Women's Longitudinal Study Reports on Rural-Urban Differences
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Appendix 3J Cross-Border Issues and Australian Bushfires
3J-1 Appendix 3J Cross-Border Issues and Australian Bushfires Table 3J-1 below contains 26 extracts from books, reports and papers, from 1983 through to 2005, which describe the impact of Australia's State-Territory borders and cross-border issues on operational responses to bushfires, and associated costs to individuals, communities and governments. These 26 extracts include 1 from 1983; 1 from 1998; 1 from 2000; 1 from 2001; 1 from 2002; 15 from 2003 (including reports on the January 2003 Canberra bushfires by the Canberra Times and the ACT Stateline television program, and the McLeod and Nairn Reports); 4 from 2004 (including the COAG Report by Ellis et al.), and 2 from 2005. 3J-2 Table 3J-1: Extracts on State-Territory Cross-Border Issues Arising in Relation to Australian Bushfires Source Selected Extracts Whitlam (1983: 40-42): The cost of Australian federalism is horrendous enough when the federal government and a state government or state governments duplicate services for which there is a commonly accepted standard. The cost is higher still when they supply services for which there is not such a standard. The most notorious case in Australian history concerned the railways where the states adopted three different gauges. ... The break of gauge syndrome has another manifestation which was brought to my attention by a fire in the bulk sugar terminal at Townsville in May 1963. The terminal's own fire fighting equipment could not cope. The adjacent Harbour Board could not assist, since its hoses could not be coupled with those of the terminal. Nor could the hoses of the City Council nor those of the federal departments of Civil Aviation and of Air at the airport. -
Emergency Services Bureau Structure
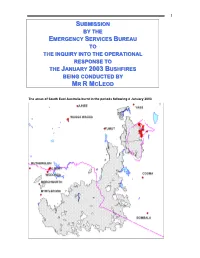
1 SSSUUUBBBMMMIIISSSSSSIIIOOONNN BBBYYY TTTHHHEEE EEEMMMEEERRRGGGEEENNNCCCYYY SSSEEERRRVVVIIICCCEEESSS BBBUUURRREEEAAAUUU TTTOOO TTTHHHEEE IIINNNQQQUUUIIIRRRYYY IIINNNTTTOOO TTTHHHEEE OOOPPPEEERRRAAATTTIIIOOONNNAAALLL RRREEESSSPPPOOONNNSSSEEE TTTOOO TTTHHHEEE JJJAAANNNUUUAAARRRYYY 222000000333 BBBUUUSSSHHHFFFIIIRRREEESSS BBBEEEIIINNNGGG CCCOOONNNDDDUUUCCCTTTEEEDDD BBBYYY MMMRRR RRR MMMCCCLLLEEEOOODDD The areas of South East Australia burnt in the periods following 8 January 2003 2 TABLE OF CONTENTS INTRODUCTION .........................................................................................................5 GLOSSARY...................................................................................................................8 ACRONYMS...............................................................................................................11 EMERGENCY SERVICES BUREAU STRUCTURE ..................................................13 ROLES AND OBJECTIVES....................................................................................13 HISTORY ...................................................................................................13 ORGANISATIONAL STRUCTURE ...............................................................14 MISSION..............................................................................................................17 VALUES ...............................................................................................................17 SERVICES PROVIDED...............................................................................17 -

Australia 2020 Crime & Safety Report: Canberra
