NJP VOLUME 39 No 4
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Interim Capacity Building for Operators of Microfinance Banks
Central Bank of Nigeria INTERIM CAPACITY BUILDING WORKSHOP FOR OPERATORS OF MICROFINACE BANKS IN NIGERIA The Central Bank of Nigeria (CBN) is organizing a capacity building workshop for operators of licensed Microfinance Banks in Nigeria. There will be four runs of 3 days each from 1st to 13th September, 2008. The workshop will be held concurrently in eight centres as detailed below: AWKA CENTRE: Venue: Choice Hotel, 71, Arthur Eze Avenue, Awka, Anambra State. Institutions: S/N NAME OF MFB ADDRESS STATE ADAZI ANI TOWN HALL, ADAZI ANI, ANAOCHA LGA, 1 AACB MFB ANAMBRA STATE ANAMBRA NKWOR MARKET SQUARE, ADAZI-ENU, ANAOCHA 2 ADAZI-ENU MFB LGA, ANAMBRA STATE ANAMBRA AKPO JUNCTION, AKPO AGUATA LGA, ANAMBRA 3 AKPO MFB STATE ANAMBRA CIVIC CENTRE COMPLEX, ADAZI-ENU, ANAOCHA 4 BESTWAY MFB LGA, ANAMBRA STATE ANAMBRA NO 1 MISSION ROAD EKWULOBIA P.M.B.24 AGUTA, 5 EKWULOBIA MFB ANAMBRA ANAMBRA 1 BANK ROAD UMUCHU, AGUATA L.G.A, ANAMBRA 6 EQUINOX MFB STATE ANAMBRA AFOR IGWE UMUDIOKA, DUNUKOFIA LGA, ANAMBRA 7 EZEBO MFB STATE ANAMBRA KM 6, ONITHSA OKIGWE RD., ICHI, EKWUSIGO LGA, 8 ICHI MFB ANAMBRA STATE ANAMBRA NNOBI/EKWULOBIA ROAD, IGBOUKWU, ANAMBRA 9 IGBO-UKWU MFB STATE ANAMBRA 10 IHIALA MFB BANK HOUSE, ORLU ROAD, IHIALA, ANAMBRA STATE ANAMBRA EKWUSIGO PARK, ISUOFIA-NNEWI ROAD, ISUOFIA, 11 ISUOFIA MFB ANAMBRA STATE ANAMBRA ZONE 16, NO.6-9, MAIN MARKET, NKWO-NNEWI, 12 MBAWULU MFB ANAMBRA STATE ANAMBRA STATE SECRETARIAT, GOVERNMENT HOUSE, AWKA, 13 NDIOLU MFB ANAMBRA STATE ANAMBRA NGENE-OKA MARKET SQ., ALONG AMAWBIA/AGULU 14 NICE MFB ROAD, NISE, AWKA SOUTH -

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

European Journal of Education Studies
European Journal of Education Studies ISSN: 2501 - 1111 ISSN-L: 2501 - 1111 Available on-line at: www.oapub.org/edu doi: 10.5281/zenodo.1199691 Volume 4 │ Issue 3 │ 2018 ASSESSMENT OF SCHOOL-BASED MANAGEMENT COMMITTEES’ (SBMCs) PHYSICAL AND FINANCIAL RESOURCES MANAGEMENT FUNCTIONS IN ANAOCHA LOCAL GOVERNMENT AREA, NIGERIA Eboatu, V. N.1i, Carol Obiageli Ezeugbor1, Golu, Joseph Arinze2 1PhD, Department of Educational Management and Policy, Nnamdi Azikiwe University, Awka, Nigeria 2Department of Educational Management and Policy, Nnamdi Azikiwe University, Awka, Nigeria Abstract: The responsibilities of the School-Based Management Committee (SBMC) include to ensure effective utilization of physical resources and to promote transparency, probity and accountability in school finances. This function becomes more critical in this period of economic recession in Nigeria. This study sought and established the extent of the School-Based Management Committees’ promotion of accountability and proper utilization of physical resources in the public secondary schools in Anaocha Local Government Area of Anambra State. The survey research method was adopted. Two (2) research questions guided the study, while two (2) hypotheses were tested at 0.05 significance level. The population of the study was 362; comprising 330 teachers, 16 community leaders and 16 principals, from which a sample of 236 (220 teachers, 8 principals and 8 community leaders) was drawn through simple random sampling technique. A 10- item Questionnaire, duly validated was used for collection of data. Data collected were analysed using mean score to answer the research questions and ANOVA to test the hypotheses. The study established among other things, that the SBMCs in Anaocha Local Government Area to a low extent contribute to ensuring proper utilization of physical resources, but to a high extent promote financial accountability in the use of school financial resources. -

