Surgery, 11(6), 449-461. Demographics and husbandry of pet cats living in Sydney, Australia: results of cross-sectional survey of pet ownership J-A.L.M.L. TORIBIO1, J.M. NORRIS1, J.D. WHITE1, N.K. DHAND1, S.A. HAMILTON1, R. MALIK1,2 1Faculty of Veterinary Science, The University of Sydney, NSW Australia 2006 2Post Graduate Foundation in Veterinary Science, Conference Centre, Building B22, The University of Sydney Australia 2006 Our aim was to collect baseline data on the age, gender, breed, reproductive status and husbandry (housing, diet, vaccination, veterinary attention) of pet cats living in Sydney. Accordingly, a cross-sectional survey of 2768 households was conducted using a postal questionnaire. The 2006 Sydney residential phone book was used as the sampling frame. Non- responders were re-mailed the questionnaire on two further occasions, two and four weeks after the first postings. Completed questionnaires were received from 884 households. No pets were kept by 387 (43.8%) respondents. Dogs and cats were owned by 295 (33.4%) and 198 (22.5%) of households, respectively, with 7.8% of households having both cat(s) and dog(s). -
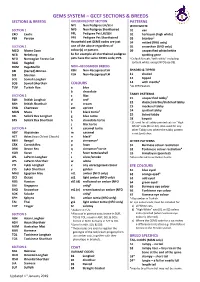
Gems System – Gccf Sections & Breeds
GEMS SYSTEM – GCCF SECTIONS & BREEDS SECTIONS & BREEDS HOUSEHOLD PET SECTION PATTERNS NPL Non Pedigree LH/SLH WITH WHITE SECTION 1 NPS Non Pedigree Shorthaired 01 van EXO Exotic PPL Pedigree Pet LH/SLH 02 harlequin (high white) PER Persian PPS Pedigree Pet Shorthaired 03 bicolour5 Household pet GEMS codes are just 04 mitted (RAG only) SECTION 2 one of the above regardless of 05 snowshoe (SNO only) MCO Maine Coon colour(s) or pattern. 09 unspecified white/white NEB Nebelung So for example all shorthaired pedigree spotting gene NFO Norwegian Forest Cat pets have the same GEMS code; PPS. 5 Default for cats “with white” including RAG Ragdoll tortie & white, except NFO (use 09). RGM RagaMuffin NON –RECOGNISED BREEDS SBI (Sacred) Birman XSH Non-Recognised SH SHADED & TIPPED SIB Siberian XLH Non-Recognised LH 11 shaded SOL Somali Longhair 12 tipped 6 SOS Somali Shorthair COLOURS 14 with mantle 6 TUV Turkish Van a blue As PER Pewters b chocolate TABBY PATTERNS SECTION 3 c lilac 7 BLH British Longhair d red1 21 unspecified tabby BSH British Shorthair e cream 22 classic/marble/blotched tabby CHA Chartreux em apricot 23 mackerel tabby MAN Manx f black tortie2 24 spotted tabby SRL Selkirk Rex Longhair g blue tortie 25 ticked tabby SRS Selkirk Rex Shorthair h chocolate tortie 28 karpati 7 21 used for all tabby pointed cats or “High j lilac tortie White” cats (01 or 02). Also used for any SECTION 4 k caramel tortie other Tabby cats where the tabby pattern ABY Abyssinian m caramel is not (yet) clear. -

A Synopsis of Feline Infectious Peritonitis Virus Infection
A synopsis of feline infectious peritonitis virus infection Niels C Pedersen, D.V.M., Ph.D., Center for Companion Animal Health, Room 213, CCAH Bldg., School of Veterinary Medicine, University of California, Davis, CA, 95616, USA. Tel:+1-530-752-7402, Fax:+1-752-7701; E-mail: [email protected] Introduction This synopsis is taken from a much larger and more scientifically comprehensive review of FIP literature from the period 1963 through 2008. Although more technical than the Q&A format review also provided on the SOCKFIP website, it should prove helpful to those people with the desire to obtain more in depth knowledge of this disease. It is also hoped that the inclusion of references will demonstrate the amount of actual peer-reviewed research that has been done on the disease and tol make readers aware of the actual state of FIP prevention, diagnosis and treatment. Readers will be also less apt to rely on the mass of anectdotal and frequently incorrect information on FIP that floods the web. Historical Feline infectious peritonitis (FIP) was first described as an “important disorder of cats” by Holzworth (1963) at the Angell Memorial Animal Hospital, Boston and a clinico-pathologic conference on this disorder from this same institution was published the following year (Feldman and Jortner, 1964). The disease was thought to be infectious but no specific etiologic agent was identified at the time. Wolfe and Griesemer (1966) were the first to propose that FIP was caused by a virus. Zook et al (1968) observed virus particles in the tissues of experimentally infected cats, but were unable to characterize the agent. -

National Breed Standards
NATIONAL BREED STANDARDS © ANCATS 2017 ANCATS National Breed Standards 2017 1 INDEX ........................................................................................................................................................................................................................................................................... 2 GLOSSARY ................................................................................................................................................................................................................................................................. 5 PREFACE .................................................................................................................................................................................................................................................................. 10 The Condition of the Cat .................................................................................................................................................................................................................. 11 Judging Disqualification Faults ........................................................................................................................................................................................................ 12 General faults in all breeds precluding a Challenge or Best in Show ............................................................................................................................................. -

C:\Users\Lbowers\Desktop\2016 Annual Meeting\2016
THE INTERNATIONAL CAT ASSOCIATION, INC. 2016 Annual Board Meeting Town and Country Resort and Convention Center San Diego, California August 31 - September 2, 2016 (Open Session) August 31, 2016, Wednesday, 8:30AM ACTION PAGE Welcome and Call to Order 1. Roll Call Mays Verbal...............................- 2. President's Remarks Mays Verbal ...............................- Ethics Mays Verbal....................................- Consent Agenda 1. Minutes, Corrections/Additions EO Approve .............................- Motion for payment of Rebate to IN Region 2. Motion to pay expenses for EO Approve .............................- Judging Administrator Executive Session (See Executive Agenda) 2016 Annual Meeting, Page 1 September 1, 2016, Thursday, 8:30AM Governance 1. Future Meetings Update ..............................- Winter 2017 January 25-27-Portland, OR Crockett .............................- Spring 2017 May 19-21 -Harlingen, TX EO .................................- Annual 2017 August 30-September 1 Corpus Christi, TX, Klamm ..............................- Annual 2018 Birmington, AL August 29-31 Patton ...............................- Fiduciary/Business Reports 1. Year End Financial Review Fisher Receive .................. 6 2. Hotel and per diem rates BOD Approve ..................- 3. Marketing Report Fulkerson Receive ................. 14 4. Communications Coordinator Fulkerson Receive................. 28 5. Update on Ticketing System, Jones ................... to be furnished Phone System, IT Program Manager Proposals Board