Mindy Goldman, MD Clinical Professor Dept
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
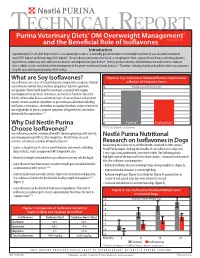
What Are Soy Isoflavones? Figure 2: Soy Isoflavones Reduced Plasma Isoprostanes Soy Isoflavones Are a Class of Natural Bioactive Compounds in Soybeans
TECHNICAL REPORT Purina Veterinary Diets® OM Overweight Management® brand canine dry formula and the Beneficial Role of Isoflavones Introduction Approximately 35% of adult dogs in the U.S. are overweight or obese1. A markedly greater incidence of overweight and obesity was observed in neutered male (59% higher) and female dogs (40% higher)1. Chronic obesity can increase the risk of, or complications from, several chronic diseases including diabetes, hypertension, pulmonary and cardiovascular disease, and degenerative joint disease2. Obesity produces chronic, mild inflammation and increases oxidative stress, which, in turn, contributes to the development of the above-mentioned chronic diseases.3,4 Therefore, reducing obesity and oxidative stress can promote a long life span and improved quality of life in dogs. What are Soy Isoflavones? Figure 2: Soy Isoflavones Reduced Plasma Isoprostanes Soy isoflavones are a class of natural bioactive compounds in soybeans. Natural a Marker of Oxidative Stress soy isoflavones include three chemical compounds: daidzein, genistein, 5 Plasma Isoprostanes (ng/ml) and glycitein. Many health benefits have been associated with regular consumption of soy products. In humans, soy has been found to reduce the 4 risk of cardiovascular disease and certain types of cancer (breast and prostate cancer); relieve a number of problems in post menopausal women including 3 hot flashes, osteoporosis, and decline in cognitive function; reduce cholesterol and triglycerides in plasma; improve symptoms of hypertension; and reduce 2 abdominal fat accumulation.5,6,7 1 Why Did Nestlé Purina 0 Control Isoflavones* Choose Isoflavones? *P<0.01 for Control vs. Isoflavones Soy isoflavones provide a number of benefits for managing dogs with obesity, and reducing rebound effects after weight loss. -

Applications of in Silico Methods to Analyze the Toxicity and Estrogen T Receptor-Mediated Properties of Plant-Derived Phytochemicals ∗ K
Food and Chemical Toxicology 125 (2019) 361–369 Contents lists available at ScienceDirect Food and Chemical Toxicology journal homepage: www.elsevier.com/locate/foodchemtox Applications of in silico methods to analyze the toxicity and estrogen T receptor-mediated properties of plant-derived phytochemicals ∗ K. Kranthi Kumara, P. Yugandharb, B. Uma Devia, T. Siva Kumara, N. Savithrammab, P. Neerajaa, a Department of Zoology, Sri Venkateswara University, Tirupati, 517502, India b Department of Botany, Sri Venkateswara University, Tirupati, 517502, India ARTICLE INFO ABSTRACT Keywords: A myriad of phytochemicals may have potential to lead toxicity and endocrine disruption effects by interfering Phytochemicals with nuclear hormone receptors. In this examination, the toxicity and estrogen receptor−binding abilities of a QSAR modeling set of 2826 phytochemicals were evaluated. The endpoints mutagenicity, carcinogenicity (both CAESAR and ISS Toxicity models), developmental toxicity, skin sensitization and estrogen receptor relative binding affinity (ER_RBA) Nuclear hormone receptor binding were studied using the VEGA QSAR modeling package. Alongside the predictions, models were providing pos- Self−Organizing maps sible information for applicability domains and most similar compounds as similarity sets from their training Clustering and classification schemes sets. This information was subjected to perform the clustering and classification of chemicals using Self−Organizing Maps. The identified clusters and their respective indicators were considered as potential hotspot structures for the specified data set analysis. Molecular screening interpretations of models wereex- hibited accurate predictions. Moreover, the indication sets were defined significant clusters and cluster in- dicators with probable prediction labels (precision). Accordingly, developed QSAR models showed good pre- dictive abilities and robustness, which observed from applicability domains, representation spaces, clustering and classification schemes. -

