Identification and Clinical Significance of Heart Murmurs in Puppies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Heart Sound Analysis for Diagnosis of Heart Diseases in Newborns
Available online at www.sciencedirect.com ScienceDirect APCBEE Procedia 7 ( 2013 ) 109 – 116 ICBET 2013: May 19-20, 2013, Copenhagen, Denmark Heart Sound Analysis for Diagnosis of Heart Diseases in Newborns Amir Mohammad Amiri*, Giuliano Armano University of Cagliari, Department of Electrical and Electronic Engineering(DIEE), 09123 Cagliari, Italy Abstract Many studies have been conducted in recent years to automatically differentiate normal heart sounds from heart sounds with pathological murmurs using audio signal processing in early stage. Serious cardiac pathology may exist without symptoms. The purpose of this study is developing an automatic heart sound signal analysis system, able to support the physician in the diagnosing of heart murmurs at early stage of life. Heart murmurs are the first signs of heart disease. We screened newborns for normal (innocent) and pathological murmurs. This paper presents an analysis and comparisons of spectrograms after smoothing phonocardiogram signals (PCG) with Cepstrum, Bispectrum, and Wigner Bispectrum techniques. A comparison between these methods has shown that higher order spectra, as Bispectrum and Wigner bispectrum, gave the best results. © 20132013 The Published Authors. Published by Elsevier by Elsevier B.V. B.V.Selection and/or peer review under responsibility of Asia-Pacific Chemical,Selection and Biological peer-review under& Environmental responsibility of EngineeringAsia-Pacific Chemical, Society Biological & Environmental Engineering Society. Keywords: Heart murmurs, Spectral, Cepstrum, Bispectrum, Wigner Bispectrum 1. Introduction Despite remarkable advances in imaging technologies for heart diagnosis, clinical evaluation of cardiac defects by auscultation is still a main diagnostic method for discovering heart disease. In experienced hands, this method is effective, reliable, and cheap. -

How to Recognize a Suspected Cardiac Defect in the Neonate
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcare- professionals/education/continuing-medical-nursing-education/neonatal- nursing-education-briefs/ Cardiac defects are commonly seen and are the leading cause of death in the neonate. Prompt suspicion and recognition of congenital heart defects can improve outcomes. An ECHO is not needed to make a diagnosis. Cardiac defects, congenital heart defects, NICU, cardiac assessment How to Recognize a Suspected Cardiac Defect in the Neonate Purpose and Goal: CNEP # 2092 • Understand the signs of congenital heart defects in the neonate. • Learn to recognize and detect heart defects in the neonate. None of the planners, faculty or content specialists has any conflict of interest or will be presenting any off-label product use. This presentation has no commercial support or sponsorship, nor is it co-sponsored. Requirements for successful completion: • Successfully complete the post-test • Complete the evaluation form Date • December 2018 – December 2020 Learning Objectives • Describe the risk factors for congenital heart defects. • Describe the clinical features of suspected heart defects. • Identify 2 approaches for recognizing congenital heart defects. Introduction • Congenital heart defects may be seen at birth • They are the most common congenital defect • They are the leading cause of neonatal death • Many neonates present with symptoms at birth • Some may present after discharge • Early recognition of CHD -
Congenital Cardiovascular Defects
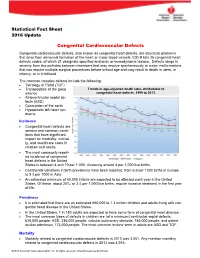
Statistical Fact Sheet 2016 Update Congenital Cardiovascular Defects Congenital cardiovascular defects, also known as congenital heart defects, are structural problems that arise from abnormal formation of the heart or major blood vessels. ICD-9 lists 25 congenital heart defects codes, of which 21 designate specified anatomic or hemodynamic lesions. Defects range in severity from tiny pinholes between chambers that may resolve spontaneously to major malformations that can require multiple surgical procedures before school age and may result in death in utero, in infancy, or in childhood. The common complex defects include the following: Tetralogy of Fallot (TOF) Transposition of the great Trends in age-adjusted death rates attributable to arteries congenital heart defects, 1999 to 2013. Atrioventricular septal de- fects (ASD) Coarctation of the aorta Hypoplastic left heart syn- drome Incidence Congenital heart defects are serious and common condi- tions that have significant impact on morbidity, mortali- ty, and healthcare costs in children and adults. The most commonly report- ed incidence of congenital heart defects in the United States is between 4 and 10 per 1,000, clustering around 8 per 1,000 live births. Continental variations in birth prevalence have been reported, from 6.9 per 1000 births in Europe to 9.3 per 1000 in Asia. An estimated minimum of 40,000 infants are expected to be affected each year in the United States. Of these, about 25%, or 2.4 per 1,000 live births, require invasive treatment in the first year of life. Prevalence It is estimated that there are an estimated 650,000 to 1.3 million children and adults living with con- genital heart disease in the United States. -