New Media and Crime Among Adolescents in Anaocha LGA of Anambra Nigeria
Current Journal of Applied Science and Technology 40(1): 65-78, 2021; Article no.CJAST.65299 ISSN: 2457-1024 (Past name: British Journal of Applied Science & Technology, Past ISSN: 2231-0843, NLM ID: 101664541) New Media and Crime among Adolescents in Anaocha LGA of Anambra Nigeria Chelsea C. Adogu1, Henry N. Chineke2, Prosper O. U. Adogu3*, Chika F. Ubajaka3, Amara F. Chizoba4, and Chinelo C. Nduka5 1Department of Sociology and Anthropology, Nnamdi Azikiwe, University, Awka, Nigeria. 2Department of Family Medicine, Imo State University, Owerri, Nigeria. 3Department of Community Medicine, Nnamdi Azikiwe University, Awka, Nigeria. 4Renewal Health Foundation Nigeria. 5Department of Community Medicine, NAU Teaching Hospital, Nnewi, Nigeria. Authors’ contributions This work was carried out in collaboration among all authors. Authors CCA and POUA designed the study, performed the statistical analysis, wrote the protocol, and wrote the first draft of the manuscript. Authors HNC and CFU managed the analyses of the study. Authors AFC and CCN managed the literature searches. All authors read and approved the final manuscript. Article Information DOI: 10.9734/CJAST/2021/v40i131222 Editor(s): (1) Dr. Ritu Singh, G.B. Pant University of Agriculture and Technology, India. (2) Dr. Kleopatra Nikolopoulou, University of Athens, Greece. Reviewers: (1) Nidia Milena Moreno López, Universidad Nacional Abierta y a Distancia UNAD, Colombia. (2) Chin Fung, The Education University of Hong Kong, Hong Kong. Complete Peer review History: http://www.sdiarticle4.com/review-history/65299 Received 02 December 2020 Accepted 08 February 2021 Original Research Article Published 20 February 2021 ABSTRACT New media use has been recently understood as an important issue to be looked into among adolescents, parents and others who deal with adolescents. -

Research Report
1.1 CHAPTER 1 INTRODUCTION Soil erosion is the systematic removal of soil, including plant nutrients, from the land surface by various agents of denudation (Ofomata, 1985). Water being the dominant agent of denudation initiates erosion by rain splash impact, drag and tractive force acting on individual particles of the surface soil. These are consequently transported seizing slope advantage for deposition elsewhere. Soil erosion is generally created by initial incision into the subsurface by concentrated runoff water along lines or zones of weakness such as tension and desiccation fractures. As these deepen, the sides give in or slide with the erosion of the side walls forming gullies. During the Stone Age, soil erosion was counted as a blessing because it unearths valuable treasures which lie hidden below the earth strata like gold, diamond and