Spontaneously Terminating Ventricular Fibrillation and Asystole Induced By
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Follow-Up of 134 Pediatric Patients with Wolff-Parkinson-White Pattern: Natural Outcome and Medical Treatment
ORIGINAL ARTICLE Follow-up of 134 Pediatric Patients with Wolff-Parkinson-White Pattern: Natural Outcome and Medical Treatment AMALIA N. STEFANI, GABRIELA R. DAL FABBRO, MARÍA J. BOSALEH, ROBERTH VÁSQUEZ, GUSTAVO A. COSTA, RICARDO SPERANZA, JORGE L. GENTILE, CLAUDIO DE ZULOAGAMTSAC Received: 01/03/2013 ABSTRACT Accepted: 01/03/2013 Address for reprints: Objective Amalia N. Stefani The aim of the study was to evaluate the outcome of a pediatric population with Almafuerte 1722 ventricular pre-excitation pattern, supraventricular tachycardia, atrial fibrillation, (1650) San Martín, cardiomyopathies, mortality and medical treatment. Pcia. de Buenos Aires e-mail: [email protected] Methods From 1976 to 2011, a descriptive observational study was conducted on patients with ventricular pre-excitation in the electrocardiogram. All patients underwent an echocardiogram, 101(75.3%) Holter monitoring, and 69 (51.5%) an ergometric test. Radiofrequency ablation was performed in selected patients. Data were expressed as mean and standard deviation. Results The study population consisted of 134 patients; 80 (59.7%) were male. Age at diag- nosis ranged from 2 days to 18 years (mean 6.5±5 years). Clinical follow-up lasted 1 month to 20 years (mean 3.6±3.9 years). Thirty five patients (26.1%) consulted for supraventricular tachycardia, 16 (11.9%) for ventricular pre-excitation, and the remaining 83 patients (61.9%) for other abnormalities. Seventy-six patients (56.7%) had left conduction pathway and 3 patients double conduction pathway. Sixteen pa- tients (11.9%) presented supraventricular tachycardia during follow-up. Overall, 51 patients (38%) had orthodromic tachycardia at 6.3±5.8 years, 10 patients during the neonatal period. -

Prolonged Asystole During Hypobaric Chamber Training
Olgu Sunumları Anadolu Kardiyol Derg 520 Case Reports 2012; 12: 517-24 contraction/ventricular tachycardia’s originating from mitral annulus contractions arising from the mitral annulus: a case with a pure annular are rarely reported (1). origin. Pacing Clin Electrophysiol 2009; 32: 680-2. [CrossRef] PVCs arising from the mitral annulus frequently originate from 5. Kimber SK, Downar E, Harris L, Langer G, Mickleborough LL, Masse S, et al. anterolateral, posteroseptal and posterior sites (2). It has been reported Mechanisms of spontaneous shift of surface electrocardiographic configuration that 2/3 of the PVCs arising from the mitral annulus originate from during ventricular tachycardia. J Am Coll Cardiol 1992; 15: 1397-404. [CrossRef] anterolateral site (2). Furthermore, small part of these arrhythmias origi- Address for Correspondence/Yaz›şma Adresi: Dr. Ömer Uz nates from the anteroseptal site of the mitral annulus. Ablation of this Gülhane Askeri Tıp Akademisi Haydarpasa, Kardiyoloji Kliniği, İstanbul-Türkiye site may be technically very challenging. Cases have been reported that Phone: +90 216 542 34 65 Fax: +90 216 348 78 80 successful catheter ablation of the premature ventricular contraction E-mail: [email protected] origin from the anteroseptal site of the mitral annulus can be performed Available Online Date/Çevrimiçi Yayın Tarihi: 22.06.2012 either by a transseptal or transaortic approach in literature (3, 4). ©Telif Hakk› 2012 AVES Yay›nc›l›k Ltd. Şti. - Makale metnine www.anakarder.com web Anterolateral site of the mitral annulus is in close proximity to anterior sayfas›ndan ulaş›labilir. of the right ventricle outflow tract, left ventricular epicardium near to ©Copyright 2012 by AVES Yay›nc›l›k Ltd. -

