Spontaneous Spinal Cerebrospinal Fluid Leaks: a Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Spatially Heterogeneous Choroid Plexus Transcriptomes Encode Positional Identity and Contribute to Regional CSF Production
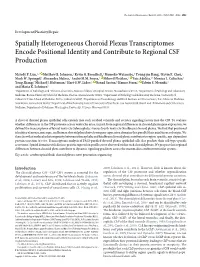
The Journal of Neuroscience, March 25, 2015 • 35(12):4903–4916 • 4903 Development/Plasticity/Repair Spatially Heterogeneous Choroid Plexus Transcriptomes Encode Positional Identity and Contribute to Regional CSF Production Melody P. Lun,1,3 XMatthew B. Johnson,2 Kevin G. Broadbelt,1 Momoko Watanabe,4 Young-jin Kang,4 Kevin F. Chau,1 Mark W. Springel,1 Alexandra Malesz,1 Andre´ M.M. Sousa,5 XMihovil Pletikos,5 XTais Adelita,1,6 Monica L. Calicchio,1 Yong Zhang,7 Michael J. Holtzman,7 Hart G.W. Lidov,1 XNenad Sestan,5 Hanno Steen,1 XEdwin S. Monuki,4 and Maria K. Lehtinen1 1Department of Pathology, and 2Division of Genetics, Boston Children’s Hospital, Boston, Massachusetts 02115, 3Department of Pathology and Laboratory Medicine, Boston University School of Medicine, Boston, Massachusetts 02118, 4Department of Pathology and Laboratory Medicine, University of California Irvine School of Medicine, Irvine, California 92697, 5Department of Neurobiology and Kavli Institute for Neuroscience, Yale School of Medicine, New Haven, Connecticut 06510, 6Department of Biochemistry, Federal University of Sa˜o Paulo, Sa˜o Paulo 04039, Brazil, and 7Pulmonary and Critical Care Medicine, Department of Medicine, Washington University, St Louis, Missouri 63110 A sheet of choroid plexus epithelial cells extends into each cerebral ventricle and secretes signaling factors into the CSF. To evaluate whether differences in the CSF proteome across ventricles arise, in part, from regional differences in choroid plexus gene expression, we defined the transcriptome of lateral ventricle (telencephalic) versus fourth ventricle (hindbrain) choroid plexus. We find that positional identitiesofmouse,macaque,andhumanchoroidplexiderivefromgeneexpressiondomainsthatparalleltheiraxialtissuesoforigin.We thenshowthatmolecularheterogeneitybetweentelencephalicandhindbrainchoroidplexicontributestoregion-specific,age-dependent protein secretion in vitro. -

Human Cerebrospinal Fluid Induces Neuronal Excitability Changes in Resected Human Neocortical and Hippocampal Brain Slices
bioRxiv preprint doi: https://doi.org/10.1101/730036; this version posted August 8, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-ND 4.0 International license. Human cerebrospinal fluid induces neuronal excitability changes in resected human neocortical and hippocampal brain slices Jenny Wickham*†1, Andrea Corna†1,2,3, Niklas Schwarz4, Betül Uysal 2,4, Nikolas Layer4, Thomas V. Wuttke4,5, Henner Koch4, Günther Zeck1 1 Neurophysics, Natural and Medical Science Institute (NMI) at the University of Tübingen, Reutlingen, Germany 2 Graduate Training Centre of Neuroscience/International Max Planck Research School, Tübingen, Germany. 3 Institute for Ophthalmic Research, University of Tübingen, Tübingen, Germany 4 Department of Neurology and Epileptology, Hertie-Institute for Clinical Brain Research, University of Tübingen, Tübingen, Germany 5 Department of Neurosurgery, University of Tübingen, Tübingen, Germany * Communicating author: Jenny Wickham ([email protected]) and Günther Zeck ([email protected]) † shared first author, Shared last author Acknowledgments: This work was supported by the German Ministry of Science and Education (BMBF, FKZ 031L0059A) and by the German Research Foundation (KO-4877/2-1 and KO 4877/3- 1) Author contribution: JW and AC performed micro-electrode array recordings, NS, BU, NL, TW, HK and JW did tissue preparation and culturing, JW, AC, GZ did data analysis and writing. Proof reading and study design: all. Conflict of interest: None Keywords: Human tissue, human cerebrospinal fluid, Microelectrode array, CMOS-MEA, hippocampus, cortex, tissue slice 1 bioRxiv preprint doi: https://doi.org/10.1101/730036; this version posted August 8, 2019. -