Management of Incidentally Detected Heart Murmurs in Dogs and Cats*,**
Journal of Veterinary Cardiology (2015) 17, 245e261 www.elsevier.com/locate/jvc REVIEW Management of incidentally detected heart murmurs in dogs and cats*,** Etienne Coˆte´, DVM a,*, N. Joel Edwards, DVM b, Stephen J. Ettinger, DVM c, Virginia Luis Fuentes, VETMB, PhD d, Kristin A. MacDonald, DVM, PhD e, Brian A. Scansen, DVM, MS f, D. David Sisson, DVM g, Jonathan A. Abbott, DVM h a Department of Companion Animals, Atlantic Veterinary College, University of Prince Edward Island, 550 University Ave., Charlottetown, PE C1A 4P3, Canada b Upstate Veterinary Specialties, 222 Troy Schenectady Rd, Latham, NY 12110, USA c VetCorp Inc, 1736 S. Sepulveda Blvd., Los Angeles, CA 90025, USA d Department of Clinical Sciences and Services, The Royal Veterinary College, University of London, Hawkshead Lane, Hatfield, Herts AL9 7TA, UK e VCA Animal Care Center of Sonoma County, 6470 Redwood Dr, Rohnert Park, CA 94928, USA f Department of Veterinary Clinical Sciences, College of Veterinary Medicine, The Ohio State University, 601 Vernon L Tharp St, Columbus, OH 43210, USA g Department of Small Animal Services, College of Veterinary Medicine, Oregon State University, 700 SW 30th Street, Corvallis, OR 97331, USA h Department of Small Animal Clinical Sciences, Virginia-Maryland Regional College of Veterinary Medicine, 215 Duck Pond Drive, Blacksburg, VA 24061, USA Received 31 March 2015; received in revised form 6 May 2015; accepted 11 May 2015 Prepared by the Working Group of the American College of Veterinary Internal Medicine Specialty of Cardiology on Incidentally Detected Heart Murmurs. * A unique aspect of the Journal of Veterinary Cardiology is the emphasis of additional web-based materials permitting the detailing of procedures and diagnostics. -

Subclinical Subaortic Stenosis in a Golden Retriever
CASE ROUTES h CARDIOLOGY h PEER REVIEWED Subclinical Subaortic Stenosis in a Golden Retriever Kursten Pierce, DVM, DACVIM (Cardiology) Colorado State University THE CASE THE CASE A 12-month-old intact female golden retriever is pre- Diagnostic investigation of the heart murmur via echo- sented for a wellness examination and to discuss the cardiography is discussed with the owner but declined pros and cons of breeding the patient versus pursuing due to the patient’s lack of clinical signs and the costs ovariohysterectomy. The owner would like her to pro- associated with additional testing. duce one litter of puppies prior to being spayed. What are the next steps? On physical examination, the patient is bright, alert, and responsive. She is extremely energetic with a good THE CHOICE IS YOURS … BCS (4/9) and appropriate musculature. Cardiovascu- CASE ROUTE 1 lar examination reveals pink mucous membranes, no To provide information on breeding and caring for a obvious jugular venous distension, and a normal heart pregnant bitch and neonatal puppies and plan to spay rate and rhythm with normal synchronous femoral the patient after the puppies have been weaned, go to pulses. Auscultation is difficult and brief because the page 28. patient is rambunctious and panting. Despite the pant- ing, she is eupneic with clear bronchovesicular sounds. CASE ROUTE 2 A grade II/VI left basilar systolic heart murmur is aus- To avoid providing additional recommendations cultated. A murmur had not previously been docu- regarding breeding and ovariohysterectomy to the mented at her puppy wellness visits. The owner has not owner until a diagnostic investigation with a cardiolo- observed any coughing, trouble breathing, exercise gist has been pursued, go to page 32. -

