Standards Presentation to California Occupational Safety and Health Standards Board
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Effect of Contingent Music with Physical Therapy in Children Who Toe- Walk Penny Roberts
Florida State University Libraries Electronic Theses, Treatises and Dissertations The Graduate School 2002 The Effect of Contingent Music with Physical Therapy in Children Who Toe- Walk Penny Roberts Follow this and additional works at the FSU Digital Library. For more information, please contact [email protected] THE FLORIDA STATE UNIVERSITY COLLEGE OF MUSIC THE EFFECT OF CONTINGENT MUSIC WITH PHYSICAL THERAPY IN CHILDREN WHO TOE-WALK By PENNY ROBERTS A Thesis submitted to the School of Music in partial fulfillment of the Requirements for the degree of Master of Music Degree Awarded: Fall Semester, 2002 The members of the Committee approve the thesis of Penny Roberts defended on November 8, 2002. ________________________ Jayne M. Standley Professor Directing Thesis ________________________ Clifford K. Madsen Committee Member ________________________ Diane Gregory Committee Member ACKNOWLEDGEMENTS I greatly appreciate Dr. Jayne Standley for her advice, patience, and gentle prodding during this experience. I sincerely thank the Physical Therapists who allowed me access to their patients, and patiently answered my many questions: E.A., V. C., M. M., S. M., & C. S. Thank you also to the facilities for your cooperation. Thank you to those friends who listened to thesis talk almost every day. You know who you are. Many thanks to Kate & Scott for their superior accommodations, computer assistance, and general support. I very much appreciate Claudine Boussicaut’s time. Most importantly, thank you to Zac, who now knows more about toe-walking and -

Symantec Web Security Service Policy Guide
Web Security Service Policy Guide Revision: NOV.07.2020 Symantec Web Security Service/Page 2 Policy Guide/Page 3 Copyrights Broadcom, the pulse logo, Connecting everything, and Symantec are among the trademarks of Broadcom. The term “Broadcom” refers to Broadcom Inc. and/or its subsidiaries. Copyright © 2020 Broadcom. All Rights Reserved. The term “Broadcom” refers to Broadcom Inc. and/or its subsidiaries. For more information, please visit www.broadcom.com. Broadcom reserves the right to make changes without further notice to any products or data herein to improve reliability, function, or design. Information furnished by Broadcom is believed to be accurate and reliable. However, Broadcom does not assume any liability arising out of the application or use of this information, nor the application or use of any product or circuit described herein, neither does it convey any license under its patent rights nor the rights of others. Policy Guide/Page 4 Symantec WSS Policy Guide The Symantec Web Security Service solutions provide real-time protection against web-borne threats. As a cloud-based product, the Web Security Service leverages Symantec's proven security technology, including the WebPulse™ cloud community. With extensive web application controls and detailed reporting features, IT administrators can use the Web Security Service to create and enforce granular policies that are applied to all covered users, including fixed locations and roaming users. If the WSS is the body, then the policy engine is the brain. While the WSS by default provides malware protection (blocks four categories: Phishing, Proxy Avoidance, Spyware Effects/Privacy Concerns, and Spyware/Malware Sources), the additional policy rules and options you create dictate exactly what content your employees can and cannot access—from global allows/denials to individual users at specific times from specific locations. -

Release Notes Micro Focus the Lawn 22-30 Old Bath Road Newbury, Berkshire RG14 1QN UK
