Responses to Static (Isometric) Exercise
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Heart Rate Information Sheet Finding Your Pulse Taking Your Pulse
Heart rate In this activity you will measure your heart rate and investigate the effect that other things have on your heart rate. Information sheet You can measure your heart (pulse) rate anywhere on your body where a major artery is close to the surface of your skin. The easiest places are: • on the front of your forearm • just above your wrist on your thumb side • on the side of your neck about half way between your chin and your ear. Finding your pulse Try to locate your pulse in one of these places, using the tips of your index and middle fingers. You should feel a gentle, regular beat. This is your heart rate. Do not use your thumb, as your thumb has a pulse of its own. Taking your pulse When you find your pulse, use a stopwatch or a watch with a second hand to count how many beats there are in a full minute (60 seconds). In most situations, taking your pulse rate over one minute will give a reasonably accurate result, but if you want to take your pulse after exercise, you should do so over a much shorter time interval. After exercise your pulse rate will be changing rapidly. To get a reasonably accurate result, start to measure the rate immediately after the exercise and count the number of beats in 10 seconds. Multiply this number by six to find your heart rate. For an adult, a normal resting heart rate is between 60–100 beats a minute. The fitter you are, the lower your resting heart beat will be. -

Comparisons of Perceived Exertion of Elliptical Training Versus Treadmill
COMPARISONS OF PERCEIVED EXERTION ON ELLIPTICAL TRAINING VERSUS TREADMILL EXERCISE A Thesis Presented to the Faculty of the College of Education Morehead State University In Partial Fulfillment of the Requirements for the Degree Master of Arts by Marcisha Brazley July, 2002 Mf,IJ._ TIIEiS!S {,,( 3.11012.... B 'Z 'J..7 c. COMPARISONS OF PERCEIVED EXERTION ON ELLIPTICAL TRAINING VERSUS TREADMILL EXERCISE Marcisha Brazley, M.A. Morehead State University, 2002 Director of Thesis: --'--=----''---c=.---''-'---..,_,,-"--"-"'.=..c--"'~-Ao.,-.Q?,.j:!sr j;; ,,{, 0, Statement of the Problem: The relationship between rates of perceived exertion (RPE) during elliptical trainer exercise and treadmill exercise is undefined. Therefore, the purpose of this investigation was to compare and determine whether there are differences in RPE with respect to submaximal workloads between elliptical trainer exercise and treadmill exercise. Sources of d,ata: Five normotensive males, age 21 to 25 years (22.4 ± 1.7) and six normotensive females, age 20 to 23 years (21 ±1.2), VO2 max values 30-59 ml/min/kg were recruited from the Health, Physical Education, and Exercise Science classes at Morehead State University (M.S.U.) and the Wellness Center at Morehead State University. Methods: Each subject completed one graded exercise test on a treadmill as determined by a Bruce protocol. On a separate day, each subject completed one graded exercise test, as determined by a predetermined protocol, on a Precor® EFX544 elliptical cross trainer. The second test was conducted at least 48 hours after the first test. Rate of perceived exertion and heart rate values were recorded after every three minutes of each exercise session. -

Heart to Heart - STEAM Activity
Heart to Heart - STEAM Activity Purpose: The main objective of this exercise is to introduce how the human heart works. This lesson will be divided into four different lessons, including an introduction to heart anatomy, heart beats and pulses, and the circulatory system. We will be using coloring activities, stethoscopes, and handmade pumps to reinforce the concepts seen in this lesson. Vocabulary ● Artery: A blood vessel that carries blood high in oxygen content away from the heart to the farthest reaches of the body. ● Vein: a Blood vessel that carries blood low in oxygen content from the body back to the heart. ● Atrium: One of the two upper cavities of the heart that passes blood to the ventricles. ● Ventricles: One of the two lower chambers of the heart that receives blood from the atria. ● Valves: Tissue-paper thin membranes attached to the heart wall that constantly open and close to regulate blood flow. ● Pulse: A rhythmical, mechanical throbbing of the arteries as blood pumps through them. ● Heart Rate: The number of times per minute that the heart contracts - the number of heart beats per minute (bpm). ● Taquicardia: A high resting heart rate that is usually higher than 100 beats per minute. ● Bradycardia: A low resting heart rate that is usually lower than 60 beats per minute. ● Circulation: The movement of blood through the vessels of the body by the pumping action of the heart. It distributes nutrients and oxygen and removes waste products from all parts of the body. ● Pulmonary Circulation: The portion of the circulatory system that carries deoxygenated blood from the heart to the lungs and oxygenated blood back to the heart. -