Australia 2020 Crime & Safety Report: Canberra This is an annual report produced in conjunction with the Regional Security Office at the U.S. Embassy in Canberra. OSAC encourages travelers to use this report (as well as the Crime & Safety Reports for other posts across Australia) to gain baseline knowledge of security conditions in Australia. For more in-depth information, review OSAC’s Australia country page for original OSAC reporting, consular messages, and contact information, some of which may be available only to private-sector representatives with an OSAC password. Travel Advisory The current U.S. Department of State Travel Advisory at the date of this report’s publication assesses Australia at Level 1, indicating travelers should exercise normal precautions. Review OSAC’s report, Understanding the Consular Travel Advisory System. Overall Crime and Safety Situation Crime Threats The U.S. Department of State has assessed Canberra as being a LOW-threat location for crime directed at or affecting official U.S. government interests. Property crimes, such as burglary, breaking and entering, and theft occur throughout Australia, and are among the crimes most likely for Australians and foreigners alike to encounter. Physical assaults are relatively uncommon, but occur with greater frequency in specific locales, predominantly outside of the city center. Crime in the central business district includes illegal recreational drug use and associated behavior, particularly after midnight. According to the Australian Bureau of Statistics National Crime Victimization Survey, 468,200 Australians (2.4%) experienced physical assault in the 2018-2019 reporting period; 600,900 (3.0%) experienced “threatened assault;” 231,000 households (2.4%) experienced a break-in; and 439,600 households (4.6%) experienced malicious property damage. -

Nsw Health Medical Retrieval - Helicopter Services in the Southern Region for the Ambulance Service of Nsw
Toll - Southern Region - DOV No 3 - Attachment 1 Redacted Contract - Execution Version (ACW:LW) CONTRACT NO HAC 13/63 BETWEEN THE HEALTH ADMINISTRATION CORPORATION AND TOLL HELICOPTERS (NSW) PTY LTD FOR NSW HEALTH MEDICAL RETRIEVAL - HELICOPTER SERVICES IN THE SOUTHERN REGION FOR THE AMBULANCE SERVICE OF NSW Clayton Utz Lawyers Level 10, 2 Phillip Law Street, Canberra ACT 2600 Australia GPO Box 9806 Canberra ACT 2601 T +61 2 6279 4008 F +61 2 6279 4099 (ACW:LW:KK) www.claytonutz.com Our reference 130/13647/80149353 1 L\339002597.1 Toll - Southern Region - DOV No 3 - Attachment 1 Redacted Contract - Execution Version (ACW:LW) CONTENTS 1. Definitions and Interpretation ................................................................................................... 4 2. Term ........................................................................................................................................... 23 3. Security ..................................................................................................................................... 25 4. Readiness for Handover .......................................................................................................... 26 4A Bankstown Base ................................................................................................................... 29 4B Aircraft Replacement ............................................................................................................ 29 5. Scope of Contract ................................................................................................................... -

Regional ~~~, Development J. a La$1VCA.(Ica
r:/r' 1 Regional ~~~, Development J. A lA$1VCA.(iCA. AUSTRALIAN CAPITAL TERRITORY Submission to the ACT Assembly Select Committee on Regional Development A.C.T. LEGJSLNI'IVE ASSEMBLY COMMl'r'l'EE OFFICE SUBMISSION '.NUME:f~H lo ------------------~DA'l'li: AU'l'H'D l'~OH PUBLICATION 1 '· . :-, '~o ~, "-. '. ·' f Table of Contents TERMS OF REFERENCE .........•••.••••••••••.....•.••.••.....•.•.........•.••.•.•.•.••.............••..••.••.•....•............•.•.•••.•...•...... 3 OVERVIEW OF THE REGIONAL DEVELOPMENT AUSTRALIA PROGRAM •.••..........••...•.•..•.••.•.•.............••.••••.•............. 4 BACKGROUND/OVERVIEW .•.•....•.•••••••••.•....•...•.•.•••.•.••••.••.•........•.••.•. •.• .••..•.•.....•...•.••.••.••.•.•..•....•....•..•.•.•.•.. 5 Introduction ............................................................................................................................................. 5 The Acr region defined ............................................................................................................................. 5 ACT Government support for the RDA Acr ................................................................................................ 5 The Acr and its relationship to the Region ................................................................................................. 6 The Region's relationship with the Acr ..................................................................................................... 7 RDA ACT- Current initiatives and engagements ........................................................................................ -
