A Modified Method for Punctoplasty: “Excisional Punctoplasty with the Guidance of a 27 G Rycroft Cannula”
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Icare Eye Hospital Rate List 2015
ICARE EYE HOSPITAL & POST GRADUATE INSTITUTE E-3A, Sector – 26, Noida – 201301 Tel:- 0120-2477600 / 02, Counselor: 0120-2477621 Fax: 0120-2556389 / Appointments: 9811880015 Email: [email protected] / Web: www.icarehospital.org ICARE EYE HOSPITAL RATE LIST 2015 S No. PARTICULAR TARIFF (₹) I CONSULTATION NEW PATIENT VALID FOR 7 DAYS (FIRST TIME CONSULTATION : REGISTRATION + 1 ₹ 600/- CONSULTATION) 2 REVIEW CONSULTATION VALID FOR 7 DAYS ₹ 500/- 3 EMERGENCY CONSULTATION FOR 7 DAYS ₹ 800/- 4 LOW VISUAL AIDS ASSESSMENT CHARGES ₹ 600/- 5 VISION THERAPY CHARGES FOR PER SITTING ₹ 200/- 6 COST OF VISION THERAPY SOFTWARE (CD) ₹ 6,000/- 7 AMBLYOPIA (CD) ₹ 4,000/- II INVESTIGATIONS 1 Digital F.F.A (Fundus Fluoroscein Angiography)(Inclusive of Fundus photo) ₹ 2,500/- 2 Colour Fundus Photo - Digital ₹ 600/- 3 Colour Slit-lamp photo ₹ 600/- 4 Duplicate color prints (FFA/OCT/CLINICAL PHOTO) ₹ 300/- 5 Orthoptic ₹ 250/- 6 OCT (Optical Coherence Tomography) ₹ 2,500/- A Repeat OCT (within 2 months) with printout ₹ 800/- B Anterior Segment OCT ₹ 2,500/- 7 Ultrasonography (U/S) A A Scan – Single Eye ₹ 600/- B B Scan – Single Eye ₹ 1,000/- C UBM - Single Eye ₹ 1,500/- 8 Computerized field analysis A Humphrey Visual Fields (HVF) both eyes ₹ 1,500/- B Humphrey Visual Fields (HVF) One eye ₹ 750/- 9 Diurnal Variation of Tension (Day DVT ) A 5 times tension (Done in both eyes)] ₹ 500/- Page 1 10 Pachymetry (Both eyes) A Ultrasound (Central Corneal Thickness- CST) ₹ 600/- B Optical ₹ 600/- 11 Corneal Topography A Single Eye ₹ 1,000/- B Both Eyes ₹ 2,000/- 12 -

Local Coverage Determination (LCD): Diagnostic Evaluation and Medical Management of Moderate-Severe Dry Eye Disease (DED) (L36232)
Local Coverage Determination (LCD): Diagnostic Evaluation and Medical Management of Moderate-Severe Dry Eye Disease (DED) (L36232) Links in PDF documents are not guaranteed to work. To follow a web link, please use the MCD Website. Contractor Information CONTRACTOR NAME CONTRACT TYPE CONTRACT NUMBER JURISDICTION STATE(S) First Coast Service Options, Inc. A and B MAC 09101 - MAC A J - N Florida First Coast Service Options, Inc. A and B MAC 09102 - MAC B J - N Florida First Coast Service Options, Inc. A and B MAC 09201 - MAC A J - N Puerto Rico Virgin Islands First Coast Service Options, Inc. A and B MAC 09202 - MAC B J - N Puerto Rico First Coast Service Options, Inc. A and B MAC 09302 - MAC B J - N Virgin Islands LCD Information Document Information LCD ID Original Effective Date L36232 For services performed on or after 11/22/2015 LCD Title Revision Effective Date Diagnostic Evaluation and Medical Management of For services performed on or after 01/08/2019 Moderate-Severe Dry Eye Disease (DED) Revision Ending Date Proposed LCD in Comment Period N/A N/A Retirement Date Source Proposed LCD N/A DL36232 Notice Period Start Date AMA CPT / ADA CDT / AHA NUBC Copyright 10/08/2015 Statement CPT codes, descriptions and other data only are Notice Period End Date copyright 2019 American Medical Association. All Rights 11/22/2015 Reserved. Applicable FARS/HHSARS apply. Current Dental Terminology © 2019 American Dental Association. All rights reserved. Copyright © 2019, the American Hospital Association, Created on 01/02/2020. Page 1 of 12 Chicago, Illinois. -

Cataract Surgery