Energy and Training Module ITU Competitive Coach
37 energy and training module ITU Competitive Coach Produced by the International Triathlon Union, 2007 38 39 energy & training Have you ever wondered why some athletes shoot off the start line while others take a moment to react? Have you every experienced a “burning” sensation in your muscles on the bike? Have athletes ever claimed they could ‘keep going forever!’? All of these situations involve the use of energy in the body. Any activity the body performs requires work and work requires energy. A molecule called ATP (adenosine triphosphate) is the “energy currency” of the body. ATP powers most cellular processes that require energy including muscle contraction required for sport performance. Where does ATP come from and how is it used? ATP is produced by the breakdown of fuel molecules—carbohydrates, fats, and proteins. During physical activity, three different processes work to split ATP molecules, which release energy for muscles to use in contraction, force production, and ultimately sport performance. These processes, or “energy systems”, act as pathways for the production of energy in sport. The intensity and duration of physical activity determines which pathway acts as the dominant fuel source. Immediate energy system Fuel sources ATP Sport E.g. carbohydrates, energy performance proteins, fats “currency” Short term energy system E.g. swimming, cycling, running, transitions Long term energy system During what parts of a triathlon might athletes use powerful, short, bursts of speed? 1 2 What duration, intensity, and type of activities in a triathlon cause muscles to “burn”? When in a triathlon do athletes have to perform an action repeatedly for longer than 10 or 15 3 minutes at a moderate pace? 40 energy systems Long Term (Aerobic) System The long term system produces energy through aerobic (with oxygen) pathways. -

Toolbox-Talks--Blood-Pressure.Pdf
TOOLBOX Toolbox Talk #1 TALKS Blood Pressure vs. Heart Rate While your blood pressure is the force of your blood moving through your blood vessels, your heart rate is the number of times your heart beats per minute. They are two separate measurements and indicators of health. • For people with high blood pressure (HBP or hypertension), there’s no substitute for measuring blood pressure. • Heart rate and blood pressure do not necessarily increase at the same rate. A rising heart rate does not cause your blood pressure to increase at the same Quarter: rate. Even though your heart is beating more times a minute, healthy blood BLOOD vessels dilate (get larger) to allow more blood to flow through more easily. PRESSURE When you exercise, your heart speeds up so more blood can reach your muscles. It may be possible for your heart rate to double safely, while your blood pressure may respond by only increasing a modest amount. Talk Number: Heart Rate and Exercise 1 In discussions about high blood pressure, you will often see heart rate Blood mentioned in relation to exercise. Your target heart rate is based on age and Pressure can help you monitor the intensity of your exercise. vs. • If you measure your heart rate (take your pulse) before, during and after Heart Rate physical activity, you’ll notice it will increase over the course of the exercise. • The greater the intensity of the exercise, the more your heart rate will increase. • When you stop exercising, your heart rate does not immediately return to your normal (resting) heart rate. -

Energy Expenditure During Acute Weight Training Exercises in Healthy Participants: a Preliminary Study
applied sciences Article Energy Expenditure during Acute Weight Training Exercises in Healthy Participants: A Preliminary Study Muhammad Adeel 1,2, Chien-Hung Lai 3,4, Chun-Wei Wu 2, Jiunn-Horng Kang 3,4, Jian-Chiun Liou 2, Hung-Chou Chen 3,5 , Meng-Jyun Hong 2 and Chih-Wei Peng 1,2,6,* 1 International PhD Program in Biomedical Engineering, College of Biomedical Engineering, Taipei Medical University, Taipei 110, Taiwan; [email protected] 2 School of Biomedical Engineering, College of Biomedical Engineering, Taipei Medical University, Taipei 110, Taiwan; [email protected] (C.-W.W.); [email protected] (J.-C.L.); [email protected] (M.-J.H.) 3 Department of Physical Medicine and Rehabilitation, School of Medicine, College of Medicine, Taipei Medical University, Taipei 110, Taiwan; [email protected] (C.-H.L.); [email protected] (J.-H.K.); [email protected] (H.-C.C.) 4 Department of Physical Medicine and Rehabilitation, Taipei Medical University Hospital, Taipei 110, Taiwan 5 Department of Physical Medicine and Rehabilitation, Shuang Ho Hospital, Taipei Medical University, New Taipei City 235, Taiwan 6 School of Gerontology Health Management, College of Nursing, Taipei Medical University, Taipei 110, Taiwan * Correspondence: [email protected]; Tel./Fax: +886-2-2736-1661 (ext. 3070) Abstract: Energy expenditure during weight training exercises produces great fitness and health benefits for humans, but few studies have investigated energy expenditure directly during weight training. Therefore, in this study, we aimed to determine energy costs during three training sessions Citation: Adeel, M.; Lai, C.-H.; Wu, consisting of three different exercises. -