The Diagnosis of Subarachnoid Haemorrhage
Journal ofNeurology, Neurosurgery, and Psychiatry 1990;53:365-372 365 J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.53.5.365 on 1 May 1990. Downloaded from OCCASIONAL REVIEW The diagnosis of subarachnoid haemorrhage M Vermeulen, J van Gijn Lumbar puncture (LP) has for a long time been of 55 patients with SAH who had LP, before the mainstay of diagnosis in patients who CT scanning and within 12 hours of the bleed. presented with symptoms or signs of subarach- Intracranial haematomas with brain shift was noid haemorrhage (SAH). At present, com- proven by operation or subsequent CT scan- puted tomography (CT) has replaced LP for ning in six of the seven patients, and it was this indication. In this review we shall outline suspected in the remaining patient who stop- the reasons for this change in diagnostic ped breathing at the end of the procedure.5 approach. In the first place, there are draw- Rebleeding may have occurred in some ofthese backs in starting with an LP. One of these is patients. that patients with SAH may harbour an We therefore agree with Hillman that it is intracerebral haematoma, even if they are fully advisable to perform a CT scan first in all conscious, and that withdrawal of cerebro- patients who present within 72 hours of a spinal fluid (CSF) may occasionally precipitate suspected SAH, even if this requires referral to brain shift and herniation. Another disadvan- another centre.4 tage of LP is the difficulty in distinguishing It could be argued that by first performing between a traumatic tap and true subarachnoid CT the diagnosis may be delayed and that this haemorrhage. -

Non-Traumatic Cerebrospinal Fluid Rhinorrhoea
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.31.3.214 on 1 June 1968. Downloaded from J. Neurol. Neurosurg. Psychiat., 1968, 31, 214-225 Non-traumatic cerebrospinal fluid rhinorrhoea AYUB K. OMMAYA, GIOVANNI DI CHIRO, MAITLAND BALDWIN, AND J. B. PENNYBACKERI From the Branches ofMedical Neurology and ofSurgical Neurology, National Institute ofNeurological Diseases and Blindness, National Institutes ofHealth, Public Health Service, United States Department of Health, Education and Welfare, Bethesda, Maryland, U.S.A. There is a certain degree of confusion in the litera- ally impossible phrase 'secondary spontaneous ture concerning nasal leakage of cerebrospinal fluid rhinorrhcea'. when trauma is not the cause. The term 'spontaneous In an earlier report by one of us (A.K.O.), an cerebrospinal fluid rhinorrhoea' has been usedmore or attempt was made to provide such a classification of less consistently to describe such cases since 1899. cerebrospinal fluid rhinorrhoea on the basis of an Although isolated observations had been made analysis of the literature and the case histories of two earlier, it was the monograph by St. Clair Thomson patients (Ommaya, 1964). Since then we have been (1899) that first clearly described and atttempted to able to collect 18 patients with non-traumatic define spontaneous cerebrospinal fluid rhinorrhcea as cerebrospinal fluid rhinorrhoea. Thirteen of these a clinical entity. Other authors have since essayed to were seen at the Radcliffe Infirmary, Oxford, andProtected by copyright. subdivide this condition into 'primary spontaneous' five at the National Institute ofNeurological Diseases or 'idiopathic' rhinorrhoea when a precipitating cause and Blindness, National Institutes of Health, could not be found and 'secondary spontaneous' Bethesda, Maryland. -