Congenital Heart Disease Parent FAQ
Congenital Heart Disease Parent FAQ achd.stanfordchildrens.org | achd.stanfordhealthcare.org About Congenital Heart Disease What is congenital heart disease? Congenital heart disease, also called congenital heart defect (CHD), is a heart problem that a baby is born with. When the heart forms in the womb, it develops incorrectly and does not work properly, which changes how the blood flows through the heart. What causes congenital heart defects? In most cases, there is no clear cause. It can be linked to something out of the ordinary happening during gestation, including a viral infection or exposure to environmental factors. Or, it may be linked to a single gene defect or chromosome abnormalities. How common is CHD in the United States among children? Congenital heart defects are the most common birth defects in children in the United States. Approximately 1 in 100 babies are born with a heart defect. What are the most common types of congenital heart defects in children? In general, CHDs disrupt the flow of blood in the heart as it passes to the lungs or to the body. The most common congenital heart defects are abnormalities in the heart valves or a hole between the chambers of the heart (ventricles). Examples include ventricular septal defect (VSD), atrial septal defect (ASD), and bicuspid aortic valve. At the Betty Irene Moore Children’s Heart Center at Stanford Children’s Health, we are known across the nation and world for treating some of the most complex congenital heart defects with outstanding outcomes. Congenital Heart Disease Parent FAQ | 2 Is CHD preventable? In some cases, it could be preventable. -

Pulmonary-Atresia-Mapcas-Pavsdmapcas.Pdf
Normal Heart © 2012 The Children’s Heart Clinic NOTES: Children’s Heart Clinic, P.A., 2530 Chicago Avenue S, Ste 500, Minneapolis, MN 55404 West Metro: 612-813-8800 * East Metro: 651-220-8800 * Toll Free: 1-800-938-0301 * Fax: 612-813-8825 Children’s Minnesota, 2525 Chicago Avenue S, Minneapolis, MN 55404 West Metro: 612-813-6000 * East Metro: 651-220-6000 © 2012 The Children’s Heart Clinic Reviewed March 2019 Pulmonary Atresia, Ventricular Septal Defect and Major Aortopulmonary Collateral Arteries (PA/VSD/MAPCAs) Pulmonary atresia (PA), ventricular septal defect (VSD) and major aortopulmonary collateral arteries (MAPCAs) is a rare type of congenital heart defect, also referred to as Tetralogy of Fallot with PA/MAPCAs. Tetralogy of Fallot (TOF) is the most common cyanotic heart defect and occurs in 5-10% of all children with congenital heart disease. The classic description of TOF includes four cardiac abnormalities: overriding aorta, right ventricular hypertrophy (RVH), large perimembranous ventricular septal defect (VSD), and right ventricular outflow tract obstruction (RVOTO). About 20% of patients with TOF have PA at the infundibular or valvar level, which results in severe right ventricular outflow tract obstruction. PA means that the pulmonary valve is closed and not developed. When PA occurs, blood can not flow through the pulmonary arteries to the lungs. Instead, the child is dependent on a patent ductus arteriosus (PDA) or multiple systemic collateral vessels (MAPCAs) to deliver blood to the lungs for oxygenation. These MAPCAs usually arise from the de- scending aorta and subclavian arteries. Commonly, the pulmonary arteries are abnormal, with hypoplastic (small and underdeveloped) central and branch pulmonary arteries and/ or non-confluent central pulmonary arteries. -