The Effects of Motion on Trunk Biomechanics
Clinical Biomechanics 15 (2000) 703±717 www.elsevier.com/locate/clinbiomech Review paper The eects of motion on trunk biomechanics K.G. Davis, W.S. Marras * Biodynamics Laboratory, Room 210, 210 Baker Systems, 1971 Neil Avenue, The Ohio State University, Columbus, OH 43210, USA Received 15 June 2000; accepted 16 June 2000 Abstract Objective. To review the literature that evaluates the in¯uence of trunk motion on trunk strength and structural loading. Background. In recent years, trunk dynamics have been identi®ed as potential risk factors for developing low-back disorders. Consequently, a better understanding of the underlying mechanisms involved in trunk motion is needed. Methods. This review summarizes the results of 53 studies that have evaluated trunk motion and its impact on several biome- chanical outcome measures. The biomechanical measures consisted of trunk strength, intra-abdominal pressure, muscle activity, imposed trunk moments, and spinal loads. Each of these biomechanical measures was discussed in relation to the existing knowledge within each plane of motion (extension, ¯exion, lateral ¯exion, twisting, and asymmetric extension). Results. Trunk strength was drastically reduced as dynamic motion increased, and males were impacted more than females. Intra- abdominal pressure seemed to only be aected by trunk dynamics at high levels of force. Trunk moments were found to increase monotonically with increased trunk motion. Both agonistic and antagonistic muscle activities were greater as dynamic character- istics increased. As a result, the three-dimensional spinal loads increase signi®cantly for dynamic exertions as compared to isometric conditions. Conclusions. Trunk motion has a dramatic aect on the muscle coactivity, which seems to be the underlying source for the decrease strength capability as well as the increased muscle force, IAP, and spinal loads. -

Effects of Vasodilation and Arterial Resistance on Cardiac Output Aliya Siddiqui Department of Biotechnology, Chaitanya P.G
& Experim l e ca n i t in a l l C Aliya, J Clinic Experiment Cardiol 2011, 2:11 C f a Journal of Clinical & Experimental o r d l DOI: 10.4172/2155-9880.1000170 i a o n l o r g u y o J Cardiology ISSN: 2155-9880 Review Article Open Access Effects of Vasodilation and Arterial Resistance on Cardiac Output Aliya Siddiqui Department of Biotechnology, Chaitanya P.G. College, Kakatiya University, Warangal, India Abstract Heart is one of the most important organs present in human body which pumps blood throughout the body using blood vessels. With each heartbeat, blood is sent throughout the body, carrying oxygen and nutrients to all the cells in body. The cardiac cycle is the sequence of events that occurs when the heart beats. Blood pressure is maximum during systole, when the heart is pushing and minimum during diastole, when the heart is relaxed. Vasodilation caused by relaxation of smooth muscle cells in arteries causes an increase in blood flow. When blood vessels dilate, the blood flow is increased due to a decrease in vascular resistance. Therefore, dilation of arteries and arterioles leads to an immediate decrease in arterial blood pressure and heart rate. Cardiac output is the amount of blood ejected by the left ventricle in one minute. Cardiac output (CO) is the volume of blood being pumped by the heart, by left ventricle in the time interval of one minute. The effects of vasodilation, how the blood quantity increases and decreases along with the blood flow and the arterial blood flow and resistance on cardiac output is discussed in this reviewArticle. -
Fundamentals of Biomechanics Duane Knudson
Fundamentals of Biomechanics Duane Knudson Fundamentals of Biomechanics Second Edition Duane Knudson Department of Kinesiology California State University at Chico First & Normal Street Chico, CA 95929-0330 USA [email protected] Library of Congress Control Number: 2007925371 ISBN 978-0-387-49311-4 e-ISBN 978-0-387-49312-1 Printed on acid-free paper. © 2007 Springer Science+Business Media, LLC All rights reserved. This work may not be translated or copied in whole or in part without the written permission of the publisher (Springer Science+Business Media, LLC, 233 Spring Street, New York, NY 10013, USA), except for brief excerpts in connection with reviews or scholarly analysis. Use in connection with any form of information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed is forbidden. The use in this publication of trade names, trademarks, service marks and similar terms, even if they are not identified as such, is not to be taken as an expression of opinion as to whether or not they are subject to proprietary rights. 987654321 springer.com Contents Preface ix NINE FUNDAMENTALS OF BIOMECHANICS 29 Principles and Laws 29 Acknowledgments xi Nine Principles for Application of Biomechanics 30 QUALITATIVE ANALYSIS 35 PART I SUMMARY 36 INTRODUCTION REVIEW QUESTIONS 36 CHAPTER 1 KEY TERMS 37 INTRODUCTION TO BIOMECHANICS SUGGESTED READING 37 OF UMAN OVEMENT H M WEB LINKS 37 WHAT IS BIOMECHANICS?3 PART II WHY STUDY BIOMECHANICS?5 BIOLOGICAL/STRUCTURAL BASES -