archaeological remains. Today, soil erosion has become an endemic global problem, In the South eastern Nigeria, mostly in Anambra State, it is an age long one that has attained a catastrophic dimension. This environmental hazard, because of the striking imprints on the landscape, has sparked off serious attention of researchers and government organisations for sometime now. Grove(1951); Carter(1958); Floyd(1965); Ofomata (1964,1965,1967,1973,and 1981); all made significant and refreshing contributions on the processes and measures to combat soil erosion. Gully Erosion is however the prominent feature in the landscape of Anambra State. The topography of the area as well as the nature of the soil contributes to speedy formation and spreading of gullies in the area (Ofomata, 2000);. 1.2 Erosion Types There are various types of erosion which occur these include Soil Erosion Rill Erosion Gully Erosion Sheet Erosion 1.2.1 Soil Erosion: This has been occurring for some 450 million years, since the first land plants formed the first soil. -

Dictionary of Ò,Nì,Chà Igbo
Dictionary of Ònìchà Igbo 2nd edition of the Igbo dictionary, Kay Williamson, Ethiope Press, 1972. Kay Williamson (†) This version prepared and edited by Roger Blench Roger Blench Mallam Dendo 8, Guest Road Cambridge CB1 2AL United Kingdom Voice/ Fax. 0044-(0)1223-560687 Mobile worldwide (00-44)-(0)7967-696804 E-mail [email protected] http://www.rogerblench.info/RBOP.htm To whom all correspondence should be addressed. This printout: November 16, 2006 TABLE OF CONTENTS Abbreviations: ................................................................................................................................................. 2 Editor’s Preface............................................................................................................................................... 1 Editor’s note: The Echeruo (1997) and Igwe (1999) Igbo dictionaries ...................................................... 2 INTRODUCTION........................................................................................................................................... 4 1. Earlier lexicographical work on Igbo........................................................................................................ 4 2. The development of the present work ....................................................................................................... 6 3. Onitsha Igbo ................................................................................................................................................ 9 4. Alphabetization and arrangement.......................................................................................................... -

Household Water Demand in the Peri-Urban Communities of Awka, Capital of Anambra State, Nigeria