Cataract surgery From Wikipedia, the free encyclopedia Jump to: navigation, search This article includes a list of references, related reading or external links, but its sources remain unclear because it lacks inline citations. Please improve this article by introducing more precise citations. (May 2011) Cataract surgery Intervention Cataract in Human Eye- Magnified view seen on examination with a slit lamp ICD-9-CM 13.19 MeSH D002387 Cataract surgery is the removal of the natural lens of the eye (also called "crystalline lens") that has developed an opacification, which is referred to as a cataract. Metabolic changes of the crystalline lens fibers over time lead to the development of the cataract and loss of transparency, causing impairment or loss of vision. Many patients' first symptoms are strong glare from lights and small light sources at night, along with reduced acuity at low light levels. During cataract surgery, a patient's cloudy natural lens is removed and replaced with a synthetic lens to restore the lens's transparency.[1] Following surgical removal of the natural lens, an artificial intraocular lens implant is inserted (eye surgeons say that the lens is "implanted"). Cataract surgery is generally performed by an ophthalmologist (eye surgeon) in an ambulatory (rather than inpatient) setting, in a surgical center or hospital, using local anesthesia (either topical, peribulbar, or retrobulbar), usually causing little or no discomfort to the patient. Well over 90% of operations are successful in restoring useful vision, with a low complication rate.[2] Day care, high volume, minimally invasive, small incision phacoemulsification with quick post-op recovery has become the standard of care in cataract surgery all over the world. -

Fixing Patients' Problems
CAN TABLETS WORK FOR EMR? P. 12 • CODING TIPS FOR CROSS-LINKING P. 16 A FRESH ANGLE ON RESIDENT TRAINING P. 68 • SIXTH CRANIAL NERVE DYSFUNCTION IN KIDS P. 72 Review of Ophthalmology Vol. XXIV, No. 4 • April 2017 • Fighting for Patient Care • Avoiding Problems Using OCT • Managing Refractive Surprises Problems • Optical Biometry Roundup Care • Avoiding No. 4 • April 2017 • Fighting for Patient Review of Ophthalmology Vol. XXIV, STEM THE TIDE OF EXCESSIVE TEARING P. 76 • POST-INJECTION IOP SPIKES P. 96 April 2017 reviewofophthalmology.com Fixing Patients’ Problems Expert surgeons give you the tools you need to succeed. ALSO INSIDE: Sizing Up Optical Biometers P. 58 001_rp0417_fc-WB.indd 1 3/24/17 12:52 PM VISIT US AT ASCRS BOOTH #1022 It’s all in CHOOSE A SYSTEM THAT EMPOWERS YOUR EVERY MOVE. Technique is more than just the motions. Purposefully engineered for exceptional versatility and high-quality performance, the WHITESTAR SIGNATURE® PRO Phacoemulsification System gives you the clinical flexibility, confidence and control to free your focus for what matters most in each procedure. How do you phaco? Join the conversation at WWW.ABBOTTPHACO.COM Rx Only INDICATIONS: The WHITESTAR SIGNATURE® PRO System is a modular ophthalmic microsurgical system that facilitates anterior segment (cataract) surgery. The modular design allows the users to configure the system to meet their surgical requirements. IMPORTANT SAFETY INFORMATION: Risks and complications of cataract surgery may include broken ocular capsule or corneal burn. This device is only to be used by a trained, licensed physician. ATTENTION: Reference the labeling for a complete listing of Indications and Important Safety Information. -

Primary External Dacryocystorhinostomy