Daidzein and Genistein Content of Cereals
European Journal of Clinical Nutrition (2002) 56, 961–966 ß 2002 Nature Publishing Group All rights reserved 0954–3007/02 $25.00 www.nature.com/ejcn ORIGINAL COMMUNICATION Daidzein and genistein content of cereals J Liggins1, A Mulligan1,2, S Runswick1 and SA Bingham1,2* 1Medical Research Council Dunn Human Nutrition Unit, Hills Road, Cambridge, UK; and 2European Prospective Investigation of Cancer, University of Cambridge, Cambridge, UK Objective: To analyse 75 cereals and three soy flours commonly eaten in Europe for the phytoestrogens daidzein and genistein. Design: The phytoestrogens daidzein and genistein were extracted from dried foods, and the two isoflavones quantified after hydrolytic removal of any conjugated carbohydrate. Completeness of extraction and any procedural losses of the isoflavones 0 0 were accounted for using synthetic daidzin (7-O-glucosyl-4 -hydroxyisoflavone) and genistin (7-O-glucosyl-4 5-dihydroxyiso- flavone) as internal standards. Setting: Foods from the Cambridge UK area were purchased, prepared for eating, which included cooking if necessary, and freeze dried. Three stock soy flours were also analysed. Results: Eighteen of the foods assayed contained trace or no detectable daidzein or genistein. The soy flours were rich sources, containing 1639 – 2117 mg=kg. The concentration of the two isoflavones in the remaining foods ranged from 33 to 11 873 mg=kg. Conclusion: These analyses will supply useful information to investigators determining the intake of phytoestrogens in cereal products in order to relate intakes to potential biological activities. Sponsorship: This work was supported by the United Kingdom Medical Research Council, Ministry of Agriculture Fisheries and Food (contract FS2034) and the United States of America Army (contract DAMD 17-97-1-7028). -

St. John's Wort 2018
ONLINE SERIES MONOGRAPHS The Scientific Foundation for Herbal Medicinal Products Hyperici herba St. John's Wort 2018 www.escop.com The Scientific Foundation for Herbal Medicinal Products HYPERICI HERBA St. John's Wort 2018 ESCOP Monographs were first published in loose-leaf form progressively from 1996 to 1999 as Fascicules 1-6, each of 10 monographs © ESCOP 1996, 1997, 1999 Second Edition, completely revised and expanded © ESCOP 2003 Second Edition, Supplement 2009 © ESCOP 2009 ONLINE SERIES ISBN 978-1-901964-61-5 Hyperici herba - St. John's Wort © ESCOP 2018 Published by the European Scientific Cooperative on Phytotherapy (ESCOP) Notaries House, Chapel Street, Exeter EX1 1EZ, United Kingdom www.escop.com All rights reserved Except for the purposes of private study, research, criticism or review no part of this text may be reproduced, stored in a retrieval system or transmitted, in any form or by any means, without the written permission of the publisher. Important Note: Medical knowledge is ever-changing. As new research and clinical experience broaden our knowledge, changes in treatment may be required. In their efforts to provide information on the efficacy and safety of herbal drugs and herbal preparations, presented as a substantial overview together with summaries of relevant data, the authors of the material herein have consulted comprehensive sources believed to be reliable. However, in view of the possibility of human error by the authors or publisher of the work herein, or changes in medical knowledge, neither the authors nor the publisher, nor any other party involved in the preparation of this work, warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for results obtained by the use of such information. -

Simultaneous Determination of Daidzein, Genistein and Formononetin in Coffee by Capillary Zone Electrophoresis
separations Article Simultaneous Determination of Daidzein, Genistein and Formononetin in Coffee by Capillary Zone Electrophoresis Feng Luan *, Li Li Tang, Xuan Xuan Chen and Hui Tao Liu College of Chemistry and Chemical Engineering, Yantai University, Yantai 264005, China; [email protected] (L.L.T.); [email protected] (X.X.C.); [email protected] (H.T.L.) * Correspondence: fl[email protected]; Tel.: +86-535-6902063 Academic Editor: Doo Soo Chung Received: 29 October 2016; Accepted: 20 December 2016; Published: 1 January 2017 Abstract: Coffee is a favorite and beverage in Western countries that is consumed daily. In the present study, capillary zone electrophoresis (CE) was applied for the separation and quantification of three isoflavones including daidzein, genistein and formononetin in coffee. Extraction of isoflavones from the coffee sample was carried out by extraction and purification process using ether after the acid hydrolysis with the antioxidant butylated hydroxy-toluene (BHT). The experimental conditions of the CE separation method were: 20 mmol/L Na2HPO4 buffer solution, 25 kV applied voltage, 3 s hydrodynamic injection at 30 mbar, and UV detection at 254 nm. The results show that the three compounds can be tested within 10 min with a linearity of 0.5–50 µg/mL for all three compounds. The limits of detection were 0.0642, 0.134, and 0.0825 µg/mL for daidzein, formononetin and genistein, respectively. The corresponding average recovery was 99.39% (Relative Standard Detection (RSD) = 1.76%), 98.71% (RSD = 2.11%) and 97.37% (RSD = 3.74%). Keywords: capillary zone electrophoresis (CE); daidzein; genistein; formononetin; acid hydrolysis 1. -