Canberra's Influence on the Surrounding NSW Economic And
Canberra’s Influence on the Surrounding NSW Economic and Housing Markets Final Report - October 2015 Prepared for the NSW Department of Planning and Environment This report has been prepared for the NSW Department of Planning and Environment. SGS Economics and Planning has taken all due care in the preparation of this report. However, SGS and its associated consultants are not liable to any person or entity for any damage or loss that has occurred, or may occur, in relation to that person or entity taking or not taking action in respect of any representation, statement, opinion or advice referred to herein. SGS Economics and Planning Pty Ltd ACN 007 437 729 www.sgsep.com.au Offices in Canberra, Hobart, Melbourne and Sydney TABLE OF CONTENTS EXECUTIVE SUMMARY 1 Objective 1 Demographic context 1 Impact of the ACT on housing markets in surrounding NSW 1 Dwelling Types 2 Economic and employment factors impacting housing markets over time 4 Employment and Economic Growth in the SE and Tablelands Region 5 Economic Growth Opportunities 5 Economic Growth Challenges 6 Recommendations 7 1 INTRODUCTION 9 1.1 Background to the project 9 1.2 Objectives 10 1.3 History of the Australian Capital Territory 11 1.4 Broader demographic changes 11 1.5 Population in the ACT and adjacent areas of NSW 13 1.6 Impact of the ACT on New South Wales 14 1.7 Findings from previous reports 14 2 EMPLOYMENT AND POPULATION MOVEMENTS 16 2.1 ACT workers living in NSW 16 2.2 Migration of people between the ACT and surrounding NSW 16 2.3 Population ageing 22 3 HOUSING MARKETS -
Australia 2019 Crime & Safety Report: Canberra
Australia 2019 Crime & Safety Report: Canberra This is an annual report produced in conjunction with the Regional Security Office at the U.S. Embassy in Canberra, Australia. The current U.S. Department of State Travel Advisory at the date of this report’s publication assesses Australia at Level 1, indicating travelers should exercise normal precautions. Overall Crime and Safety Situation The U.S. Embassy in Canberra does not assume responsibility for the professional ability or integrity of the persons or firms appearing in this report. The American Citizens Services (ACS) unit cannot recommend a particular individual or establishment, and assumes no responsibility for the quality of services provided. Review OSAC’s Australia page for original OSAC reporting, consular messages, and contact information, some of which may be available only to private-sector representatives with an OSAC password. Crime Threats There is minimal risk from crime in Canberra. Property crimes, such as burglary, breaking and entering, and theft, occur throughout Australia and are among the crimes most likely to be encountered by Australians and foreigners alike. Physical assaults are relatively uncommon, but occur with greater frequency in specific locales, predominantly outside of the city center. Crime in the central business district includes illegal recreational drug use and associated behavior, particularly after midnight. According to the Australian Bureau of Statistics 2017-18 National Crime Victimization Survey, the personal and household crime most frequently experienced by Australians was face-to-face threatened assault (2.6%), followed by physical assault (2.4%), non-face-to-face threatened assault (0.8%), and robbery (0.3%); the latter two categories are down from 2016-2017. -

Continued Public Ownership of Snowy Hydro Limited