Vol. 6(6), pp. 237-243, August, 2013 DOI: 10.5897/JGRP2013.0385 Journal of Geography and Regional Planning ISSN 2070-1845 © 2013 Academic Journals http://www.academicjournals.org/JGRP Full Length Research Paper Household water demand in the peri-urban communities of Awka, Capital of Anambra State, Nigeria E. E. Ezenwaji1*, P.O. Phil-Eze2, V. I. Otti3 and B. M. Eduputa4 1Department of Geography and Meteorology, Nnamdi Azikiwe University, Awka, Nigeria. 2Department of Geography, University of Nigeria, Nsukka, Nigeria. 3Civil Engineering Department, Federal Polytechnic, Oko, Nigeria. 4Department of Environmental Management, Nnamdi Azikiwe University, Awka, Nigeria. Accepted 22 July, 2013 The aim of this paper is to determine relevant factors contributing to the water demand in the peri-urban communities of Awka capital city. Towards achieving this aim, questionnaire were developed and served on the households in various communities to collect relevant data on the 13 physical and socio- economic factors we earlier identified as influencing water demand in the area. Water quality was ascertained through microbiological analysis of water samples. The major analytical techniques used were multiple correlations, the result of which was subjected to Principal Component Analysis (PCA) and Principal Component Regression. Result shows that the 13 variables combined to contribute 90.0% of water demand in the area. Furthermore, the low standard error of estimates of 0.029 litres shows that water demand in the communities could be predicted using the 13 variables. Policy and planning measures to improve the water supply situation of the area were suggested. Key words: Capital, communities, factors, peri-urban, water demand. -

STRUCTURE PLAN for Awka and SATELLITE TOWNS
AWKA STRUCTURE PLAN FOR AWKA AND SATELLITE TOWNS Anambra State STRUCTURE PLAN FOR AWKA AND SATELLITE TOWNS Anambra State 1 Structure Plan for Awka and Satellite Towns Copyright © United Nations Human Settlements Programme (UN-HABITAT), 2009 All rights reserved United Nations Human Settlements Programme publications can be obtained from UN-HABITAT Regional and Information Offices or directly from: P.O.Box 30030, GPO 00100 Nairobi, Kenya. Fax: + (254 20) 762 4266/7 E-mail: [email protected] Website: http://www.unhabitat.org HS/1152/09E ISBN: 978-92-1-132118-0 DISCLAIMER The designation employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning delimitation of its frontiers or boundaries, or regarding its economic system or degree of development. The analysis, conclusions and recommendations of the report do not necessarily reflect the views of the United Nations Human Settlements Programme (UN-HABITAT), the Governing Council of UN-HABITAT or its Member States. Excerpts from this publication may be reproduced without authorisation, on condition that the source is indicated. Photo Credits : © UN-HABITAT acknowLEDGEMents Director: Dr Alioune Badiane Principal Editor: Prof. Johnson Bade Falade Co-ordinator: Dr. Don Okpala Principal Authors: Prof. Louis C. Umeh Prof. Samson O. Fadare Dr. Carol Arinze –Umobi Chris Ikenna Udeaja Tpl. (Dr) Francis Onweluzo Design and Layout: Andrew Ondoo 2 FOREWORD t is now widely It is to reverse and stem this development trend acknowledged and to realize the developmental potentials of well- and accepted that planned and managed cities, towns and villages, that citiesI and urban areas my Government approached the United Nations are engines of economic Human Settlements Programme (UN-HABITAT) in development and growth. -

States and Lcdas Codes.Cdr