Assessment Report on Hypericum Perforatum L., Herba
European Medicines Agency Evaluation of Medicines for Human Use London, 12 November 2009 Doc. Ref.: EMA/HMPC/101303/2008 COMMITTEE ON HERBAL MEDICINAL PRODUCTS (HMPC) ASSESSMENT REPORT ON HYPERICUM PERFORATUM L., HERBA 7 Westferry Circus, Canary Wharf, London, E14 4HB, UK Tel. (44-20) 74 18 84 00 Fax (44-20) 75 23 70 51 E-mail: [email protected] http://www.emea.europa.eu © European Medicines Agency, 2009. Reproduction is authorised provided the source is acknowledged TABLE OF CONTENTS I. REGULATORY STATUS OVERVIEW...................................................................................4 II. ASSESSMENT REPORT............................................................................................................5 II.1 INTRODUCTION..........................................................................................................................6 II.1.1 Description of the herbal substance(s), herbal preparation(s) or combinations thereof 6 II.1.1.1 Herbal substance:........................................................................................................ 6 II.1.1.2 Herbal preparation(s): ................................................................................................ 7 II.1.1.3 Combinations of herbal substance(s) and/or herbal preparation(s)........................... 9 Not applicable. ................................................................................................................................9 II.1.1.4 Vitamin(s) ................................................................................................................... -

Contemporary Approaches for Managing Menopause Symptoms
Menopause 2017 Guidelines: Looking at Special Populations and Building on Existing Practice Patricia Geraghty, MSN, FNP-BC, WHNP Disclosures • Speaker Bureau • AbbVie • Therapeutics MD • Advisory Board • AbbVie (endometriosis) • Sharecare Inc. • Procedure Proctor • Bayer (Contraception) • Off label discussion will be included and identified in this discussion. Objectives • Identify the benefits and risks of estrogen, progesterone, and non-hormonal pharmacological management of menopause symptoms based on dosage, route of administration, pharmacokinetics, treatment population and duration of use. • Develop treatment strategies for special populations including premature ovarian insufficiency, prolonged symptoms, and women who are not candidates for estrogen. • Incorporate the NAMS 2017 Position Statement into patient counseling on the timeline of menopause symptoms and the termination of hormone therapy. Lifespan Lifespan Median 34 322 BC Aristotle describes transition Ages the Through Menopause yr JAMA. JAMA. Investigators. Initiative Health the Women's for Group Writing 2002;288(3):321 - 333. doi:10.1001/jama.288.3.321 Treated with plants s/a 1800’s cohosh, cannabis, opium 1821 French physician DeGardanne 53 lifespan lifespan calls it “Menopause” Adult - 1900’s Deficiency disease 55 1942 Premarin” copyright yr 1960’s “Forever Feminine” by Robert Wilson MD 1980’s-1990’s “Politics of Menopause” by Frances McCrea 2002 WHI- First large randomized control trial “My periods are different. Is This Menopause?” • Random cycling, sometimes early, sometimes late. • Flow variable with prodromal spotting, a long taper, or stopping and starting. • She has a day of very heavy flow. • 77% have duration 10+ days, heavy bleeding 3+ days, spotting 6+ days Paramsothy P, et al. BJOG. 2014 Nov;121(12):1564-73. -

Dietary Supplements Compendium Volume 1
2015 Dietary Supplements Compendium DSC Volume 1 General Notices and Requirements USP–NF General Chapters USP–NF Dietary Supplement Monographs USP–NF Excipient Monographs FCC General Provisions FCC Monographs FCC Identity Standards FCC Appendices Reagents, Indicators, and Solutions Reference Tables DSC217M_DSCVol1_Title_2015-01_V3.indd 1 2/2/15 12:18 PM 2 Notice and Warning Concerning U.S. Patent or Trademark Rights The inclusion in the USP Dietary Supplements Compendium of a monograph on any dietary supplement in respect to which patent or trademark rights may exist shall not be deemed, and is not intended as, a grant of, or authority to exercise, any right or privilege protected by such patent or trademark. All such rights and privileges are vested in the patent or trademark owner, and no other person may exercise the same without express permission, authority, or license secured from such patent or trademark owner. Concerning Use of the USP Dietary Supplements Compendium Attention is called to the fact that USP Dietary Supplements Compendium text is fully copyrighted. Authors and others wishing to use portions of the text should request permission to do so from the Legal Department of the United States Pharmacopeial Convention. Copyright © 2015 The United States Pharmacopeial Convention ISBN: 978-1-936424-41-2 12601 Twinbrook Parkway, Rockville, MD 20852 All rights reserved. DSC Contents iii Contents USP Dietary Supplements Compendium Volume 1 Volume 2 Members . v. Preface . v Mission and Preface . 1 Dietary Supplements Admission Evaluations . 1. General Notices and Requirements . 9 USP Dietary Supplement Verification Program . .205 USP–NF General Chapters . 25 Dietary Supplements Regulatory USP–NF Dietary Supplement Monographs . -

