University Application Packet for Psychology and Psychiatric Rehabilitation Dual Major
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

To View the Dawg Print June 2021
Vol. LXXXXVIIII Jonathan Dayton High School June 2021 Senior Edition Class of 2021 EDITORIAL BOARD Brielle & Nicole Ramundo Ms. Rooney-Kuhn Sarah Zarember Editors in Chief Advisor Opinions Editor CONGRATULATIONS TO THE CLASS OF 2021! THE DAWG PRINT WISHES EVERYONE THE BEST OF LUCK IN THEIR FUTURE AND WE ARE EXCITED TO SEE WHAT EVERYONE ACCOMPLISHES. HAVE A GREAT SUMMER! The Dawg Print Class of 2021 3 CLASS OF 2021 Compiled by Brielle Ramundo, 2021 and Sarah Zarember, 2021 Ali Abouzeid Kai Cobbs- Rutgers University Zach Abramovitz- The Ohio State University Ethan Coelho Isabella Ahrens- Cosmetology School Elsie Cohen- Gap Year in Israel, The New School Babatunde Ajayi- Cornell University Rose Coleman- Union County College Anaziah Alexander Ciara Corbett- The College of New Jersey Anthony Apicella- Gettysburg University Anthony Corigliano- Kean University Zoe Araw Ana Craciun- Rutgers University David Ares- Penn State University Makhi Cromartie David Arias- Army Juan Cruz Marios Aristodemou- Seton Hall University John Cunha AJ Armah- Montclair State University Mark Cunningham- University of Tampa Maiya Barnhardt- Howard University Joey Czepurko- Gap Year Emma Barone- Marywood University Kolby Dagner- Iona College Sarivelle Bento- Rutgers University Jeremy Dash- Syracuse University Jordan Berkowitz- University of Delaware Laila Davis- Allegheny College Ava Bertolotti- Northeastern University Luigi Del Mauro- Monmouth University Timothy Burns Ryan Disko- University of Delaware Gina Carrera- New Jersey Institute of Technology Jenna Dordoni- -

Section Iii-A
Section III-E Seven Year Capital Improvement Plan SECTION III-E SEVEN-YEAR CAPITAL IMPROVEMENT PLAN FISCAL 2009 – 2015 New Jersey City University Kean University William Paterson University Montclair State University The College of New Jersey Ramapo College of New Jersey The Richard Stockton College of New Jersey Section III-E, Page 437 Section III-E Seven Year Capital Improvement Plan HIGHER EDUCATION Overview The New Jersey system of higher education is committed to enabling all people to achieve their maximum potential, fostering democratic principles, improving the quality of life, and supporting the State's success in a global economy. By placing teaching and learning at the core of its mission, the higher education system in New Jersey prepares individuals for fulfilling lives, rewarding careers, and lifelong learning; through research, colleges and universities enhance teaching and learning, increase knowledge, improve the human condition, and enhance the economy. Many institutions also provide community service, work with local schools and organizations, sponsor recreational and cultural events, and offer technical assistance to small businesses. In addition to promoting personal and intellectual growth, the higher education system bestows economic benefits to the State. By providing an educated and skilled workforce, developing new technologies through research, and devising new partnerships with private enterprise, the system attracts new businesses, creates jobs, and promotes economic growth. New Jersey has more scientists and engineers per capita than any other state and is an international leader in corporate research and development. Overall, the State has a higher than average number of executives, administrators and managers, and a lower than average concentration of workers in service occupations. -