11 Primary External Dacryocystorhinostomy Richard H. Hart, Suzanne Powrie, and Geoffrey E. Rose The watering eye may be the result of excessive tear production, abnor- malities of lid position or movement, lacrimal canalicular pump failure, or obstruction of the outfl ow tract. With external dacryocystorhinos- tomy (DCR), the lacrimal sac is directly incorporated into the lateral wall of the nose, so that the canaliculi drain directly into the nasal cavity. The aims of surgery are twofold: to eliminate fl uid and mucus reten- tion within the lacrimal sac and prevent sac enlargement (as a muco- cele) – the latter leading to intermittent viscous ocular discharge – and to bypass the higher hydraulic resistance of the nasolacrimal duct, thereby increasing tear conductance and aiding the relief of epiphora. Indications for Surgery 1. Primary acquired nasolacrimal duct obstruction 2. Secondary acquired nasolacrimal duct obstruction attributed, for example, to dacryolithiasis, endonasal surgery, infl ammatory nasal or sinus disease, or prior midfacial injury 3. Persistent congenital nasolacrimal duct obstruction, often after unsuccessful probing or intubation of the nasolacrimal duct 4. Functional obstruction of lacrimal outfl ow with decreased tear conductance as a result of: (a) Stenosis, but not occlusion, of the nasolacrimal duct (b) Lacrimal canalicular pump failure from age-related laxity of the lower eyelid, or after facial nerve palsy 5. Acute or chronic dacryocystitis; the former group requiring initial treatment with systemic antibiotics Surgical Principles External DCR should establish a low-resistance drainage pathway between the conjunctival tear sac and the nasal cavity, by conversion of the lacrimal sac into part of the lateral nasal wall. -
Summary of Safety and Effectivness (SSED)
SUMMARY OF SAFETY AND EFFECTIVENESS DATA (SSED) I. GENERAL INFORMATION Device Generic Name: Intraocular Pressure Lowering Implant Device Trade Name: Hydrus® Microstent Device Procode: OGO Applicant’s Name and Address: Ivantis, Inc. 38 Discovery, Suite 150 Irvine, CA 92618 Date(s) of Panel Recommendation: None Premarket Approval Application (PMA) Number: P170034 Date of FDA Notice of Approval: August 10, 2018 II. INDICATIONS FOR USE The Hydrus® Microstent is indicated for use in conjunction with cataract surgery for the reduction of intraocular pressure (IOP) in adult patients with mild to moderate primary open-angle glaucoma (POAG). III. CONTRAINDICATIONS The Hydrus® Microstent is contraindicated under the following circumstances or conditions: • In eyes with angle closure glaucoma • In eyes with traumatic, malignant, uveitic, or neovascular glaucoma or discernible congenital anomalies of the anterior chamber (AC) angle. IV. WARNINGS AND PRECAUTIONS The warnings and precautions can be found in the Hydrus® Microstent labeling. V. DEVICE DESCRIPTION The Hydrus® Microstent is a crescent-shaped, implantable microstent pre-loaded onto a hand-held delivery system. The microstent (Figure 1) is composed of nitinol, a metal alloy of nickel (Ni) and titanium (Ti) with super-elastic properties. The implant is laser cut from nitinol tubing to a design with alternating “spines” for structural support and “windows” to provide PMA P170034: FDA Summary of Safety and Effectiveness Data Page 1 outflow pathways for aqueous humor. After laser cutting, the shape of the implant is heat-set to a curvature intended to match the curvature of Schlemm’s canal and is electro- polished to create a smooth surface. The microstent is approximately 8 mm in overall length with major and minor axes of 292 µm and 185 µm, respectively. -