ICD-9-ICD-10 Codes for Cardiology
ICD-9-ICD-10 Codes for Cardiology ICD-9 Code ICD-10 Code(s) ICD-10 Descrption(s) Atrial Fibrillation and Flutter 427.31, 427.32 I48.0 Paroxysmal atrial fibrillation I48.1 Persistent atrial fibrillation I48.2 Chronic atrial fibrillation I48.3 Typical atrial flutter I48.4 Atypical atrial flutter I48.91* Unspecified atrial fibrillation I48.92* Unspecified atrial flutter Cardiac Arrhythmias (Other) 427.41, 427.42, 427.60, 427.61, 427.69, 427.81, 427.89, 427.9 I49.01 Ventricular fibrillation I49.02 Ventricular flutter I49.1 Atrial premature depolarization I49.2 Junctional premature depolarization I49.3 Ventricular premature depolarization I49.40 Unspecified premature depolarization I49.49 Other premature depolarization I49.5 Sick sinus syndrome I49.8 Other specified cardiac arrhythmias I49.9* Cardiac arrhythmia, unspecified Chest Pain 411.1, 413.1, 413.9, 786.50 to 786.59 range I20.0 Unstable angina I20.1 Angina pectoris with documented spasm I20.8 Other forms of angina pectoris I20.9 Angina pectoris, unspecified R07.1 Chest pain on breathing R07.2 Precordial pain R07.81 Pleurodynia R07.82 Intercostal pain R07.89 Other chest pain R07.9* Chest pain, unspecified Heart Failure 428.0, 428.1, 428.20 to 428.23 range, 428.30 to 428.33 range, 428.40 to 428.43 range, 428.9 I50.1 Left ventricular failure I50.20* Unspecified systolic (congestive) heart failure I50.21 Acute systolic (congestive) heart failure I50.22 Chronic systolic (congestive) heart failure I50.23 Acute on chronic systolic (congestive) heart failure I50.30* Unspecified diastolic (congestive) -

Ventricular Rhythms Originate Below the Branching Portion of The
Northwest Community Healthcare Paramedic Program VENTRICULAR DYSRHYTHMIAS Pacemakers Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol 3; pp. 96-109 SOPs: VT with pulse; Ventricular fibrillation/PVT; Asystole/PEA Drugs: Amiodarone, magnesium, epinephrine 1mg/10mL Procedure manual: Defibrillation; Mechanical Circulatory Support (MCS) using a Ventricular Assist Device KNOWLEDGE OBJECTIVES: Upon completion of the reading assignments, class and homework questions, reviewing the SOPs, and working with their small group, each participant will independently do the following with at least an 80% degree of accuracy and no critical errors: 1. Identify the intrinsic rates, morphology, conduction pathways, and common ECG features of ventricular beats/rhythms. 2. Identify on a 6-second strip the following: a) Idioventricular rhythm b) Accelerated idioventricular rhythm c) Ventricular tachycardia: monomorphic & polymorphic d) Ventricular escape beats e) Premature Ventricular Contractions (PVCs) f) Ventricular fibrillation g) Asystole h) Paced rhythms i) Intraventricular conduction defects (Bundle branch blocks) 3. Systematically evaluate each complex/rhythm for the following: a) Rate (atrial and ventricular) b) Rhythm: Regular/irregular - R-R Interval, P-P Interval c) Presence/absence/morphology of P waves d) Presence/absence/morphology of QRS complexes d) P-QRS relationships f) QRS duration 4. Correlate the cardiac rhythm with patient assessment findings to determine the emergency treatment for each rhythm according to NWC EMSS SOPs. 5. Discuss the action, prehospital indications, side effects, dose and contraindications of the following during VT a) Amiodarone b) Magnesium 6. Describe the indications, equipment needed, critical steps, and patient monitoring parameters for cardioversion and defibrillation. 7. Identify the management of a patient with an implanted defibrillator and/or pacemaker. -