VIRTUAL ASPIRE 2021 Building Success Through the Liberal Arts Building Success Through the Liberal Arts
COLLEGE OF ARTS, HUMANITIES, AND SOCIAL SCIENCES UNIVERSITY PRESENTS VIRTUAL ASPIRE 2021 Building Success Through the Liberal Arts Building Success through the Liberal Arts Vision Statement The goal of the Aspire program is to empower students to appreciate, articulate, and leverage the intellectual skills, knowledge, and dispositions unique to a liberal arts education in the service of their personal and professional development. Participants will learn to convey the core values and strengths of their degree program, identify career paths that may connect to that program, and prepare themselves to fur- ther pursue passions and opportunities upon completing their degrees. Thank you to Boston College, Endeavor: The Liberal Arts Advantage for Sophomores, for inspiration and activity ideas. 2 Contents Schedule Overview 4-5 CoAHSS 6-9 Dean’s Advisory Board 10-21 Connect with Us! Guest Speakers 22-24 Campus Resources 25-26 @WPCOAHSS Thank You 27 “What we think, we become.” -Buddha 3 Schedule Overview In-Person Evening Program: Monday, August 2nd Student Center. Rm. 211 5:30pm-6:30pm: Welcome: Program Overview/Introduction: Speakers: o Dr. Wartyna Davis, Dean, College of Arts, Humanities, and Social Science o Dr. Joshua Powers, Provost and Senior Vice President, William Paterson University o Valerie Gross, Dean’s Advisory Board Chair o Selected Student from Aspire 2020, Zhakier Seville Reception: Light Refreshments VIRTUAL Day One Tuesday, August 3th from 9:00am to 2:35pm 9:00– 9:05am Welcome: Dr. Ian Marshall and Lauren Agnew 9:05am-10:00am Virtual Workshops: Career Foundations Group A: The Liberal Arts Advantage: Understanding Yourself through the Strong Interest Inventory Assessment with Ms. -
Kean Program W.Map -.Pdf
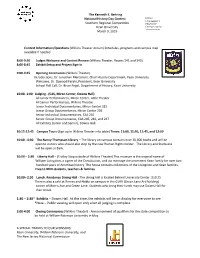
The Kenneth E. Behring National History Day Contest Kean University Southern Regional Competition History Kean University Department Townsend March 9, 2019 Contest Information/Questions (Wilkins Theater Atrium) Schedules, programs and campus map available if needed 8:00-9:30 Judges Welcome and Contest Review (Wilkins Theater, Rooms 141 and 143) 8:00-8:45 Exhibit Setup and Project Sign-In (Wilkins Theater). 9:00-9:45 Opening Ceremonies Introductions, Dr. Jonathan Mercantini, Chair History Department, Kean University Welcome, Dr. Dawood Farahi, President, Kean University School Roll Call, Dr. Brian Regal, Department of History, Kean University 10:00- 1:00 Judging - (CAS, Miron Center, Downs Hall) All Junior Performances, Miron Center, Little Theater All Senior Performances, Wilkins Theatre Junior Individual Documentaries, Miron Center 315 Junior Group Documentaries, Miron Center 226 Senior Individual Documentaries, CAS 235 Senior Group Documentaries, CAS 245, 246, and 247 All Exhibits (Junior and Senior), Downs Hall 10:15-12:45 Campus Tours (Sign up in Wilkins Theater info table) Times: 11:00, 11:30, 11:45, and 12:00 10:00 - 4:30 The Nancy Thompson Library – The library on campus contains over 30,000 books and will be open to visitors who should also stop by the new Human Rights Center. The Library and Starbucks will be open at 8am. 10:00 – 2:30 Liberty Hall – (Trolley Stop outside of Wilkins Theater) This museum is the original home of William Livingston, a signer of the Constitution, and via marriage the prominent Kean family for over two hundred years of American history. The house contains collections of the Livingston and Kean families. -

College Acceptances & Scholarships 2016-2017
COLLEGE ACCEPTANCES & SCHOLARSHIPS 2016-2017 Last Name First Name College State Scholarship Adams Victoria American University DC Drew University NJ $70,000.00 Loyola University MD Saint Joseph's University PA $52,000.00 Seton Hall University NJ $36,500.00 The College of New Jersey NJ University of Tampa FL $24,000.00 Aleta Nicole Drexel University PA Georgian Court University NJ $56,000.00 Ramapo College NJ Alves Justin Mount St. Mary's University MD $96,000.00 Ocean County College NJ Asanza Jackson Coastal Carolina University SC Drexel University PA $58,800.00 Monmouth University NJ $44,000.00 Penn State University PA $16,000.00 Saint Joseph's University PA $52,000.00 Seton Hall University NJ $62,500.00 Baguio Jade Arcadia University PA $78,000.00 Elizabethtown College PA $108,000.00 Lebanon Valley College PA $92,000.00 Sacred Heart University CT $40,000.00 Seton Hall University NJ $82,500.00 Widener University PA $106,000.00 Baltus Matas Monmouth University NJ Seton Hall University NJ Banias Cole Christopher Newport University VA $20,000.00 Fordham University NY $50,000.00 Monmouth University NJ $64,000.00 Roger Williams University RI $70,000.00 Sacred Heart University CT $64,000.00 Salve Regina University RI $88,000.00 Seton Hall University NJ $106,500.00 Baptista Kyle Ocean County College NJ Bidwell Nicholas Syracuse University NY University of Arizona AZ $32,000.00 Brosius Mario Ocean County College NJ Brown Katherine Caldwell University NJ College of Mount Saint Vincent NY $96,000.00 Georgian Court University NJ $68,000.00 Seton Hall University NJ $92,500.00 Wagner College NY $80,000.00 Bruinooge Matthew Brown University RI $166,720.00 Calvetto Hunter Georgian Court University NJ $72,000.00 Mount St. -