PFA CODES 28 UKANEFUN KPK AK 6 CHIBOK CBK BO 8 ETSAKO-EAST AGD ED 20 ONUIMO KWE IM 32 RIMIN-GADO RMG KN KWARA 9 IJEBU-NORTH JGB OG 30 OYO-EAST YYY OY YOBE 1 Stanbic IBTC Pension Managers Limited 0021 29 URU OFFONG ORUKO UFG AK 7 DAMBOA DAM BO 9 ETSAKO-WEST AUC ED 21 ORLU RLU IM 33 ROGO RGG KN S/N LGA NAME LGA STATE 10 IJEBU-NORTH-EAST JNE OG 31 SAKI-EAST GMD OY S/N LGA NAME LGA STATE 2 Premium Pension Limited 0022 30 URUAN DUU AK 8 DIKWA DKW BO 10 IGUEBEN GUE ED 22 ORSU AWT IM 34 SHANONO SNN KN CODE CODE 11 IJEBU-ODE JBD OG 32 SAKI-WEST SHK OY CODE CODE 3 Leadway Pensure PFA Limited 0023 31 UYO UYY AK 9 GUBIO GUB BO 11 IKPOBA-OKHA DGE ED 23 ORU-EAST MMA IM 35 SUMAILA SML KN 1 ASA AFN KW 12 IKENNE KNN OG 33 SURULERE RSD OY 1 BADE GSH YB 4 Sigma Pensions Limited 0024 10 GUZAMALA GZM BO 12 OREDO BEN ED 24 ORU-WEST NGB IM 36 TAKAI TAK KN 2 BARUTEN KSB KW 13 IMEKO-AFON MEK OG 2 BOSARI DPH YB 5 Pensions Alliance Limited 0025 ANAMBRA 11 GWOZA GZA BO 13 ORHIONMWON ABD ED 25 OWERRI-MUNICIPAL WER IM 37 TARAUNI TRN KN 3 EDU LAF KW 14 IPOKIA PKA OG PLATEAU 3 DAMATURU DTR YB 6 ARM Pension Managers Limited 0026 S/N LGA NAME LGA STATE 12 HAWUL HWL BO 14 OVIA-NORTH-EAST AKA ED 26 26 OWERRI-NORTH RRT IM 38 TOFA TEA KN 4 EKITI ARP KW 15 OBAFEMI OWODE WDE OG S/N LGA NAME LGA STATE 4 FIKA FKA YB 7 Trustfund Pensions Plc 0028 CODE CODE 13 JERE JRE BO 15 OVIA-SOUTH-WEST GBZ ED 27 27 OWERRI-WEST UMG IM 39 TSANYAWA TYW KN 5 IFELODUN SHA KW 16 ODEDAH DED OG CODE CODE 5 FUNE FUN YB 8 First Guarantee Pension Limited 0029 1 AGUATA AGU AN 14 KAGA KGG BO 16 OWAN-EAST -
State: Anambra Code: 04
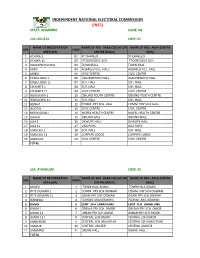
INDEPENDENT NATIONAL ELECTORAL COMMISSION (INEC) STATE: ANAMBRA CODE: 04 LGA :AGUATA CODE: 01 NAME OF REGISTRATION NAME OF REG. AREA COLLATION NAME OF REG. AREA CENTRE S/N CODE AREA (RA) CENTRE (RACC) (RAC) 1 ACHINA 1 01 ST CHARLED ST CHARLED 2 ACHINA 11 02 PTOGRESSIVE SCH. PTOGRESSIVE SCH. 3 AGULEZECHUKWU 03 TOWN HALL TOWN HALL 4 AKPO 04 AGBAELU VILL. HALL AGBAELU VILL. HALL 5 AMESI 05 CIVIC CENTRE CIVIC CENTRE 6 EKWULOBIA 1 06 UMUEZENOFO HALL. UMUEZENOFO HALL. 7 EKWULOBIA 11 07 SCH. HALL SCH. HALL 8 EZENIFITE 1 08 SCH. HALL SCH. HALL 9 EZENIFITE 11 09 CIVIC CENTRE CIVIC CENTRE 10 IGBOUKWU 1 10 OBIUNO YOUTH CENTRE OBIUNO YOUTH CENTRE 11 IGBOUKWU 11 11 SCH. HALL SCH. HALL 12 IKENGA 12 COMM. PRY SCH. HALL COMM. PRY SCH. HALL 13 ISUOFIA 13 CIVIC CENTRE CIVIC CENTRE 14 NKPOLOGWU 14 MOFEL HEALTH CENTRE MOFEL HEALTH CENTRE 15 ORAERI 15 OBIUNO HALL OBIUNO HALL 16 UGA 1 16 OKWUTE HALL OKWUTE HALL 17 UGA 11 17 UGA BOYS UGA BOYS 18 UMUCHU 1 18 SCH. HALL SCH. HALL 19 UMUCHU 11 19 CORPERS LODGE CORPERS LODGE 20 UMOUNA 20 CIVIC CENTRE CIVIC CENTRE TOTAL LGA: AYAMELUM CODE: 02 NAME OF REGISTRATION NAME OF REG. AREA COLLATION NAME OF REG. AREA CENTRE S/N CODE AREA (RA) CENTRE (RACC) (RAC) 1 ANAKU 1 TOWN HALL ANAKU TOWN HALL ANAKU 2 IFITE OGWARI 1 2 COMM. PRY SCH.OGWARI COMM. PRY SCH.OGWARI 3 IFITE OGWARI 11 3 OGARI PRY SCH.OGWARI OGARI PRY SCH.OGWARI 4 IGBAKWU 4 ISIOKWE ARA,IGBAKWU ISIOKWE ARA,IGBAKWU 5 OMASI 5 CENT. -

June 2014 Issues of the Knights Section 4, Pages 8-9, Which Now Reads Commanders Journal and Will Be Discussed and Voted