Pub 100-04 Medicare Claims Processing Centers for Medicare & Medicaid Services (CMS) Transmittal 3054 Date: August 29, 2014 Change Request 8803
Department of Health & CMS Manual System Human Services (DHHS) Pub 100-04 Medicare Claims Processing Centers for Medicare & Medicaid Services (CMS) Transmittal 3054 Date: August 29, 2014 Change Request 8803 SUBJECT: Ventricular Assist Devices for Bridge-to-Transplant and Destination Therapy I. SUMMARY OF CHANGES: This Change Request (CR) is effective for claims with dates of service on and after October 30, 2013; contractors shall pay claims for Ventricular Assist Devices as destination therapy using the criteria in Pub. 100-03, part 1, section 20.9.1, and Pub. 100-04, Chapter 32, sec. 320. EFFECTIVE DATE: October 30, 2013 *Unless otherwise specified, the effective date is the date of service. IMPLEMENTATION DATE: September 30, 2014 Disclaimer for manual changes only: The revision date and transmittal number apply only to red italicized material. Any other material was previously published and remains unchanged. However, if this revision contains a table of contents, you will receive the new/revised information only, and not the entire table of contents. II. CHANGES IN MANUAL INSTRUCTIONS: (N/A if manual is not updated) R=REVISED, N=NEW, D=DELETED-Only One Per Row. R/N/D CHAPTER / SECTION / SUBSECTION / TITLE D 3/90.2.1/Artifiical Hearts and Related Devices R 32/Table of Contents N 32/320/Artificial Hearts and Related Devices N 32/320.1/Coding Requirements for Furnished Before May 1, 2008 N 32/320.2/Coding Requirements for Furnished After May 1, 2008 N 32/320.3/ Ventricular Assist Devices N 32/320.3.1/Postcardiotomy N 32/320.3.2/Bridge-To -Transplantation (BTT) N 32/320.3.3/Destination Therapy (DT) N 32/320.3.4/ Other N 32/320.4/ Replacement Accessories and Supplies for External Ventricular Assist Devices or Any Ventricular Assist Device (VAD) III. -

The Unsuspected Complications of Bacterial Endocarditis Imaged by Gallium-67 Scanning
The Unsuspected Complications of Bacterial Endocarditis Imaged by Gallium-67 Scanning Shobha P. Desai and David L. Yuille Nuclear Medicine Department, St. Luke's Medical Center, Milwaukee, @V&sconsin tivity in the region of the aortic valve which extended into the In this case report, we present a patient with bacterial endocar right atrium (Fig. 1)but was better appreciated on an axial SPECF ditiswho was evaluatedby 67(@imagingfor persistentfever image (Fig. 2). despitetreatmentwith multipleintravenousantibiotics.Afthough cardiac catheterizationconfirmeda densely calcified bicuspid evidence of bactenal endocarditiswas absent wfth @“Gaimag aorticvalve with both stenosis and insufficiencyas well as what ing,the studydemonstratedfindingsthat representcomplica was thoughtto be aveiy largerightsinus ofvalsalva aneurysm.At tions of bacterial endocarditis. The procedure demonstrated surgery, there was evidence of epicarditisand pericarditisand a moderatepencardialuptakeof isotopeandthus pro@4dedthe hugerightsinus of valsalva abscess was foundwhich was eroding first evidence of pehcardi@swhich was later confirmed at sur into the aortic wall. The aortic valve annuluswas debrided, the gery.The studyalsodemonstratedmi@ increasedactivityin abscess cavity was drainedandthe patient's diseased aorticvalve thevicinityoftheaorticrootandnghtattium.A sinusofvalsalva was replacedwith a no. 25 St. Jude's prosthesis (St. JudeMedical abscess, complicatingthe underlyingdiagnosis of bacterialen Inc., St. Paul, MN). The immediatepostoperativeperiodwas docarc@bs,was -