Sure System Documentation ______
SURE SYSTEM DOCUMENTATION ___________________________________________________________________ DATA DICTIONARY FOR NEW TRANSFER ENROLLMENT DATA SUBMISSIONS JULY 2008 OFFICE OF RESEARCH NEW JERSEY COMMISSION ON HIGHER EDUCATION TABLE OF CONTENTS NAME POSITION LENGTH DATA ELEMENT DESCRIPTION ---- -------- ------ --------------------------------- T01 01-06 6 Reporting Date (Month/Year) T02 07-12 6 Institution (CEEB Code) T03 13-21 9 Social Security Number T04 22 1 Class Level T05 23-28 6 Program Major (CIP Code) T06 29 1 Baccalaureate Degree Program T07 30-35 6 Transfer Institution (CEEB Code) T08 36 1 Associate Degree from NJ Comm. Col. T09 37-41 5 Degree Credits Awarded by Transfer Inst. T10 42-46 5 Degree Credits Accepted from Trans. Ins. NOTE: This data is to be reported by New Jersey Senior Public Institutions for all new undergraduate transfer students from New Jersey Community Colleges. If a student has multiple transfer institutions, list them as separate records in the file. This data is needed to fulfill reporting requirements under NJ Chapter 175 c.18a:62-49. SURE NEW TRANSFER ENROLLMENT DATA DICTIONARY – JULY 2008 -- PAGE 2 DATA ELEMENT (T01) REPORTING DATE ----------------------------------- DEFINITION: THE POINT IN TIME FOR WHICH DATA ARE REPORTED. LOCATION: 01 - 06 CODING: 6 DIGITS: THE FIRST AND SECOND DIGITS ARE THE MONTH THE SEMESTER BEGAN; THE THIRD THROUGH SIXTH DIGITS ARE THE CALENDAR YEAR. FIRST AND SECOND DIGITS ----------------------- 01 = JANUARY (OPENING SPRING SEMESTER) 09 = SEPTEMBER (OPENING FALL SEMESTER) THIRD THROUGH SIXTH DIGITS -------------------------- 2008 = 2008 2009 = 2009 2010 = 2010 ETC. EXAMPLES OF REPORTING PERIODS ----------------------------- 092008 = OPENING FALL, 2008 012009 = OPENING SPRING, 2009 092010 = OPENING FALL, 2010 SURE NEW TRANSFER ENROLLMENT DATA DICTIONARY -- JULY 2008 -- PAGE 3 DATA ELEMENT (T02) INSTITUTION (CEEB) CODE -------------------------------------------- DEFINITION: A NUMBER ASSIGNED TO AN EDUCATION INSTITUTION BY THE COLLEGE ENTRANCE EXAMINATION BOARD (CEEB). -
Masters Child Welfare Education Program 2017-18 Annual Report
MCWEP MASTERS CHILD WELFARE EDUCATION PROGRAM 2017-18 ANNUAL REPORT LESSONS LEARNED AND RECOMMENDATIONS FOR PROGRAM ENHANCEMENT DIANE S. FALK, PH.D., MSW CO-PRINCIPAL INVESTIGATOR CHILD WELFARE EDUCATION INSTITUTE JOSEPH EVERETT, MSW DAWN KONRADY, ED.D., MBA, MA PROGRAM COORDINATOR, CHILD WELFARE EDUCATION INSTITUTE DIRECTOR AND CO-PRINCIPAL INVESTIGATOR CHILD WELFARE EDUCATION INSTITUTE MCWEP ANNUAL REPORT 2017 - 2018 Child Welfare Education Institute Staff LESSONS LEARNED AND RECOMMENDATIONS FOR ONGOING PROGRAM ENHANCEMENT Diane S. Falk, Ph.D., MSW Co-Principal Investigator, Child Welfare Education Institute Dawn Konrady, Ed.D., MBA, MA Director and Co-Principal Investigator, Child Welfare Education Institute Joseph Everett, MSW Program Coordinator, Child Welfare Education Institute Robin Hernandez-Mekonnen, Ph.D., MSW Faculty & Learning Community Coordinator, MCWEP Maya Lewis, Ph.D., MSW Faculty & Learning Community Coordinator, MCWEP 2 MCWEP ANNUAL REPORT 2017 - 2018 ACKNOWLEDGMENTS The authors are grateful for the cooperation of the students who took the time to give feedback on their experiences with the Masters Child Welfare Education Program (MCWEP). Without their input, this report would not have been possible. We would also like to thank our MCWEP partners, including the Graduate Program Academic Coordinators, faculty, and staff at Kean University, Monmouth University, Rutgers University and Stockton University. Additionally, the support received from the New Jersey Department of Children and Families, the Division of Child Protection and Permanency (DCP&P), the Office of Training and Professional Development, and the New Jersey Chapter of the National Association of Social Workers has been essential for the ongoing success of this project. The Masters Child Welfare Education Program especially thanks Christine Norbut Beyer, MSW, Commissioner of the New Jersey Department of Children and Families, for her ongoing support of efforts to improve the lives of New Jersey families through education and training of the workforce. -