Micro Focus Visual COBOL 2.3 for ISVs Release Notes Micro Focus The Lawn 22-30 Old Bath Road Newbury, Berkshire RG14 1QN UK http://www.microfocus.com Copyright © Micro Focus 2009-2015. All rights reserved. MICRO FOCUS, the Micro Focus logo and Visual COBOL are trademarks or registered trademarks of Micro Focus IP Development Limited or its subsidiaries or affiliated companies in the United States, United Kingdom and other countries. All other marks are the property of their respective owners. 2015-11-09 ii Contents Micro Focus Visual COBOL 2.3 for ISVs Release Notes .................................5 System Requirements ........................................................................................6 System Requirements for Visual COBOL for Visual Studio ................................................ 6 Hardware Requirements .......................................................................................... 6 Operating Systems Supported ................................................................................. 6 Software Requirements ............................................................................................6 System Requirements for Visual COBOL for Eclipse (Windows) ........................................8 Hardware Requirements .......................................................................................... 8 Operating Systems Supported ................................................................................. 8 Software requirements ............................................................................................ -
Item 3F. LBR-2018-19-039 Joe Goode
CITY AND COUNTY OF SAN FRANCISCO LONDON N. BREED, MAYOR OFFICE OF SMALL BUSINESS REGINA DICK-ENDRIZZI, DIRECTOR Legacy Business Registry Staff Report HEARING DATE JUNE 24, 2019 JOE GOODE PERFORMANCE GROUP Application No.: LBR-2018-19-039 Business Name: Joe Goode Performance Group Business Address: 499 Alabama Street, #150 District: District 9 Applicant: Adriana Marcial, Executive Director Nomination Date: February 7, 2019 Nominated By: Mayor London N. Breed Staff Contact: Richard Kurylo [email protected] BUSINESS DESCRIPTION Choreographer Joe Goode established Joe Goode Performance Group (JGPG) in 1986 with the mission of promoting understanding, compassion, and tolerance among people through the innovative use of dance and theater. JGPG is currently located at 401 Alabama Street in the Project Artaud building, an arts complex in San Francisco's Mission District. Over the past 32 years, JGPG has performed an annual Home Season in San Francisco at venues such as the old Footworks Studio, Cowell Center for Performing Arts, Yerba Buena Center for the Arts, and Z Space. JGPG has also produced site-specific and has offered dance and movement classes in various studios throughout the city since its inception. Before finding a permanent home in the Mission/Potrero Hill in 2011, JGPG acquired a loyal following due to its consistent annual Home Season presentations. JGPG has brought national and international attention to the San Francisco arts scene as the company by touring throughout the U.S. and in Canada, Europe, South America, the Middle East, and Africa. From the beginning, Goode's public stance as an out gay artist making work that sought to identify the commonality of all people helped to de-stigmatize issues of sexuality and gender identity and used the arts as a healing tool in face of the AIDS epidemic. -
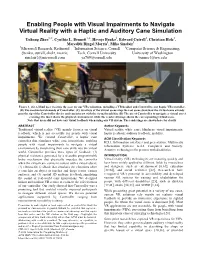
Enabling People with Visual Impairments to Navigate Virtual Reality with a Haptic and Auditory Cane Simulation Yuhang Zhao1, 2, Cynthia L
Enabling People with Visual Impairments to Navigate Virtual Reality with a Haptic and Auditory Cane Simulation Yuhang Zhao1, 2, Cynthia L. Bennett1, 3, Hrvoje Benko1, Edward Cutrell1, Christian Holz1, Meredith Ringel Morris1, Mike Sinclair1 1Microsoft Research, Redmond 2Information Science, Cornell 3Computer Science & Engineering, {benko, cutrell, cholz, merrie, Tech, Cornell University University of Washington sinclair}@microsoft.com [email protected] [email protected] Figure 1. (A) A blind user wearing the gear for our VR evaluation, including a VR headset and Canetroller, our haptic VR controller. (B) The mechanical elements of Canetroller. (C) Overlays of the virtual scene atop the real scene show how the virtual cane extends past the tip of the Canetroller device and can interact with the virtual trash bin. (D) The use of Canetroller to navigate a virtual street crossing: the inset shows the physical environment, while the rendered image shows the corresponding virtual scene. Note that users did not have any visual feedback when using our VR system. The renderings are shown here for clarity. ABSTRACT Author Keywords Traditional virtual reality (VR) mainly focuses on visual Virtual reality; white cane; blindness; visual impairments; feedback, which is not accessible for people with visual haptic feedback; auditory feedback; mobility. impairments. We created Canetroller, a haptic cane ACM Classification Keywords controller that simulates white cane interactions, enabling H.5.1. Information interfaces and presentation: Multimedia people -