Arrhythmias in Two Patients with Left Ventricular Bypass Transplants'
Br Heart J: first published as 10.1136/hrt.38.7.725 on 1 July 1976. Downloaded from British Heart Journal, 1976, 38, 725-731. Arrhythmias in two patients with left ventricular bypass transplants' Brian M. Kennelly, Peter Corte, Jacques Losman, and Christiaan N. Barnard From the Cardiac Clinic and Department of Cardiothoracic Surgery, Groote Schuur Hospital and the Departments of Medicine and Surgery, University of Cape Town, South Africa Two patients who underwvent left ventricular bypass transplants are described. Both patients sustained post- operative rhythm disturbances of their own hearts during sinus rhythm of the donor hearts. Illustrative examples of atrialflutter, ventricular flutter, ventricular fibrillation, blocked atrial extrasystoles, and double ventricular parasystole in the recipient hearts are presented. The patients tolerated all these arrhythmias well during uninterrupted sinus rhythm in the donor heart. The problems in interpretation of arrhythmias in the presence of two hearts are discussed. [DONOR I IRECIPIENTI Sv C..AOT A ;PULMONARY ARRY http://heart.bmj.com/ RIGHTATRIU_gXARA t,.Y APPENDAGE R.V R.V on September 28, 2021 by guest. Protected copyright. FIG. 1 Position of donor and recipient hearts in anteroposterior view with relevant anasta- moses (Barnard and Losman (1975). Reprinted with permission of South African Medical Journal). The purpose of this report is to illustrate some of right lung and in the right cardiophrenic angle. the bizarre electrocardiograms resulting from Both venae cavae of the donor heart are ligated and cardiac transplantation in man where the recipient the donor right ventricle pumps only its coronary heart is left in situ. The surgical technique was sinus venous return into the recipient's right described in detail by Barnard and Losman (1975). -

Short-Term Exposure to Air Pollution and Cardiac Arrhythmia: a Meta-Analysis and Systematic Review
Int. J. Environ. Res. Public Health 2016, 13, doi:10.3390/ijerph13070642 S1 of S7 Supplementary Materials: Short-Term Exposure to Air Pollution and Cardiac Arrhythmia: A Meta-Analysis and Systematic Review Xuping Song, Yu Liu, Yuling Hu, Xiaoyan Zhao, Jinhui Tian, Guowu Ding and Shigong Wang Figure S1. Flow chart of the literature screening process. Int. J. Environ. Res. Public Health 2016, 13, doi:10.3390/ijerph13070642 S2 of S7 Figure S2. Association between particulate and gaseous components with hospitalization or mortality due to arrhythmia. Int. J. Environ. Res. Public Health 2016, 13, doi:10.3390/ijerph13070642 S3 of S7 Table S1. Search Strategy for PubMed. No. Search Strategy air pollution*/or air pollutant*/or air polluted/or air contamination*/or atmosphere pollution*/or atmosphere pollutant*/ or atmosphere contamination*/or atmospheric pollution*/or atmospheric #1 pollutant*/or atmospheric contamination*/or “particulate matter”/or “PM10”/or “PM2.5”/or ozone/ or “O3”/or “carbon monoxide”/or carbonmonoxide/or “CO“/or “nitrogen dioxide”/or “NO2”/or “sulphur dioxide”/or “sulphur dioxyde”/or “sulfurous anhydride“/or “SO2”.ti,ab. Air Pollution/or Particulate Matter/or Ozone/or Carbon Monoxide/or Nitrogen Dioxide/or Sulfur #2 Dioxide.sh. #3 or/1,2 #4 arrhythmia* /or dysrhythmia* /or “CA”.ti,ab. #5 Arrhythmias, Cardiac.sh. “Sick Sinus Syndrome”/or “SSS”/or “Sick Sinus Node Syndrom”/or Sinus Node Dysfunction*/or #6 Sinus Node Disease*/or Sinus Arrest*.ti,ab. #7 Arrhythmia, Sinus/or Sick Sinus Syndrome/or Sinus Arrest, Cardiac.sh. #8 atrial fibrillation*/or auricular fibrillation*/or “AF".ti,ab. #9 Atrial Fibrillation.sh. -