Cerebrospinal Fluid in Critical Illness
Cerebrospinal Fluid in Critical Illness B. VENKATESH, P. SCOTT, M. ZIEGENFUSS Intensive Care Facility, Division of Anaesthesiology and Intensive Care, Royal Brisbane Hospital, Brisbane, QUEENSLAND ABSTRACT Objective: To detail the physiology, pathophysiology and recent advances in diagnostic analysis of cerebrospinal fluid (CSF) in critical illness, and briefly review the pharmacokinetics and pharmaco- dynamics of drugs in the CSF when administered by the intravenous and intrathecal route. Data Sources: A review of articles published in peer reviewed journals from 1966 to 1999 and identified through a MEDLINE search on the cerebrospinal fluid. Summary of review: The examination of the CSF has become an integral part of the assessment of the critically ill neurological or neurosurgical patient. Its greatest value lies in the evaluation of meningitis. Recent publications describe the availability of new laboratory tests on the CSF in addition to the conventional cell count, protein sugar and microbiology studies. Whilst these additional tests have improved our understanding of the pathophysiology of the critically ill neurological/neurosurgical patient, they have a limited role in providing diagnostic or prognostic information. The literature pertaining to the use of these tests is reviewed together with a description of the alterations in CSF in critical illness. The pharmacokinetics and pharmacodynamics of drugs in the CSF, when administered by the intravenous and the intrathecal route, are also reviewed. Conclusions: The diagnostic utility of CSF investigation in critical illness is currently limited to the diagnosis of an infectious process. Studies that have demonstrated some usefulness of CSF analysis in predicting outcome in critical illness have not been able to show their superiority to conventional clinical examination. -

ICD-10 Coordination and Maintenance Committee Meeting Diagnosis Agenda March 5-6, 2019 Part 2
ICD-10 Coordination and Maintenance Committee Meeting Diagnosis Agenda March 5-6, 2019 Part 2 Welcome and announcements Donna Pickett, MPH, RHIA Co-Chair, ICD-10 Coordination and Maintenance Committee Diagnosis Topics: Contents Babesiosis ........................................................................................................................................... 10 David, Berglund, MD Mikhail Menis, PharmD, MS Epi, MS PHSR Epidemiologist Office of Biostatistics and Epidemiology CBER/FDA C3 Glomerulopathy .......................................................................................................................... 13 David Berglund, MD Richard J. Hamburger, M.D. Professor Emeritus of Medicine, Indiana University Renal Physicians Association Eosinophilic Gastrointestinal Diseases ............................................................................................ 18 David Berglund, MD Bruce Bochner, MD Samuel M. Feinberg Professor of Medicine Northwestern University Feinberg School of Medicine and President, International Eosinophil Society ICD-10 Coordination and Maintenance Committee Meeting March 5-6, 2019 Food Insecurity.................................................................................................................................. 20 Donna Pickett Glut1 Deficiency ................................................................................................................................ 23 David Berglund, MD Hepatic Fibrosis ............................................................................................................................... -
Thunderclap Headache and Subarachnoid Hemorrhage
Thunderclap Headache and Subarachnoid Hemorrhage W David Freeman, MD No conflicts of interest or disclosures Subarachnoid Hemorrhage Neurocrit Care. 2017 Sep;27(Suppl 1):116- 123. doi: 10.1007/s12028-017-0458-8. Objectives •Recognize the symptoms (thunderclap headache) and Subarachnoid signs of SAH Hemorrhage •Initiate workup for suspected SAH •Initial management of SAH patient Case • 39 year old woman presents with severe headache, uncertain time of onset, associated with nausea • PMH: long history of migraine headaches • Meds: • Reports taking ibuprofen prior to ED, with moderate improvement of headache • Taking warfarin for a pelvic DVT - year prior during pregnancy • Exam: sleepy, yet follows commands, left eye droop and dilated pupil, moving all extremities • BP 160/95 mmHg, RR 24/min, HR 98/min • Breathing shallow and rapid, airway protection uncertain Initial Checklist in Emergency Dept. ☐ Brain Imaging ☐ Labs: PT/PTT, CBC, electrolytes, BUN, Cr, troponin, toxicology screen ☐ 12 lead ECG ☐ Blood pressure goal established ☐ Consult neurosurgery ☐ Address hydrocephalus SAH Algorithm Neurocrit Care. 2017 Sep;27(Suppl 1):116- 123. doi: 10.1007/s12028-017-0458-8. SAH Symptoms and Signs CLASSIC NOT-SO-CLASSIC Abrupt onset of severe headache (HA), HA is not reported as abrupt (patient may i.e. thunderclap not remember event well) “Worst or first” headache of one’s life HA responds well to non-narcotic that is instantaneously maximal at onset analgesics (“thunderclap” after lightening strike) May have nausea, vomiting and neck pain HA -