A Robust Heart Sounds Segmentation Module Based on S-Transform Ali Moukadem, Alain Dieterlen, Nicolas Hueber, Christian Brandt
A Robust Heart Sounds Segmentation Module Based on S-Transform Ali Moukadem, Alain Dieterlen, Nicolas Hueber, Christian Brandt To cite this version: Ali Moukadem, Alain Dieterlen, Nicolas Hueber, Christian Brandt. A Robust Heart Sounds Segmen- tation Module Based on S-Transform. Biomedical Signal Processing and Control, Elsevier, 2013, 8 (Issue 3), pp.273-281. 10.1016/j.bspc.2012.11.008. hal-00984327 HAL Id: hal-00984327 https://hal.archives-ouvertes.fr/hal-00984327 Submitted on 28 Apr 2014 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. A Robust Heart Sounds Segmentation Module Based on S-Transform Ali Moukadem1, 3, Alain Dieterlen1, Nicolas Hueber2, Christian Brandt3 1MIPS Laboratory, University of Haute Alsace, 68093 - MULHOUSE CEDEX FRANCE 2 ISL: French-German Research Institute of SAINT-LOUIS, 68300 - SAINT-LOUIS FRANCE 3University Hospital of Strasbourg, CIC, Inserm, BP 426, 67091 STRASBOURG CEDEX FRANCE Abstract This paper presents a new module for heart sounds segmentation based on S-Transform. The heart sounds segmentation process segments the PhonoCardioGram (PCG) signal into four parts: S1 (first heart sound), systole, S2 (second heart sound) and diastole. It can be considered one of the most important phases in the auto-analysis of PCG signals. -

Transcatheter Device Closure of Atrial Septal Defect in Dextrocardia with Situs Inversus Totalis
Case Report Nepalese Heart Journal 2019; Vol 16(1), 51-53 Transcatheter device closure of atrial septal defect in dextrocardia with situs inversus totalis Kiran Prasad Acharya1, Chandra Mani Adhikari1, Aarjan Khanal2, Sachin Dhungel1, Amrit Bogati1, Manish Shrestha3, Deewakar Sharma1 1 Department of Cardiology, Shahid Gangalal National Heart Centre, Kathmandu, Nepal 2 Department of Internal Medicine, Kathmandu Medical College, Kathmandu,Nepal 3 Department of Pediatric Cardiology, Shahid Gangalal National Heart Centre, Kathmandu, Nepal Corresponding Author: Chandra Mani Adhikari Department of Cardiology Shahid Gangalal National Heart Centre Kathmandu, Nepal Email: [email protected] Cite this article as: Acharya K P, Adhikari C M, Khanal A, et al. Transcatheter device closure of atrial septal defect in dextrocardia with situs inversus totalis. Nepalese Heart Journal 2019; Vol 16(1), 51-53 Received date: 17th February 2019 Accepted date: 16th April 2019 Abstract Only few cases of Device closure of atrial septal defect in dextrocardia with situs inversus totalis has been reported previously. We present a case of a 36 years old male, who had secundum type of atrial septal defect in dextrocardia with situs inversus totalis. ASD device closure was successfully done. However, we encountered few technical difficulties in this case which are discussed in this case review. Keywords: atrial septal defect; dextrocardia; transcatheter device closure, DOI: https://doi.org/10.3126/njh.v16i1.23901 Introduction There are only two case reported of closure of secundum An atrial septal defect (ASD) is an opening in the atrial ASD associated in patients with dextrocardia and situs inversus septum, excluding a patent foramen ovale.1 ASD is a common totalis. -

Tetralogy of Fallot.” These Podcasts Are Designed to Give Medical Students an Overview of Key Topics in Pediatrics
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on “Tetralogy of Fallot.” These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio versions are accessible on iTunes or at www.pedcases.com/podcasts. Tetralogy of Fallot Developed by Katie Girgulis, Dr. Andrew Mackie, and Dr. Karen Forbes for PedsCases.com. April 14, 2017 Introduction Hello, my name is Katie Girgulis and I am a medical student at the University of Alberta. This podcast was developed with the help of Dr. Andrew Mackie and Dr. Karen Forbes. Dr. Mackie is a pediatric cardiologist at the Stollery Children’s Hospital, and Dr. Forbes is a pediatrician and medical educator at the Stollery Children’s Hospital. This podcast is about the cardiac condition Tetralogy of Fallot (ToF). For teaching on the general approach to pediatric heart murmurs, please check out the ‘Evaluation of a Heart Murmur’ podcast on Pedscases.com. Slide 2 Learning Objectives By the end of this podcast, the learner will be able to: 1) Recognize the clinical presentations of ToF 2) Describe the four anatomical characteristics of ToF 3) Describe the pathophysiology of the murmur in ToF 4) Formulate initial steps when ToF is suspected 5) Delineate the treatment of hypercyanotic episodes 6) Summarize the definitive treatment for ToF Slide 3 Case – Baby Josh Let’s start with a clinical case: You are working with Dr. Smith, a family physician, during your family medicine rotation. Josh is a 4-month-old infant who is here for a well-baby check. -