Inhibitory Effect of Genistein and Daidzein on Ovarian Cancer Cell Growth
ANTICANCER RESEARCH 24: 795-800 (2004) Inhibitory Effect of Genistein and Daidzein on Ovarian Cancer Cell Growth CICEK GERCEL-TAYLOR, ANNA K. FEITELSON and DOUGLAS D. TAYLOR Department of Obstetrics, Gynecology and Women’s Health, University of Louisville, School of Medicine, Louisville, KY 40202, U.S.A. Abstract. Background: Survival from ovarian cancer has not Genistein, a soy isoflavanoid, has been intensely studied changed significantly in the past twenty years requiring in relation to breast cancer. Interest first arose upon development of additional treatment protocols. We studied the discovery of the vast difference in breast cancer rates in effect of genistein and daidzein on ovarian cancer cell growth. Asia versus Western countries (1). Large dietary differences Materials and Methods: Five ovarian cancer cell lines from Stage exist, especially in genistein consumption, as the average IIIC disease were evaluated. Sulforhodamine B and colony Asian intake is 20-80 mg/day whereas the average US intake formation assays were used to analyze growth inhibitory effects of is only 1-3 mg (2,3) The dietary and disease discrepancy genistein and daidzein alone and with cisplatin, paclitaxel or prompted further study into the chemopreventive and topotecan. Apoptosis induction was studied by determining potentially therapeutic properties of genistein. caspase-3 activity. Results: Inhibition of growth (50-80%), colony Genistein has been found to inhibit cell proliferation, formation and colony size was seen at 144 Ìm of genistein, 0-23% oncogenesis and clonogenic ability in animal and human reduction was demonstrated at 9 Ìm. At 144 Ìm, the colony size cells (3-5). Several studies have been performed to evaluate was inhibited >75%; at 9 Ìm 4/5 cell lines had >50% reduction. -

Daidzein and Breast Cancer Risk in Later Years FACT SHEET on the PHYTOESTROGEN DAIDZEIN
BREAST CANCER & THE ENVIRONMENT RESEARCH CENTERS Early Life Exposure to the Phytoestrogen Daidzein and Breast Cancer Risk in Later Years FACT SHEET on the PHYTOESTROGEN DAIDZEIN Abstract Daidzein is a phytoestrogen (estrogen-like chemical compound present in plants) that binds to estrogen receptors and has both weak estrogenic and weak anti-estrogenic effects. There are three major classes of phytoestrogens that have estrogen-like actions in the human body. They are lignans, isoflavones, and coumestans. Daidzein is an isoflavone. Exposure to daidzein occurs principally through foods made with soybeans and soy protein. In a proportion of the population, daidzein is metabolized by intestinal bacteria to produce equol and O-DMA, metabolites that are more estrogenic than daidzein. Daidzein can cross the placenta and has been found in breast milk. It is unknown whether daidzein influences early onset of puberty in girls. Exposure to daidzein can be measured using a blood or urine test; however levels vary widely in each person due to considerable variability in the metabolism of daidzein. In vitro and in vivo studies have found that daidzein stimulates the growth of estrogen-sensitive breast cancer cells. Epidemiologic studies have found conflicting evidence; some studies have found an association between soy exposure and decreased breast cancer risk while others have found no association. Some epidemiological evidence indicates that soy intake may be more protective when the exposure occurs prior to puberty. More research needs to be conducted on the association between breast cancer risk and daidzein specifically before conclusions can be drawn. The International Agency for Research on Cancer (IARC) has not determined whether phytoestrogens are carcinogenic to humans. -