Jugular Venous Pressure
NURSING Jugular Venous Pressure: Measuring PRACTICE & SKILL What is Measuring Jugular Venous Pressure? Measuring jugular venous pressure (JVP) is a noninvasive physical examination technique used to indirectly measure central venous pressure(i.e., the pressure of the blood in the superior and inferior vena cava close to the right atrium). It is a part of a complete cardiovascular assessment. (For more information on cardiovascular assessment in adults, see Nursing Practice & Skill ... Physical Assessment: Performing a Cardiovascular Assessment in Adults ) › What: Measuring JVP is a screening mechanism to identify abnormalities in venous return, blood volume, and right heart hemodynamics › How: JVP is determined by measuring the vertical distance between the sternal angle and the highest point of the visible venous pulsation in the internal jugular vein orthe height of the column of blood in the external jugular vein › Where: JVP can be measured in inpatient, outpatient, and residential settings › Who: Nurses, nurse practitioners, physician assistants, and treating clinicians can measure JVP as part of a complete cardiovascular assessment What is the Desired Outcome of Measuring Jugular Venous Pressure? › The desired outcome of measuring JVP is to establish the patient’s JVP within the normal range or for abnormal JVP to be identified so that appropriate treatment may be initiated. Patients’ level of activity should not be affected by having had the JVP measured ICD-9 Why is Measuring Jugular Venous Pressure Important? 89.62 › The JVP is -
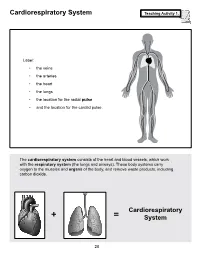
Cardiorespiratory System Teaching Activity 1
Cardiorespiratory System Teaching Activity 1. Label: • the veins • the arteries • the heart • the lungs • the location for the radial pulse • and the location for the carotid pulse. The cardiorespiratory system consists of the heart and blood vessels, which work with the respiratory system (the lungs and airways). These body systems carry oxygen to the muscles and organs of the body, and remove waste products, including carbon dioxide. Cardiorespiratory + = System 28 The Most Important Muscle: The Heart Teaching Activity 1, continued. In the circulatory system, the heart is a muscle that acts as a pump. In fact, the heart is a double pump. Blood that needs oxygen enters the heart and is pumped by the first pump to the lungs. The second pump of the heart pumps the oxygen-rich blood to all the other parts of the body. This gives the heart its common, “lub-dub” sound. The number of times the heart pumps, or beats, is counted in a minute. This is known as the pulse rate. A person’s pulse is affected by their current level of activity. If you are sleeping or do no physical activity at all, your heart is pumping at a resting heart rate. When active, you are using all your body systems. These systems require fuel in the form of calories (found in food), and oxygen (what you breathe). The more active you are, the Hearty Facts more fuel your muscles need. This is why your breathing rate and your heart rate increase when • Your system of blood vessels (arteries, you exercise. veins, and capillaries) is over 60,000 miles long. -

Cardiovascular System: Heart
Cardiovascular System: Heart Cardiovascular System – Heart Conducting cells: Cardiac Electrophysiology Cardiac cells specialized to quickly spread action potentials across myocardium • Weak force generators System allows for orderly, sequential depolarization and Intrinsic Conduction System: contraction of heart Normal sinus rhythm: 1) AP originates at SA node 2) SA node fires at 60 – 100 beats / min Atrial internodal tracts Sinoatrial node: (SA node) 3) Correct myocardial activation sequence • Located in right atrial wall • Initiates action potentials (APs) • Pacemaker (~ 80 beats / min) Bundle branches Atrioventricular node: (AV Node) • Connects atria to ventricles • Slowed conduction velocity • Ventricular filling Purkinje Bundle of His fibers Marieb & Hoehn (Human Anatomy and Physiology, 8th ed.) – Figure 18.14 1 Cardiovascular System – Heart Cardiac Electrophysiology The autonomic nervous system can directly affect the heart rate; these effects are called chronotropic effects Recall: spontaneous depolarization = VG Na+ channels Positive chronotrophic effects: (increase heart rate) • Under sympathetic control Leads to g ; cells SA Na NE node reach threshold more rapidly Sinoatrial node Pharmacology: β1 receptors β-blockers (e.g., propanolol) Negative chronotrophic effects: (decrease heart rate) • Under parasympathetic control Leads to gNa; cells reach threshold SA less rapidly ACh node Leads to gK; cells hyperpolarized during Muscarinic receptors repolarization stage (further from threshold) Costanzo (Physiology, 4th ed.) – Figure