Cardiac Arrhythmias in Survivors of Sudden Cardiac Death Requiring Impella Assist Device Therapy
Journal of Clinical Medicine Article Cardiac Arrhythmias in Survivors of Sudden Cardiac Death Requiring Impella Assist Device Therapy Khaled Q. A. Abdullah 1,2, Jana V. Roedler 1, Juergen vom Dahl 1, Istvan Szendey 1, Dimitrios Dimitroulis 1, Lars Eckardt 3, Albert Topf 4, Bernhard Ohnewein 4, Lorenz Fritsch 4, Fabian Föttinger 4, Mathias C. Brandt 4, Bernhard Wernly 4,5,6 , Lukas J. Motloch 4 and Robert Larbig 2,3,* 1 Department of Cardiology, Hospital Maria Hilf Moenchengladbach, 41063 Moenchengladbach, Germany; [email protected] (K.Q.A.A.); [email protected] (J.V.R.); [email protected] (J.v.D.); [email protected] (I.S.); [email protected] (D.D.) 2 Department of Cardiology, University Hospital Aachen, RWTH University Aachen, 52062 Aachen, Germany 3 Department of Cardiovascular Medicine, Division of Electrophysiology, University of Muenster, 48149 Muenster, Germany; [email protected] 4 Department of Cardiology, Clinic II for Internal Medicine, University Hospital Salzburg, Paracelsus Medical University, 5020 Salzburg, Austria; [email protected] (A.T.); [email protected] (B.O.); [email protected] (L.F.); [email protected] (F.F.); [email protected] (M.C.B.); [email protected] (B.W.); [email protected] (L.J.M.) 5 Department of Anesthesiology, Perioperative Medicine and Intensive Care Medicine, Paracelsus Medical University of Salzburg, 5026 Salzburg, Austria 6 Center for Public Health and Healthcare Research, Paracelsus Medical University of Salzburg, 5026 Salzburg, Austria Citation: Abdullah, K.Q.A.; Roedler, * Correspondence: [email protected]; Tel.: +49-216-1892-4770 J.V.; vom Dahl, J.; Szendey, I.; Dimitroulis, D.; Eckardt, L.; Topf, A.; Abstract: In this retrospective single-center trial, we analyze 109 consecutive patients (female: 27.5%, Ohnewein, B.; Fritsch, L.; Föttinger, F.; median age: 69 years, median left ventricular ejection fraction: 20%) who survived sudden cardiac et al. -
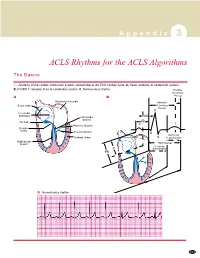
ACLS Rhythms for the ACLS Algorithms
A p p e n d i x 3 ACLS Rhythms for the ACLS Algorithms The Basics 1. Anatomy of the cardiac conduction system: relationship to the ECG cardiac cycle. A, Heart: anatomy of conduction system. B, P-QRS-T complex: lines to conduction system. C, Normal sinus rhythm. Relative Refractory A B Period Bachmann’s bundle Absolute Sinus node Refractory Period R Internodal pathways Left bundle AVN branch AV node PR T Posterior division P Bundle of His Anterior division Q Ventricular Purkinje fibers S Repolarization Right bundle branch QT Interval Ventricular P Depolarization PR C Normal sinus rhythm 253 A p p e n d i x 3 The Cardiac Arrest Rhythms 2. Ventricular Fibrillation/Pulseless Ventricular Tachycardia Pathophysiology ■ Ventricles consist of areas of normal myocardium alternating with areas of ischemic, injured, or infarcted myocardium, leading to chaotic pattern of ventricular depolarization Defining Criteria per ECG ■ Rate/QRS complex: unable to determine; no recognizable P, QRS, or T waves ■ Rhythm: indeterminate; pattern of sharp up (peak) and down (trough) deflections ■ Amplitude: measured from peak-to-trough; often used subjectively to describe VF as fine (peak-to- trough 2 to <5 mm), medium-moderate (5 to <10 mm), coarse (10 to <15 mm), very coarse (>15 mm) Clinical Manifestations ■ Pulse disappears with onset of VF ■ Collapse, unconsciousness ■ Agonal breaths ➔ apnea in <5 min ■ Onset of reversible death Common Etiologies ■ Acute coronary syndromes leading to ischemic areas of myocardium ■ Stable-to-unstable VT, untreated ■ PVCs with -