LEGISLATIVE COUNCIL Select Committee on the continued public ownership of Snowy Hydro Limited Continued public ownership of Snowy Hydro Limited Ordered to be printed 26 October 2006 Report - October 2006 LEGISLATIVE COUNCIL Continued public ownership of Snowy Hydro Limited New South Wales Parliamentary Library cataloguing-in-publication data: New South Wales. Parliament. Legislative Council. Select Committee on the continued public ownership of Snowy Hydro Limited. The continued public ownership of Snowy Hydro Limited : [report] / Legislative Council, Select Committee on the continued public ownership of Snowy Hydro Limited. [Sydney, N.S.W.] : The Committee, 2006. – 105 p. ; 30 cm. (Report) “October 2006”. Chair: Rev. the Hon. Dr. Gordon Moyes, MLC. ISBN 1921286059 1. Snowy Mountains Hydro-Electric Authority. 2. Hydroelectric power plants--New South Wales--Snowy Mountains. I. Moyes, Gordon. II. Title III. Series: New South Wales. Parliament. Legislative Council. Select Committee on the continued public ownership of Snowy Hydro Limited. Report. DDC 621.312 ii Report - October 2006 SELECT COMMITTEE ON THE CONTINUED PUBLIC OWNERSHIP OF SNOWY HYDRO LIMITED How to contact the committee Members of the Select Committee on the continued public ownership of Snowy Hydro Limited can be contacted through the Committee Secretariat. Correspondence and enquiries should be directed to: The Director Select Committee on the continued public ownership of Snowy Hydro Limited Legislative Council Parliament House, Macquarie Street Sydney New South Wales 2000 Internet: www.parliament.nsw.gov.au/snowyhydro Email: [email protected] Telephone: 02 9230 3544 Facsimile: 02 9230 3416 Report - October 2006 iii LEGISLATIVE COUNCIL Continued public ownership of Snowy Hydro Limited Terms of reference 1. -

Legislative Assembly
21380 LEGISLATIVE ASSEMBLY Thursday 9 March 2006 ______ Mr Speaker (The Hon. John Joseph Aquilina) took the chair at 10.00 a.m. Mr Speaker offered the Prayer. Mr SPEAKER: I acknowledge the Gadigal clan of the Eora nation and their elders and thank them for the custodianship of this land. ROYAL REHABILITATION CENTRE SYDNEY SITE PROTECTION BILL Second Reading Debate resumed from 2 March 2006. Mr ANTHONY ROBERTS (Lane Cove) [10.02 a.m.]: It is with great pride that I once again today stand shoulder to shoulder with my residents and community in protecting my electorate from gross overdevelopment. As I stated last week, we have more than 2,500 signatures on petitions opposing this overdevelopment and thousands have marched in my electorate and other electorates protesting against this proposal. I must pay particular tribute to each and every one of those people in Putney and surrounding areas who have supported our plight in an area that is becoming the target of more and more overdevelopment. The area is already suffering from extensive infrastructure and traffic problems. So far it has been able to maintain an appropriate level of housing. However, once again, we are confronting a proposal from a greedy developer to turn one of the most magnificent areas of Sydney—in fact, of the country—into something reminiscent of the inner city. I pay tribute particularly to Rolf Clapham of the Coalition Against Private Overdevelopment [CAPO], Graham Clift, Ted Webber, Susan Macgregor, Eleanor Chaine, Simone Chaine, Rona Agnew, Simone Galvin and Kylie Rennie for their assistance and leadership in this matter. -
AR JACS 02 03Part1.Pdf
annual report ACT Department of Justice & Community Safety ANNUAL REPORT 2002 – 2003 Australian Capital Territory Government www.jcs.act.gov.au volume 1 Mr Jon Stanhope MLA Attorney General ACT Legislative Assembly London Circuit CANBERRA ACT 2600 Dear Attorney General I am pleased to present the Annual Report of the Department of Justice and Community Safety for the year ended 30 June 2003. This Report has been prepared under section 7(1) of the Annual Reports (Government Agencies) Act 1995 and in accordance with the requirements referred to in the Chief Minister’s Annual Reports Directions. It has been prepared in conformity with other legislation applicable to the preparation of the Annual Report by the Department of Justice and Community Safety. I hereby certify that the attached Annual Report is an honest and accurate account and that all material information on the operations of the Department of Justice and Community Safety during the period 1 July 2002 to 30 June 2003 has been included and that it complies with the Chief Minister’s Annual Reports Directions. Yours sincerely Tim Keady Chief Executive 5 September 2003 2 ANNUAL REPORT 2002 – 2003 ACT Department of Justice & Community Safety Mr Bill Wood MLA Minister for Police and Emergency Services ACT Legislative Assembly London Circuit CANBERRA ACT 2600 Dear Minister I am pleased to present the Annual Report of the Department of Justice and Community Safety for the year ended 30 June 2003. This Report has been prepared under section 7(1) of the Annual Reports (Government Agencies) Act 1995 and in accordance with the requirements referred to in the Chief Minister’s Annual Report Directions. -