Hypothesis on the Pathophysiology of Syringomyelia Based on Simulation of Cerebrospinal Fluid Dynamics H S Chang, H Nakagawa
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.74.3.344 on 1 March 2003. Downloaded from 344 PAPER Hypothesis on the pathophysiology of syringomyelia based on simulation of cerebrospinal fluid dynamics H S Chang, H Nakagawa ............................................................................................................................. J Neurol Neurosurg Psychiatry 2003;74:344–347 See end of article for authors’ affiliations ....................... Objectives: Despite many hypotheses, the pathophysiology of syringomyelia is still not well Correspondence to: understood. In this report, the authors propose a hypothesis based on analysis of cerebrospinal fluid Dr H S Chang, Department of Neurological Surgery, dynamics in the spine. Aichi Medical University, Methods: An electric circuit model of the CSF dynamics of the spine was constructed based on a tech- 21 Yazako-Karimata, nique of computational fluid mechanics. With this model, the authors calculated how a pulsatile CSF Nagakute-cho, Aichi-gun, wave coming from the cranial side is propagated along the spinal cord. Aichi 480–1195, Japan; Results: Reducing the temporary fluid storage capacity of the cisterna magna dramatically increased [email protected] the pressure wave propagated along the central canal. The peak of this pressure wave resided in the Received 14 June 2002 mid-portion of the spinal cord. In final revised form Conclusions: The following hypotheses are proposed. The cisterna magna functions as a shock 11 November 2002 Accepted absorber against the pulsatile CSF waves coming from the cranial side. The loss of shock absorbing 21 November 2002 capacity of the cisterna magna and subsequent increase of central canal wall pressure leads to syrinx ....................... formation in patients with Chiari I malformation. -

Spinal Cerebrospinal Fluid Leak As the Cause of Chronic Subdural Hematomas in Nongeriatric Patients
J Neurosurg 121:1380–1387, 2014 ©AANS, 2014 Spinal cerebrospinal fluid leak as the cause of chronic subdural hematomas in nongeriatric patients Clinical article JÜRGEN BECK, M.D.,1 JAN GRALLA, M.D., M.SC.,2 CHRISTIAN FUNG, M.D.,1 CHRISTIAN T. ULRICH, M.D.,1 PHILIppE SCHUCHT, M.D.,1 JENS FICHTNER, M.D.,1 LUKAS ANDEREGGEN, M.D.,1 MARTIN GOSAU, M.D.,4 ELKE HATTINGEN, M.D.,5 KLEMENS GUTBROD, M.D.,3 WERNER J. Z’GRAGGEN, M.D.,1,3 MICHAEL REINERT, M.D.,1,6 JÜRG HÜSLER, PH.D.,7 CHRISTOPH OzdOBA, M.D.,2 AND ANDREAS RAABE, M.D.1 Departments of 1Neurosurgery, 2Neuroradiology, and 3Neurology, Bern University Hospital, Bern, Switzerland; 4Department of Cranio-Maxillo-Facial Surgery, University Medical Center, Regensburg, Germany; 5Institute of Neuroradiology, University of Frankfurt, Frankfurt/Main, Germany; 6Department of Neurosurgery, Ospedale Cantonale di Lugano, Switzerland; and 7Institute of Mathematical Statistics and Actuarial Science, University of Bern, Switzerland Object. The etiology of chronic subdural hematoma (CSDH) in nongeriatric patients (≤ 60 years old) often re- mains unclear. The primary objective of this study was to identify spinal CSF leaks in young patients, after formulat- ing the hypothesis that spinal CSF leaks are causally related to CSDH. Methods. All consecutive patients 60 years of age or younger who underwent operations for CSDH between September 2009 and April 2011 at Bern University Hospital were included in this prospective cohort study. The pa- tient workup included an extended search for a spinal CSF leak using a systematic algorithm: MRI of the spinal axis with or without intrathecal contrast application, myelography/fluoroscopy, and postmyelography CT. -