Systolic Heart Murmur As First Manifestation of High Output Heart
Arch Cardiol Mex. 2012;82(3):214---217 www.elsevier.com.mx BRIEF REPORT Systolic heart murmur as first manifestation of high output heart failure due to the vein of galen malformation Juan S. Barajas-Gamboa a,b,∗, Julio A. Diaz-Perez b, Yoana Leon-Camargo a, Carlos A. Gonzalez-Gomez a, Cecilia Sandoval-Gomez a a School of Medicine, Autonomous University of Bucaramanga (UNAB), Bucaramanga, Colombia b Department of Medicine, University of California, San Diego, La Jolla CA, USA Received 27 January 2012; accepted 17 April 2012 KEYWORDS Abstract The vein of Galen aneurysmal malformation (VGAM) is an extremely rare arterio- Newborn; venous malformation. The VGAM clinical manifestations vary depending on the magnitude of Vein of Galen vascular compromise and the age at initial presentation. Neonates typically present with severe malformations; congestive heart failure. Here we present a case in which a systolic heart murmur was the first Aneurysm; manifestation of high output heart failure due to a VGAM. Heart Failure; © 2012 Instituto Nacional de Cardiología Ignacio Chávez. Published by Masson Doyma México United States S.A. All rights reserved. of America PALABRAS CLAVE Soplo sistólico como primera manifestación de insuficiencia cardiaca de gasto alto Neonato; secundaria a malformación de la vena de Galeno Malformaciones de la vena de Galeno; Resumen Las malformaciones de la vena cerebral de Galeno (MVG) son extremadamente Aneurisma; raras. Sus manifestaciones clínicas varían dependiendo de la magnitud del compromiso vascular Insuficiencia y la edad inicial de presentación. En neonatos, típicamente se presenta con una insuficiencia Cardiaca; cardiaca congestiva grave. Se presenta un caso en el cual un soplo sistólico cardiaco fue la Estados Unidos primera manifestación de una insuficiencia cardíaca de gasto alto secundaria a una malforma- de América ción aneurismática de la vena de Galeno. -

Congenital Heart Disease: Recognition and Treatment Options – Anna Gelzer
CONGENITAL HEART DISEASE: RECOGNITION AND TREATMENT OPTIONS – ANNA GELZER Prevalence and Frequency Congenital heart disease in dogs: ≤ 1% (Canine clinic population of U Penn 1992) Cats estimated < 0.2% Prevalence likely underestimated (perinatal death, no murmur) Small % of cardiac disease overall, but most common in animals < 1 y old Common congenital cardiac defects in dogs (in the order of frequency): Subaortic stenosis (SAS) Pulmonic stenosis (PS) Patent ductus arteriosus (PDA) Tricuspid valve dysplasia (TVD) Ventricular septal defect (VSD) Tetralogy of Fallot (TOF) Persistent right aortic arch (PRAA) Atrial septal defects (ASD) Mitral valve dysplasia (MVD) Persistent left carnial venal cava Congenital cardiac defects in cats (in the order of frequency): Mitral valve dysplasia (MVD) Ventricular septal defect (VSD) Endocardial cushion defect (ASD+VSD) Patent ductus arteriosus (PDA) Aortic stenosis (SAS) Tetralogy of Fallot (TOF) Pulmonic stenosis (PS) Atrial septal defects (ASD) Tricuspid valve dysplasia (TVD) Physical exam finding in animals with most common congenital heart disease: The simple congenital heart defects are normally identified by the presence of a heart murmur. From the clinical examination, by localizing the heart murmur, identifying its radiation, assessing the precordial impulse and the peripheral pulse, a differential diagnosis list can be drawn up. The table summarizes the findings for some of the common defects identified in dogs and cats. Note, for these simple defects, mucus membrane color is normal (pink).