Operative Dictations in Ophthalmology Eric D
Operative Dictations in Ophthalmology Eric D. Rosenberg • Alanna S. Nattis Richard J. Nattis Editors Operative Dictations in Ophthalmology Editors Eric D. Rosenberg Alanna S. Nattis Ophthalmology Resident Cornea and Refractive Surgery Fellow Department of Ophthalmology Ophthalmic Consultants of Long Island New York Medical College Rockville Centre, NY, USA Valhalla, NY, USA Richard J. Nattis Chief of Ophthalmology and Clinical Professor Department of Ophthalmology Good Samaritan Hospital West Islip, NY, USA ISBN 978-3-319-45494-8 ISBN 978-3-319-45495-5 (eBook) DOI 10.1007/978-3-319-45495-5 Library of Congress Control Number: 2017932292 © Springer International Publishing Switzerland 2017 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, express or implied, with respect to the material contained herein or for any errors or omissions that may have been made. -

Curriculum Vitae
Kashkouli MB, CV CURRICULUM VITAE Mohsen Bahmani Kashkouli, MD Section Subject I Personal Information II 1. Executive Position 2. Journal Editor 3. Organizing a meeting 4. Journals’ reviewer, 5. Establishing an organization III Education IV Work Experience V Trained Fellows VI Edited Books/ Chapters VII Peer Reviewed Paper Publications VIII Courses Attended IX Directing Workshops/Courses/ Symposia X Conference Abstracts XI Invited (Guest) Speaker XII Awards XIII Innovations XIV Ongoing Research Projects XV Referees XVI Interests XVII Affiliations 1 Kashkouli MB, CV I. PERSONAL INFORMATION NAME: Mohsen Bahmani Kashkouli WORK ADDRESS University Hospital Private Office Rassoul Akram Hospital No.:49, West Brazil- South Sattarkhan-Niayesh Avenue Sheikhbahaee intersection, POBox: 14455-364 Tehran, Iran Tehran, Iran Phone: +98 21 66559595 Phone: +98 21 88065620 Fax: +98 21 66509162 Fax: +98 21 66558811 Email [email protected] DATE OF BIRTH: 09/January/1967 PLACE OF BIRTH: Gachsaran , Iran Language: Farsi, English, Turkish II. SCIENTIFIC & EXECUTIVE POSITIONS 1. Executive Positions 2. Professor, Head of Oculo-Facial Plastic Surgery, Rassoul Akram Hospital, Iran University of Medical Sciences (www.iums.ac.ir), Tehran, Iran. 3. Regional (Iran and Turkey) Vice President of Middle East African Council of Ophthalmology (MEACO).(www.meaco.org), Since Nov. 2019. 4. Vice President of Middle East African Council of Ophthalmology (MEACO) in Middle East (www.meaco.org), Since 2012. 5. Vice President, Middle East African Society of Ophthalmic Plastic and Reconstructive Surgery (MEASOPRS, www.meaco.org ), Since June 2016. 6. Scientific Coordinator, Middle East African Society of Ophthalmic Plastic and Reconstructive Surgery (MEASOPRS, www.meaco.org ), 2012-2016. 7. Scientific Director and chair of International relation section, Iranian Society of Ophthalmic Plastic and Reconstructive Suregry (IrSOPRS, www.irso.org/irsoprs), Tehran, Iran, Since 2007. -

Co-Managing Premium Iols: the Optometrist's Role COPE #26507-PO
Disclosures Walter O. Whitley, OD, MBA, FAAO has received consulting fees, honorarium or research funding from: Rapid Fire Grand Rounds • Alcon • Science Based Health COPE#52118- PO • Allergan • Shire • Bausch and Lomb • Sun Pharmaceuticals • Biotissue • TearLab Corporation • Beaver-Visitec • Tearscience Walter O. Whitley, OD, MBA, FAAO • Ocusoft Director of Optometric Services Virginia Eye Consultants • Publications Residency Program Supervisor – Advanced Ocular Care – Co-Chief Medical Editor PCO at Salus University – Review of Optometry – Contributing Editor – Optometry Times – Editorial Advisory Board Virginia Eye Consultants Pearls on Optometric Co-management Tertiary Referral Eye Care Since 1963 • John D. Sheppard, MD, MMSc • Walter Whitley, OD, MBA, FAAO • Get to know your surgeon • Stephen V. Scoper, MD • Mark Enochs, OD • David Salib, MD • Chris Kuc, OD, FAAO • Convey patient preferences, observations and • Elizabeth Yeu, MD • Cecelia Koetting, OD, FAAO • Thomas J. Joly, MD, PhD • Leanna Olennikov, OD conditions to your surgeon • Dayna M. Lago, MD • Chris Kruthoff, OD • Constance Okeke, MD, MSCE • Jillian Janes, OD • Inform your patients on your role in perioperative • Esther Chang, MD • Jay Starling, MD care • Samantha Dewundara, MD • Rohit Adyanthaya, MD • Successful co-management is the result of • Albert Cheung, MD continuous communication 1 Today’s Optometrists TODAY’S CATARACT PATIENT • In 2015, people aged 50 and older represented 45% of the US population1 “To be on the cutting edge of • There were approximately 4 million cataract procedures in 2015 and optometry, you need to be on the that number is expected to grow by 3% in 20166 cutting edge of science and Active Outgoing Still Digitally technology.” working savvy 1. -

Leicester 14 & 15 June 2012 Programme & Abstract Book
Leicester 14 & 15 June 2012 Programme & abstract book About BOPSS BOPSS, the British Oculoplastic Surgery Society, was founded in 2000 with the aim of bringing together surgeons in the United Kingdom and Ireland who share an interest in Ophthalmic Plastic and Reconstructive Surgery, Lacrimal, Orbital and Aesthetic (cosmetic), Eyelid and Facial Surgery. Brian Leatherbarrow Richard Collin, Brian Leatherbarrow and Jane Olver, the Founding Executive Committee, President of BOPSS saw the necessity for such a society as a reflection of the interest in oculoplastic surgery as a sub-speciality of ophthalmology. Aims of BOPSS 1. To advance education, research and the quality of clinical practice in the area of ophthalmology known as oculoplastic surgery. This field comprises periocular, plastic reconstructive and aesthetic surgery, specialising in the eyelids, lacrimal system, orbit, upper and mid-face. 2. To provide an opportunity for Members to meet and discuss Oculoplastic Surgery. Ben Parkin 3. To provide information and advice to the public in order to gain a better understanding BOPSS Secretary of oculoplastic surgery. Members BOPSS has over 120 consultant oculoplastic surgeon members and holds an annual scientific meeting. In order to become a member of BOPSS, you need to send a written submission to the Executive Secretary. You can download the application form from the website (Membership > Application). Prior meetings BOPSS has organized meetings in Birmingham (2001, 2003 and 2005), Manchester (2002 David Verity BOPSS Treasurer and 2004), London (2006), Leeds (2007), Newcastle (2008), Cambridge (2009), Edinburgh (2010) and Cardiff (2011). The meeting in 2006 was co-organized by the European Society Of Ophthalmic Plastic And Reconstructive Surgery (ESOPRS). -
Referral Request Form
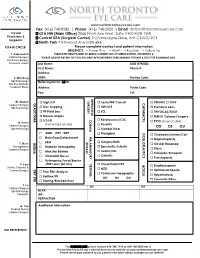