Severe Hypotension, Bradycardia and Asystole After Sugammadex Administration in an Elderly Patient
medicina Case Report Severe Hypotension, Bradycardia and Asystole after Sugammadex Administration in an Elderly Patient Carmen Fierro 1 , Alessandro Medoro 1 , Donatella Mignogna 1 , Carola Porcile 1 , Silvia Ciampi 1 , Emanuele Foderà 1 , Romeo Flocco 2, Claudio Russo 1,3,* and Gennaro Martucci 2 1 Department of Medicine and Health Sciences, University of Molise, 86100 Campobasso, Italy; c.fi[email protected] (C.F.); [email protected] (A.M.); [email protected] (D.M.); [email protected] (C.P.); [email protected] (S.C.); [email protected] (E.F.) 2 Anesthesia and Intensive Care Unit, “A. Cardarelli” Hospital, Azienda Sanitaria Regionale del Molise, 86100 Campobasso, Italy; romeofl[email protected] (R.F.); [email protected] (G.M.) 3 UOC Governance del Farmaco, Azienda Sanitaria Regionale del Molise, 86100 Campobasso, Italy * Correspondence: [email protected] Abstract: Background and Objectives: Sugammadex is a modified γ-cyclodextrin largely used to prevent postoperative residual neuromuscular blockade induced by neuromuscular aminosteroid blocking agents. Although Sugammadex is considered more efficacious and safer than other drugs, such as Neostigmine, significant and serious complications after its administration, such as hypersen- sitivity, anaphylaxis and, more recently, severe cardiac events, are reported. Case presentation: In this report, we describe the case of an 80-year-old male with no medical history of cardiovascular disease who was scheduled for percutaneous nephrolithotripsy under general anesthesia. The intraoperative course was uneventful; however, the patient developed a rapid and severe hypotension, asystole and cardiac arrest after Sugammadex administration. Spontaneous cardiac activity and hemodynamic Citation: Fierro, C.; Medoro, A.; stability was restored with pharmacological therapy and chest compression. -

Cardiac Lesions Associated with Cardiopulmonary Resuscitation
Rom J Leg Med [19] 1-6 [2011] DOI: 10.4323/rjlm.2011.1 © 2011 Romanian Society of Legal Medicine Cardiac lesions associated with cardiopulmonary resuscitation George Cristian Curcă1, Dan Dermengiu2, Mihai Ceaușu3, Adriana Francisc4, Mugurel Constantin Rusu5, Sorin Hostiuc6 ___________________________________________________________________________________________________________ Abstract: Cardiac arrest is a major cause of morbidity and mortality across the world despite the fact that significant advances were made in basic and advanced life support techniques. Cardiac lesions during CPR are rare, and usually are not involved in thanatologic chains. They can however lead to severe or even lethal complications and may be difficult to differentiate from non-iatrogen trauma, especially in traumatic deaths. We present in this article four cases of cardiac lesions associated with resuscitated cardiac arrest, discuss their forensic significance and review the most important iatrogen cardiac lesions associated with cardiopulmonary resuscitation. Keywords: cardiac contusion, myocardial lesions, cardiopulmonary resuscitation ardiac arrest is a major cause of morbidity and mortality across the world despite the fact that significant advances were made in basic and advanced life support C techniques. Even though cardiopulmonary resuscitation has an overall success rate of 30-40%[1], over 50% of all resuscitated patients die before leaving the hospital, usually due to cardiovascular or CNS complications[2]; many successful resuscitations are in turn