Hydrocephalus Patient Information Guide Experience Life Without Boundaries
Hydrocephalus Patient Information Guide Experience Life Without Boundaries Aesculap Neurosurgery 2 Table of Contents Foreword Page 4 About Us Page 5 What Is Hydrocephalus Page 6 Types Of Hydrocephalus Page 7 What You Should Know Page 8 Diagnosis Page 9 Treatment/Goal/Surgical Procedure Page 10 Complications Page 10 Prognosis/Helpful Sites Page 11 The Aesculap Shunts Page 12 Medical Definitions Page 13 3 Foreword The intention of this booklet is to provide information to patients, family members, caregivers and friends on the subject of hydrocephalus. The information provided is a general overview of the diagnosis and treatment of hydrocephalus and other conditions associated with hydrocephalus. About us History Aesculap AG (Germany) was founded in 1867 by Gottfried Jetter, a master craftsman trained in surgical instrument and cutlery techniques. Jetter’s original workshop, located in Tuttlingen, Germany, is the same location where Aesculap world headquarters resides today. The employee count has increased over the years (3,000+ employees), and the number of instrument patterns has grown from a select few to over 17,000; however, the German standard for quality and pattern consistency remains the same. Prior to 1977, many of the instruments sold in America by competing companies were sourced from Aesculap in Tuttlingen. In response to the United States customer demand for Aesculap quality surgical instruments, Aesculap, Inc. (U.S.) was established in 1977. Headquartered in Center Valley, Pennsylvania, with over one hundred direct nationwide sales representatives, Aesculap, Inc. currently supports the marketing, sales and distribution of Aesculap surgical instrumentation in the U.S. In order to support the company’s continued growth and provide the service and quality which customers have come to expect, Aesculap relocated the corporate offices from San Francisco to Center Valley, Pennsylvania. -

Effect of Methemoglobin Formation on the MR Appearance of Subarachnoid Hemorrhage1
William G. Bradley, Jr., M.D., Ph.D. Effect of Methemoglobin Formation Paul G. Schmidt, Ph.D. on the MR Appearance of Subarachnoid Hemorrhage1 Subarachnoid hemorrhage has a much T HE EARLIEST reports of magnetic resonance (MR) images of in- higher intensity in magnetic resonance tracranial hemorrhage (1, 2) suggested a relatively intense ap- (MR) images with the passage of time. peanance of the hemorrhage relative to the surrounding brain. This Acute subarachnoid hemorrhage is diff i- was attributed to the short Ti relaxation time of the presumably cult to see; within 1 week its appearance paramagnetic, iron-containing hemoglobin. Figure 1 illustrates this has become intensified on Ti-weighted appearance in a patient imaged 1 week after rupture of an aneurysm images. Different concentrations of blood in an anterior communicating artery, with resulting intraparenchy- and lysed red blood cells in cerebrospinal mal hematoma and subarachnoid hemorrhage. The short Ti charac- fluid (CSF) were examined spectroscopi- ten of the injured area is enhanced relative to surrounding brain on cally but did not significantly alter Ti a Ti-weighted spin-echo image. and T2 relaxation of CSF acutely. Ultra- As experience was gained, subsequent reports (3, 4) indicated violet visible spectroscopy of bloody CSF that acute intracranial hemorrhage could be much more difficult to stored hypoxically for 3 days showed the detect on MR images. This was attributed by Sipponen et al. (3) to a presence of methemoglobin. The iron in lack of Ti shortening during the acute phase; however, they at- methemoglobin is paramagnetic; in com- tempted no explanation of this phenomenon. -
D40. Cerebrospinal Fluid.Pdf
CEREBROSPINAL FLUID D40 (1) Cerebrospinal Fluid (CSF) Last updated: June 3, 2019 PHYSIOLOGY ............................................................................................................................................ 1 CSF PRODUCTION .................................................................................................................................. 1 CSF REABSORPTION ............................................................................................................................... 1 PARAMETERS ........................................................................................................................................... 2 NORMAL ................................................................................................................................................ 2 OPENING PRESSURE ................................................................................................................................ 3 COLOR ................................................................................................................................................... 3 BLOODY CSF ......................................................................................................................................... 3 VISCOSITY & TURBIDITY ....................................................................................................................... 4 CELLS ...................................................................................................................................................