0 www.northtorontoeyecare.com Fax: (416) 748-8582 | Phone: (416) 748-2020 | Email: [email protected] Ocular GTA NW (Main Office) 2065 Finch Ave West, Suite #400 M3N 1W8 Physicians & Central GTA (Surgical Center) 2 Champagne Drive, Unit C2 M3J 2C5 Surgeons North York 7 Elmwood Ave M2N 6R6 PLEASE CIRCLE: Please complete contact and patient information. URGENCY: □ Same Day □ ASAP □ Routine □ Follow Up T. Rabinovitch PLEASE INFORM PATIENT TO BRING CURRENT LIST OF MEDICATIONS, EYE DROPS & Cataract Surgery PLEASE ADVISE PATIENT OF TWO POSSIBLE APPOINTMENTS (PRELIMINARY TESTING & DOCTOR EXAMINATION) Refractive Surgery Cornea & Uveitis Last Name: ________________ First Name: ________ DOB (Y/M/D): First Name: _______________________________________ Phone #: ____________________ Address:_ J. Waisberg OHIP: _ Version Code:Version Ophthalmology Referring Doctor: Dr. Dry Eye Disease Cosmetic Botox Address: Postal Code: T Fax: Tel: _____ _________ REFRACTIVE SURGERY M. Azadeh GLAUCOMA High IOP Lasik/PRK Consult CATARACTS PRIVATE OHIP Cataract Surgery Ophthalmology Disc Cupping RLE/CLE Premium Lens VF Field Loss ICL TRIFOCAL/EDOF Narrow Angles FEMTO Cataract Surgery CORNEA Keratoconus/CXL SLT/LPI N. Pesin _______________________________________ PCO (laser on site) (Performed on site) Keratitis Cataract Surgery________________ OD OS OU Ophthalmology Corneal Ulcer OCULOPLASTICS AMD DRY WET Pterygium Chalazion/Lesions/Cyst INFLAMMATORY Hole/T ear/Detachment Blepharoplasty DISEASE RETINA Conjunctivitis T. Hess ERM Ocular Rosacea Oculoplastics Diabetic Retinopathy Episcleritis/Scleritis Cataract Surgery Ptosis Macular Edema Uveitis/Iritis Entropion/Ectropion Choroidal Nevus Cellulitis Punctoplasty Retinopexy/Focal/Barrier TESTING /PRP Laser (on site) Visual Field/OCT BOTOX V. Lam Blepharospasm Uveitis, Cataract & DRY EYE MTO Hemifacial Spasm Cornea Surgery Tear Film Analysis Pentacam Topography Hyperhidrosis Lipiflow/IPL OD OS OU Cosmetic/Fillers Tearing/Blocked Duct T. -

Characterizing the Lacrimal Punctum Using Anterior Segment Optical Coherence Tomography
Characterising congenital double punctum anomalies: Clinical, endoscopic and imaging findings Hannah M. Timlin, BSc, FRCOphth,1 Pearse A. Keane, MD, FRCOphth,2 Daniel G. Ezra, MA, MD, FRCOphth1,2 1Lacrimal Clinic, Moorfields Eye Hospital, London, United Kingdom 2NIHR Biomedical Research Centre for Ophthalmology, Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology, UK Financial support: None Correspondence: Hannah M Timlin, Adnexal Office, Moorfields Eye Hospital, 162 City Road, London EC1V2PD Tel: +44(0) 207 253 3411 Fax: +44(0) 20 7566 2334 Email: [email protected] 1 Disclosures; Disclosures; Drs. Keane and Ezra have received a proportion of their funding from the Department of Health’s NIHR Biomedical Research Centre for Ophthalmology at Moorfields Eye Hospital and UCL Institute of Ophthalmology. The views expressed in the publication are those of the authors and not necessarily those of the Department of Health. Dr. Keane has received travel grants from the Allergan European Retina Panel. Dr. Timlin has no conflicts of interest. Running Head: Epiphora with coexistent duplex punctum Precis: Double puncta co-exist with a range of other nasolacrimal pathologies. OCT suggests that the medial of the two double puncta is the abnormal one, with DCG and endoscopy demonstrating a range of accessory canaliculus lengths. Word Count: 2141 Figures: 1 Abbreviations: OCT – optical coherence tomography FDDT - fluorescein dye disappearance test NLDO – nasolacrimal duct obstruction DCG – dacryocystography DCR – dacryocystorhinostomy Keywords: Lacrimal punctum, epiphora, optical coherence tomography, malformation 2 ABSTRACT Purpose: To characterise the anatomical anomaly of congenital double puncta, identify factors contributing to epiphora and its treatment. Methods: Retrospective review of patients presenting with epiphora and a double lacrimal punctum over a 6-month period.