![Archive and Compressed [Edit]](https://docslib.b-cdn.net/cover/8796/archive-and-compressed-edit-1288796.webp)
Archive and Compressed [Edit]
Archive and compressed [edit] Main article: List of archive formats • .?Q? – files compressed by the SQ program • 7z – 7-Zip compressed file • AAC – Advanced Audio Coding • ace – ACE compressed file • ALZ – ALZip compressed file • APK – Applications installable on Android • AT3 – Sony's UMD Data compression • .bke – BackupEarth.com Data compression • ARC • ARJ – ARJ compressed file • BA – Scifer Archive (.ba), Scifer External Archive Type • big – Special file compression format used by Electronic Arts for compressing the data for many of EA's games • BIK (.bik) – Bink Video file. A video compression system developed by RAD Game Tools • BKF (.bkf) – Microsoft backup created by NTBACKUP.EXE • bzip2 – (.bz2) • bld - Skyscraper Simulator Building • c4 – JEDMICS image files, a DOD system • cab – Microsoft Cabinet • cals – JEDMICS image files, a DOD system • cpt/sea – Compact Pro (Macintosh) • DAA – Closed-format, Windows-only compressed disk image • deb – Debian Linux install package • DMG – an Apple compressed/encrypted format • DDZ – a file which can only be used by the "daydreamer engine" created by "fever-dreamer", a program similar to RAGS, it's mainly used to make somewhat short games. • DPE – Package of AVE documents made with Aquafadas digital publishing tools. • EEA – An encrypted CAB, ostensibly for protecting email attachments • .egg – Alzip Egg Edition compressed file • EGT (.egt) – EGT Universal Document also used to create compressed cabinet files replaces .ecab • ECAB (.ECAB, .ezip) – EGT Compressed Folder used in advanced systems to compress entire system folders, replaced by EGT Universal Document • ESS (.ess) – EGT SmartSense File, detects files compressed using the EGT compression system. • GHO (.gho, .ghs) – Norton Ghost • gzip (.gz) – Compressed file • IPG (.ipg) – Format in which Apple Inc. -

Sensor-Based Assistive Devices for Visually-Impaired People: Current Status, Challenges, and Future Directions
Review Sensor-Based Assistive Devices for Visually-Impaired People: Current Status, Challenges, and Future Directions Wafa Elmannai and Khaled Elleithy * Department of Computer Science and Engineering, University of Bridgeport, Bridgeport, CT 06604, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-203-576-4703 Academic Editor: Panicos Kyriacou Received: 23 January 2017; Accepted: 1 March 2017; Published: 10 March 2017 Abstract: The World Health Organization (WHO) reported that there are 285 million visually- impaired people worldwide. Among these individuals, there are 39 million who are totally blind. There have been several systems designed to support visually-impaired people and to improve the quality of their lives. Unfortunately, most of these systems are limited in their capabilities. In this paper, we present a comparative survey of the wearable and portable assistive devices for visually- impaired people in order to show the progress in assistive technology for this group of people. Thus, the contribution of this literature survey is to discuss in detail the most significant devices that are presented in the literature to assist this population and highlight the improvements, advantages, disadvantages, and accuracy. Our aim is to address and present most of the issues of these systems to pave the way for other researchers to design devices that ensure safety and independent mobility to visually-impaired people. Keywords: assistive devices; visually-impaired people; obstacles detection; navigation and orientation systems; obstacles avoidance 1. Introduction The World Health Organization (WHO) Fact reported that there are 285 million visually- impaired people worldwide. Among these individuals, there are 39 million who are blind in the world [1]. -
Application Development Standards and Guidelines