JUNE, 2014 R 1 R Published Quarterly Second Class Postage Paid at Celina, Ohio (USPS 296880) Vol. 51 No. 2 IN GOD WE TRUST June, 2014 St. George Commanderies 97 and 98 Welcome All to Columbus, Ohio “With God, All Things Are Possible” KNIGHTS OF ST JOHN INTERNATIONAL 79th International _ 53rd Biennial Convention and Ladies Auxiliary 58th International Convention _ July 20 26, 2014 See pages 18 and 19 for 2014 Supreme Convention Registration and Hotel Registration forms. Note cutoff dates. 2 R JUNE, 2014 POSTMASTER Supreme Treasurer - Lieut. Gen. Terrence W. OVERSEAS GRAND PRESIDENTS Send address changes to: McCann, 63 Butternut Circle, Orchard Park, Accra-East - Brig. Gen. Anthony Chinebuah, Box Knight Of St. John N.Y. 14127-1904 - Tel. 716-662-5723. - Assistant 8399, Tema, Ghana, W.A. - MOB:+233-24-4330217 The Messenger Press Supreme Treasurer - Francis Jerome Countiss, Jr. [email protected] Carthagena, OH 45822-9998 Supreme Trustee - Major Gen. Douglas Accra-West - Brig. Gen. William Adjei, Box Francony, 1010 W. North St., Piqua, OH 45356 AN8356, Accra-North, Ghana, W.A. - MOB: +233- The Knight of St. John is the official organ of the Tel/Fax 937-778-0804 - [email protected] 24-4356277 - [email protected] Knights of St. John Internatinal and is entirely de- Supreme Trustee - Major Gen. Dan Anaebo Cape Coast - Brig. Gen. Francis Koomson-Barnes, voted to their interests. Okekenta, Darumi District of Area One Flyover, P.O. Box CC1471, Cape Coast, Ghana - Tel. +233- The Knight of St. John is published under the P.O. Box 6252, Garki, Abuja, Nigeria, W.A. -

Agulu Road, Adazi Ani, Anambra State. ANAMBRA 2 AB Microfinance Bank Limited National No
LICENSED MICROFINANCE BANKS (MFBs) IN NIGERIA AS AT SEPTEMBER 22, 2017 # Name Category Address State Description 1 AACB Microfinance Bank Limited State Nnewi/ Agulu Road, Adazi Ani, Anambra State. ANAMBRA 2 AB Microfinance Bank Limited National No. 9 Oba Akran Avenue, Ikeja Lagos State. LAGOS 3 Abatete Microfinance Bank Limited Unit Abatete Town, Idemili Local Govt Area, Anambra State ANAMBRA 4 ABC Microfinance Bank Limited Unit Mission Road, Okada, Edo State EDO 5 Abestone Microfinance Bank Ltd Unit Commerce House, Beside Government House, Oke Igbein, Abeokuta, Ogun State OGUN 6 Abia State University Microfinance Bank Limited Unit Uturu, Isuikwuato LGA, Abia State ABIA 7 Abigi Microfinance Bank Limited Unit 28, Moborode Odofin Street, Ijebu Waterside, Ogun State OGUN 8 Abokie Microfinance Bank Limited Unit Plot 2, Murtala Mohammed Square, By Independence Way, Kaduna State. KADUNA 9 Abubakar Tafawa Balewa University Microfinance Bank Limited Unit Abubakar Tafawa Balewa University (ATBU), Yelwa Road, Bauchi Bauchi 10 Abucoop Microfinance Bank Limited State Plot 251, Millenium Builder's Plaza, Hebert Macaulay Way, Central Business District, Garki, Abuja ABUJA 11 Accion Microfinance Bank Limited National 4th Floor, Elizade Plaza, 322A, Ikorodu Road, Beside LASU Mini Campus, Anthony, Lagos LAGOS 12 ACE Microfinance Bank Limited Unit 3, Daniel Aliyu Street, Kwali, Abuja ABUJA 13 Acheajebwa Microfinance Bank Limited Unit Sarkin Pawa Town, Muya L.G.A Niger State NIGER 14 Achina Microfinance Bank Limited Unit Achina Aguata LGA, Anambra State ANAMBRA 15 Active Point Microfinance Bank Limited State 18A Nkemba Street, Uyo, Akwa Ibom State AKWA IBOM 16 Acuity Microfinance Bank Limited Unit 167, Adeniji Adele Road, Lagos LAGOS 17 Ada Microfinance Bank Limited Unit Agwada Town, Kokona Local Govt.