Dr. Duke's Phytochemical and Ethnobotanical Databases List of Chemicals for Dry Mouth / Xerostomia
Dr. Duke's Phytochemical and Ethnobotanical Databases List of Chemicals for Dry Mouth / Xerostomia Chemical Activity Count (+)-CATECHIN 2 (+)-EPIPINORESINOL 1 (-)-ANABASINE 1 (-)-EPICATECHIN 2 (-)-EPIGALLOCATECHIN 2 (-)-EPIGALLOCATECHIN-GALLATE 2 (Z)-1,3-BIS(4-HYDROXYPHENYL)-1,4-PENTADIENE 1 1,8-CINEOLE 2 10-METHOXYCAMPTOTHECIN 1 16-HYDROXY-4,4,10,13-TETRAMETHYL-17-(4-METHYL-PENTYL)-HEXADECAHYDRO- 1 CYCLOPENTA[A]PHENANTHREN-3-ONE 2,3-DIHYDROXYBENZOIC-ACID 1 3'-O-METHYL-CATECHIN 1 3-ACETYLACONITINE 1 3-O-METHYL-(+)-CATECHIN 1 4-O-METHYL-GLUCURONOXYLAN 1 5,7-DIHYDROXY-2-METHYLCHROMONE-8-C-BETA-GLUCOPYRANOSIDE 1 5-HYDROXYTRYPTAMINE 1 5-HYDROXYTRYPTOPHAN 1 6-METHOXY-BENZOLINONE 1 ACEMANNAN 1 ACETYL-CHOLINE 1 ACONITINE 2 ADENOSINE 2 AFFINISINE 1 AGRIMONIIN 1 ALANTOLACTONE 2 ALKANNIN 1 Chemical Activity Count ALLANTOIN 1 ALLICIN 2 ALLIIN 2 ALLOISOPTEROPODINE 1 ALLOPTEROPODINE 1 ALLOPURINOL 1 ALPHA-LINOLENIC-ACID 1 ALPHA-TERPINEOL 1 ALPHA-TOCOPHEROL 2 AMAROGENTIN 1 AMELLIN 1 ANABASINE 1 ANDROMEDOTOXIN 1 ANETHOLE 1 ANTHOCYANIDINS 1 ANTHOCYANINS 1 ANTHOCYANOSIDE 1 APIGENIN 1 APOMORPHINE 1 ARABINO-3,6-GALACTAN-PROTEIN 1 ARABINOGALACTAN 1 ARACHIDONIC-ACID 1 ARCTIGENIN 2 ARECOLINE 1 ARGLABRIN 1 ARISTOLOCHIC-ACID 1 ARISTOLOCHIC-ACID-I 1 2 Chemical Activity Count ARMILLARIEN-A 1 ARTEMISININ 1 ASCORBIC-ACID 4 ASTRAGALAN-I 1 ASTRAGALAN-II 1 ASTRAGALAN-III 1 ASTRAGALIN 1 AURICULOSIDE 1 BAICALEIN 1 BAICALIN 1 BAKUCHIOL 1 BENZALDEHYDE 1 BERBAMINE 1 BERBERASTINE 3 BERBERINE 3 BERBERINE-CHLORIDE 1 BERBERINE-IODIDE 1 BERBERINE-SULFATE 1 BETA-AMYRIN-PALMITATE -

Pharmacology and Therapeutic Potential of Sigma1 Receptor Ligands E.J
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by PubMed Central 344 Current Neuropharmacology, 2008, 6, 344-366 Pharmacology and Therapeutic Potential of Sigma1 Receptor Ligands E.J. Cobos1,2, J.M. Entrena1, F.R. Nieto1, C.M. Cendán1 and E. Del Pozo1,* 1Department of Pharmacology and Institute of Neuroscience, Faculty of Medicine, and 2Biomedical Research Center, University of Granada, Granada, Spain Abstract: Sigma () receptors, initially described as a subtype of opioid receptors, are now considered unique receptors. Pharmacological studies have distinguished two types of receptors, termed 1 and 2. Of these two subtypes, the 1 re- ceptor has been cloned in humans and rodents, and its amino acid sequence shows no homology with other mammalian proteins. Several psychoactive drugs show high to moderate affinity for 1 receptors, including the antipsychotic haloperi- dol, the antidepressant drugs fluvoxamine and sertraline, and the psychostimulants cocaine and methamphetamine; in ad- dition, the anticonvulsant drug phenytoin allosterically modulates 1 receptors. Certain neurosteroids are known to interact with 1 receptors, and have been proposed to be their endogenous ligands. These receptors are located in the plasma membrane and in subcellular membranes, particularly in the endoplasmic reticulum, where they play a modulatory role in 2+ intracellular Ca signaling. Sigma1 receptors also play a modulatory role in the activity of some ion channels and in sev- eral neurotransmitter systems, mainly in glutamatergic neurotransmission. In accordance with their widespread modula- tory role, 1 receptor ligands have been proposed to be useful in several therapeutic fields such as amnesic and cognitive deficits, depression and anxiety, schizophrenia, analgesia, and against some effects of drugs of abuse (such as cocaine and methamphetamine).