ANNUAL REPORT 06SERVICE ONE CREDIT UNION LTD 07 Contents
ANNUAL REPORT 06SERVICE ONE CREDIT UNION LTD 07 CONTENTS 3 Vision, Mission and Values 4 In the Community 11 Corporate Directory 12 Message from the Chair 16 Directors 18 Corporate Governance Statement 24 Directors’ Report 28 Financial Report 61 Directors’ Declaration 62 Independent Audit Report 1 vision To be the first choice banking institution for those living in the ACT and South Eastern NSW. mission To excel at providing banking and financial services. values We care about each other and behave as a supportive family would behave. The conduct of our business and ourselves shows others what kind of organisation we are and is demontrated by the following values: • We are respectful and courteous • We are tolerant and supportive • We are honest and open • We are dependable and accountable • We are prudent and ethical. 2 3 IN THE COMMUNITY SERVICE ONE Members Banking is proud to support community events and organisations within our region. Some of the events and organisations we have supported over the past 12 months include: ACT Cancer Society Carers Charity Bowls Day Sids and Kids ACT Eden Monaro Cancer Cooma Show Snowy Hydro SouthCare Support Helicopter Service Cooma Cats Australian Rules ACT Tennis Football Club Snowy Hydro Driver Education Australian National University Cooma Lions Club Snowy River Festival (ANU) Dalgety Show Southern NSW Health Seminar Batemans Bay Baby Dream and Achieve Special Children’s Christmas Competition Party Gadara P&C Special School Batemans Bay Orchid and Summer in the Capital Foliage Society Heart to -

About the John James Foundation Our Mission
About the John James Foundation The John James Foundation is a The Foundation is now an independent not-for-profit organisation. It built what broad based healthcare charity providing is now the Calvary John James Hospital a range of programs and assistance to in 1970 and operated it until 2006 when the people of Canberra and beyond. the hospital business was sold to Calvary The Foundation is grateful for the Private Healthcare Canberra. Following ongoing support of the large number of the sale of the business, the Foundation Canberra based Medical Specialists who retained ownership of all of the hospital are the members of the Foundation. land and buildings which form the John James Healthcare Campus. Our Mission To be recognised widely as a leading charitable healthcare organisation through the provision of specialist medical facilities support and services to those in need. Contact Us John James Memorial Foundation Ltd ABN: 25 008 453 469 Suite 1 Level 2 Peter Yorke Building John James Healthcare Campus 173 Strickland Crescent DEAKIN ACT 2600 Our Cover PO Box 23 John James Foundation has quite a fleet of DEAKIN WEST ACT 2600 “vehicles”, through donations provided under the Foundation’s Community Health Program, with Tel: 02 6281 6695 each vehicle showing the Foundation’s logo as a Fax: 02 6282 9973 supporter of that cause. Pictured on the cover, Email: [email protected] from left to right are: Web: www.jjmf.org.au Nathalie Maconachie, CEO SIDS and Kids ACT Owen Finegan, CEO Our Patron Snowy Hydro SouthCare His Excellency General Martine Parsons, volunteer driver The Honourable Sir Peter Cosgrove AK MC (Retd) SIDS and Kids ACT Phil Greenwood, CEO Staff John James Foundation Mr Phil Greenwood (CEO) Rick Smyth, volunteer driver Palliative Care ACT Mrs Stephanie Burgess (Finance Manager) Susan Fisher, Business Development Manager Ms Karryn Smith (Administration Manager) Leukaemia Foundation ACT Ms Jane Smith (Writer) From the Chairman Prof Paul N.