FLORIDA DEPARTMENT OF AGRICULTURE AND CONSUMER SERVICES APPLICATION DEVELOPMENT STANDARDS AND GUIDELINES VERSION 8.5 Creation Date: 04/21/2000 Last Updated: 07/12/2017 Application Development Standards TABLE OF CONTENTS ECTION 1: PURPOSE ......................................................................................................................... - 4 - SECTION 2: SCOPE ............................................................................................................................ - 4 - SECTION 3: CHANGE PROCEDURES FOR THE APPLICATION DEVELOPMENT STANDARDS ........................................................................................................................................ - 5 - SECTION 4: SECURITY ...................................................................................................................... - 5 - SECTION 4.1: NETWORK USER ACCOUNT ACCESS TYPES ...................................................................... - 6 - SECTION 4.2: ORACLE DATABASE LOGINS AND SECURITY .................................................................. - 7 - SECTION 4.3: MICROSOFT ACCESS SECURITY ........................................................................................ - 12 - SECTION 4.5: PASSWORDS ........................................................................................................................... - 13 - SECTION 5: 60-8.001 FLORIDA ACCESSIBLE AND ELECTRONIC INFORMATION TECHNOLOGY RULE ...................................................................................................................... -

MUSCULOSKELETAL PHYSICAL THERAPY for SACROILIAC JOINT PAIN Anas Alhakami*1, Mohammed Qasheesh2, Senthilkumar Cennappan Bose3
International Journal of Physiotherapy and Research, Int J Physiother Res 2020, Vol 8(4):3533-36. ISSN 2321-1822 Case Report DOI: https://dx.doi.org/10.16965/ijpr.2020.144 MUSCULOSKELETAL PHYSICAL THERAPY FOR SACROILIAC JOINT PAIN Anas Alhakami*1, Mohammed Qasheesh2, Senthilkumar Cennappan Bose3. *1 Senior Musculoskeletal Physical Therapist, King Faisal Medical City for Southern Regions, Kingdom of Saudi Arabia. 2 Assistant Professor and Head-Physical Therapy, Jazan University,Kingdom of Saudi Arabia 3 Lecturer-Physical Therapy, Jazan University, Kingdom of Saudi Arabia. ABSTRACT This case report describes a clinical case of a 53 years aged male with Low Back Pain(LBP) at Sacro Iliac Joint(SIJ). Patient referred to physical therapy department with LBP over the past 3 weeks. Pain extended to posterior aspect of left thigh and worsening with prolonged standing, sitting and with stair climbing. Moreover, he found difficulty to ride his car or going from sit to stand. He had a history of road traffic accident 30 years ago that led to severe pain in his lower back area, he was a farmer as well and was working hardly more than 8 hours daily by lifting heavy objects. Patient came to the department by walking with assistive cane. By palpation, there was a local tenderness at the posterior aspect of the SIJ. Range of motion was limited by pain in lumbar flexion, extension, rotation and bilateral side bending movements. Pain scored 7 out of 10 on Numerical Pain Rating Visual Analogue Scale. Functional disability scored 19 out of 24 on Roland-Morris Disability questionnaire. -

French (12.86Mb)
NATIONS UNIES UNEP/MED WG.482/18 PROGRAMME DES NATIONS UNIES POUR L’ENVIRONNEMENT PLAN D’ACTION POUR LA MÉDITERRANÉE 2 novembre 2020 Français Original : anglais Réunions intégrées des groupes de correspondance de l'approche écosystémique sur la mise en œuvre de l’IMAP (CORMONs) Vidéoconférence, 1-3 décembre 2020 Point 5 de l’ordre du jour : Sessions CORMON parallèles (Pollution et déchets marins, et Biodiversité et pêche) Directives/Protocoles de contrôle concernant la préparation et l’analyse des échantillons des échantillons des produits de la mer pour l’indicateur commun 20 de l’IMAP : métaux lourds, éléments traces et polluants organiques Pour des raisons environnementales et économiques, le tirage du présent document a été restreint. Les participants sont priés d’apporter leur copie à la réunion et de ne pas demander de copies supplémentaires. PNUE/PAM Athènes, 2020 Table des matières 1 Introduction .................................................................................................................................... 1 2 Note technique pour l'analyse des échantillons de tissus de poissons et de fruits de mer pour la recherche de métaux lourds ...................................................................................................................... 3 Protocole pour la digestion des tissus du biote à l'aide d'acide nitrique ............................................... 6 Protocole pour l’analyse des métaux lourds à l'aide de la AAS ........................................................... 7 Protocole pour -