MONTCLAIR STATE UNIVERSITY Montclair, New Jersey BOARD OF
MONTCLAIR STATE UNIVERSITY Montclair, New Jersey BOARD OF TRUSTEES July 27, 2017 Present: Ms. Rose Cali, Dr. Susan Cole, Mr. Hasani Council, Dr. Francis Cuss, Mr. Jean Marc de Grandpre, Mr. George J. Hiltzik, Mr. Douglas Kennedy, Mr. George Koutsouradis, Mr. John McGoldrick, Mr. William Mullen, and Mr. Kent Slutyer Absent: Ms. Mary Comito, Mr. Lawrence Inserra, Mr. Ralph LaRossa, Mr. Tom Maguire, and Mr. Preston Pinkett Present by invitation: Mr. Shawn Connolly, Ms. Candace Fleming, Hon. Mark Fleming, Ms. Shivaun Gaines, Dr. Karen Pennington, Mr. Jon Rosenhein, Mr. Jack Shannon, Dr. Ken Sumner, Ms. Junea Williams-Edmund, Ms. Maria C. Anderson, and Mr. Keith Barrack Mr. Hiltzik called the meeting to order in the School of Communication, 1th Floor Presentation Hall, at 11:15 a.m. Statement regarding manner of public notice of meeting Mr. Hiltzik read the following statement regarding the public notice of the meeting: “Please be advised that in compliance with the requirements of the Open Public Meetings Act, adequate notice of this meeting — July 27, 2017— has been provided by distributing notices as required, properly posting 48- hour notice, and forwarding notices to designated newspapers and to persons requesting such notification.” Oath of Office Mark Fleming, Esq. swore in George Koutsouradis as the non-voting student trustee. Roll call — As reported above. Minutes from the meeting of June 8, 2017 Trustees approved the minutes from June 8, 2017 as distributed. No. 3113 Union Report Professor Wolfson spoke on behalf of AFT Local 1904. Professor Wolfson reported that there is a tentative agreement between the Union and the State of New Jersey, and the Union is pleased that the negotiations are completed. -

Music Student Wins Competition “Some of the Ideas We’Ve Talked About Are Student and Faculty Housing, As Well As by Raquel Fernandes Eugene J
runningback dawn & Lisa With change dish out the big read P. 3 advice P. 6 FALL FASHION of heart P. 15 SPECIAL The Tower see page 5 www.kean.edu/~thetower Kean University’s stUDENT NEWSPAPER Volume 10 • Issue 2 Oct. 21-Nov. 17, 2009 Transforming Morris Avenue? Kean University and Elizabeth Look at New Ideas BY JOSEPH TINGLE prise zone,” which the state designates to promote growth and private investment Kean University President Dawood through special tax breaks and other pro- Farahi and Chris Bollwage, mayor of the grams. Jersey Gardens Mall is in an urban city of Elizabeth, have a plan for Morris enterprise zone. Avenue that would permanently change “[The plan] would need to be a private- the atmosphere of Kean University and public partnership,” Bollwage said, and parts of its neighboring city. “will not work with [only] government The plan, which was announced briefly money.” by Dr. Farahi at a welcoming address to faculty and students last month, would create a student-centered “walking path” Photo: Ana Maria Silverman which would stretch from the intersection Chapolera Latin Musical Festival (See centerfold, pgs 8-9.) between Morris Avenue and North Avenue to the Elizabeth train station, and attract private investment to Kean and the city of Elizabeth, according to Bollwage. Music Student Wins Competition “Some of the ideas we’ve talked about are student and faculty housing, as well as BY RAQUEL FERNANDES Eugene J. Cornacchia and Dr. YiLi Lin, other businesses that are minimal to Kean the symphony’s conductor, signed a for- University, like bookstores and clothing Kean University music student Kenny mal agreement. -