Assistive Multi-Purpose Mobility Device with Folding Temporary Seat
Assistive Multi-Purpose Mobility Device with Folding Temporary Seat A Major Qualifying Project Proposal Submitted to the Faculty of WORCESTER POLYTECHNIC INSTITUTE in partial fulfillment of the requirements for the Degree of Bachelor of Science by _________________________ Xinping Deng _________________________ Daniel Haley _________________________ Taylor Roseen Date: 4/30/15 Approved: ______________________________ Professor Allen H. Hoffman, Co-Advisor ______________________________ Professor Holly K. Ault, Co-Advisor Abstract Crutches and canes are widely used around the world as a means of providing stability and support for those who need them; the elderly population in particular utilizes these devices the most. There are numerous products on the market that attempt to add a seat to the crutch or cane in an effort to alleviate the stress of standing for too long. However, these products are oftentimes too cumbersome, heavy, or just simply unsafe. The goal of this project is to design and build a device that can be used as either a crutch or a cane that gives stability and helps support the weight of the user while standing and walking, additionally offering the ability for the user to rest comfortably and safely in a seated position when necessary. A first generation prototype was successfully manufactured using an existing forearm crutch and machined aluminum and steel components. The prototype underwent load and dimension tests in addition to students conducting overall usability tests. i Table of Contents Abstract ......................................................................................................................................................... -

Electronic Smart Canes for Visually Impaired People
NATIONAL AND KAPODISTRIAN UNIVERSITY OF ATHENS SCHOOL OF SCIENCE DEPARTMENT OF INFORMATICS AND TELECOMMUNICATION BSc THESIS Electronic Smart Canes for Visually Impaired People Dimitra P. Marini Supervisor: Georgios Kouroupetroglou, Associate Professor ATHENS MARCH 2018 ΕΘΝΙΚΟ ΚΑΙ ΚΑΠΟΔΙΣΤΡΙΑΚΟ ΠΑΝΕΠΙΣΤΗΜΙΟ ΑΘΗΝΩΝ ΣΧΟΛΗ ΘΕΤΙΚΩΝ ΕΠΙΣΤΗΜΩΝ ΤΜΗΜΑ ΠΛΗΡΟΦΟΡΙΚΗΣ ΚΑΙ ΤΗΛΕΠΙΚΟΙΝΩΝΙΩΝ ΠΤΥΧΙΑΚΗ ΕΡΓΑΣΙΑ Έξυπνα Ηλεκτρονικά Μπαστούνια για Άτομα με Απώλεια Όρασης Δήμητρα Π. Μαρίνη Επιβλέπων: Γεώργιος Κουρουπέτρογλου, Αναπληρωτής Καθηγητής ΑΘΗΝΑ ΜΑΡΤΙΟΣ 2018 BSc THESIS Electronic Smart Canes for Visually Impaired People Dimitra P. Marini S.N.: 1115201100044 SUPERVISOR: Georgios Kouroupetroglou, Associate Professor ΠΤΥΧΙΑΚΗ ΕΡΓΑΣΙΑ Έξυπνα Ηλεκτρονικά Μπαστούνια για Άτομα με Απώλεια Όρασης Δήμητρα Π. Μαρίνη Α.Μ.: 1115201100044 ΕΠΙΒΛΕΠΩΝ: Γεώργιος Κουρουπέτρογλου, Αναπληρωτής Καθηγητής ABSTRACT The purpose of this paper is to present and describe existing devices and smart-stick technologies for blind and visually impaired people. This state-of-the-art review includes the most recent research results of international scientific literature (published in scientific journals, conferences, etc.), patents and commercially available products. These technologies are classified according to their basic characteristics and are then accompanied by of the research trials conducted (where reference is made to the respective sources) and their results. In order to achieve this goal, after an extensive search in the international scientific literature, the most important and most recent technologies of smart sticks were selected and the operating principle of each of them was briefly described. Subsequently, the devices were classified according to the technologies they use and their basic characteristics, along with the additional information on the relative user trials and their results. The positive and negative aspects of each device as well as whether it covers the needs and requirements of visually impaired people are easily distinguishable.