Kean Viewbook
U N I V ERS I T Y CougarsUNIVERSITY Climb HIGHER Minutes from Manhattan Metro NYC Study business, public administration, liberal Not sure what you want to do? We get it. arts and humanities, or the sciences. Whether Our faculty advisors are here to help you find you want to be a global executive, architect, your path. We believe every student has a KEAN designer, teacher or medical professional, special gift, and it is our job to bring it out you gain the knowledge, skills and confidence and nourish it. to build a career and a fulfilling life at Kean COUGARS CLIMB (pronounced “cane”). Kean students graduate with research skills to pursue an advanced degree and practical You learn in small classes from faculty who skills to excel in the New York metro job are nationally recognized scholars in their market and beyond. fields and dedicated to providing you with HIGHER real-world experience. Our faculty conduct The heights you reach are up to you. research with STEM students, build national branding campaigns with design students Kean University offers a public, world-class education in the and work with business students on projects New York metro area with more than 50 undergraduate majors for multinational corporations. and 60 graduate programs designed to help you climb higher. You determine the path. Kean has 16,000 students at 3 campuses in New Jersey and Prof. Patricia Morreale was recently named U.S. News & World Report named a campus in Wenzhou, China. a fellow of the American Association for the Kean’s Occupational Therapy program Advancement of Science for bringing more one of the best in the nation. -
MASTERS CHILD WELFARE EDUCATION PROGRAM Masters Child Welfare Education Program (MCWEP) ABOUT the PROGRAM
MCWEP MASTERS CHILD WELFARE EDUCATION PROGRAM Masters Child Welfare Education Program (MCWEP) ABOUT THE PROGRAM The Masters Child Welfare Education Program (MCWEP) is a partnership among the New Jersey Department of Children and Families and a consortium of four New Jersey MSW programs—Kean University, Monmouth University, Rutgers University, and Stockton University - the lead institution. Its purpose is to offer current Division of Child Protection and Permanency supervisors the opportunity to strengthen their skills in clinical social work practice and supervision, obtain an advanced credential in social work (MSW), and ultimately to enhance the capacity of the Division to deliver the highest quality services to the vulnerable children and families that it serves. DCF will provide tuition and fees for applicants accepted into MCWEP. MCWEP Program Structure: The program consists of three components: 1. Enrollment in one of four New Jersey part-time MSW programs* o Traditional MSW Program, for individuals with a bachelor’s degree with a major other than social work • Requires 60 credits of coursework, including 900-1125 hours of supervised field experience in an approved agency or institution o Advanced Standing MSW Program, for selected individuals who have completed a degree with a major in social work • Requires 30-39 credits of coursework, including 500-885 hours of supervised field experience in an approved agency or institution 2. Participation in the MCWEP Learning Community o Consisting of online discussions and quarterly face-to-face -

Paterson Public Schools High School Seniors Earn $9.4 Million in Scholarships
FOR IMMEDIATE RELEASE Contact: Paul Brubaker June 20, 2019 973-518-2298 PATERSON PUBLIC SCHOOLS HIGH SCHOOL SENIORS EARN $9.4 MILLION IN SCHOLARSHIPS Scholarship total only includes awards based on student merit PATERSON – Paterson Public Schools officials reported today that 1,022 students have been accepted to college. Collectively, those students have been awarded $9,430,490 in scholarships, based on data provided by the district’s 12 high schools. This funding total does not include monies that would be made available to students based on their families’ economic eligibility, such as the Pell Grant. “These numbers are strong indicators of how well the district is working with students and families,” said Schools Superintendent Eileen F. Shafer. “I want to congratulate all of the students who have been accepted into college and have been awarded scholarships based on their hard work. I also want to thank all of the parents who have supported their academic achievements at home, as well as all of the teachers, administrators, guidance counselors and principals who have done everything they can to help prepare our students for college.” What follows is a school-by-school representation of the number of students accepted into college, the colleges where the students were accepted, and the total amount of scholarship dollars awarded to students at that school. PANTHER Academy Total Students Accepted Colleges (34) Total Scholarship Dollars 39 Passaic County Community College $2,558,174 Fairleigh Dickenson University New Jersey City University