Rotator Cuff Tendon Problems Patient Information Anatomy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Shoulder Injuries: Dislocated Shoulder and Labral Tear
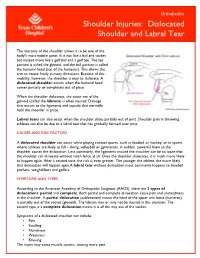
Orthopedics Shoulder Injuries: Dislocated Shoulder and Labral Tear The anatomy of the shoulder allows it to be one of the body's most mobile joints. It is not like a ball and socket but instead more like a golf ball and a golf tee. The tee portion is called the glenoid, and the ball portion is called the humeral head (top of the humerus). This allows the arm to rotate freely in many directions. Because of this mobility, however, the shoulder is easy to dislocate. A dislocated shoulder occurs when the humeral head comes partially or completely out of place. When the shoulder dislocates, the outer rim of the glenoid (called the labrum) is often injured. Damage also occurs to the ligaments and capsule that normally hold the shoulder in place. Labral tears can also occur when the shoulder slides partially out of joint. Shoulder pain in throwing athletes can also be due to a labral tear that has gradually formed over time. CAUSES AND RISK FACTORS A dislocated shoulder can occur while playing contact sports, such as football or hockey, or in sports where athletes are likely to fall – skiing, volleyball or gymnastics. A sudden, powerful blow to the shoulder causes the dislocation. Less commonly, the ligaments around the shoulder can be so loose that the shoulder can dislocate without much force at all. Once the shoulder dislocates, it is much more likely to happen again. After a second time, the risk is even greater. The younger the athlete, the more likely that dislocation will happen again.A labral tear without dislocation most commonly happens to baseball pitchers, weightlifters and golfers. -
Dislocated Shoulder -Orthoinfo - AAOS Page 1 of 2
Dislocated Shoulder -OrthoInfo - AAOS Page 1 of 2 Dislocated Shoulder The shoulder joint is the body's most mobile joint. It can turn in many directions. But, this advantage also makes the shoulder an easy joint to dislocate. A partial dislocation (subluxation) means the head of the upper arm bone (humerus) is partially out of the socket (glenoid). A complete dislocation means it is all the way out of the socket. Both partial and complete dislocation cause pain and unsteadiness in the shoulder. Shoulder instability Symptoms Symptoms to look for include: • Swelling • Numbness • Weakness • Bruising Sometimes dislocation may tear ligaments or tendons in the shoulder or damage nerves. The shoulder joint can dislocate forward, backward, or downward. A common type of shoulder dislocation is when the shoulder slips forward (anterior instability). This means the upper arm bone moved forward and down out of its joint. It may happen when the arm is put in a throwing position. Diagnosis The muscles may have spasms from the disruption, and this can make it hurt more. When the shoulder dislocates time and again, there is shoulder instability. The doctor will examine the shoulder and may order an X-ray. It is important that the doctor know how the dislocation happened and whether the shoulder had ever been dislocated before. Treatment http://orthoinfo.aaos.org/topic.cfm?topic=A00035 2/2/2015 Dislocated Shoulder -OrthoInfo - AAOS Page 2 of 2 The doctor will place the ball of the upper arm bone (humerus) back into the joint socket. This process is called closed reduction. Severe pain stops almost immediately once the shoulder joint is back in place. -

Sports Injuries
Sports Injuries Lacrosse Lacrosse is America’s oldest game. It can be dated back to the Native Americans, and was used astraining for war. It is both played by boys and girls,however, some rules are drastically different between genders. Nonetheless, the combination of contact, a stick, a hard ball, and quick changes of direction, puts lacrosse players at risk for injury. Protective Equipment There is a wide range of equipment that lacrosse players wear. For girls, goggles and mouth pieces are mandatory. Lightweight gloves and headgear is optional. For boys, helmets with full face guards, shoulder pads, padded gloves, and mouth pieces are used. It is most important for this equipment to fit properly. If equipment does not fit properly it can actually cause injury. There is no helmet which has been proven through research that confused with a “dislocated shoulder,” which is when prevents concussions. the shoulder comes out of socket. Dislocated shoulders What are the most common types are not common in lacrosse. of lacrosse injuries? Concussions Contusions Concussions are quite common in lacrosse. For more information, please refer to our concussion handout. Because of the nature of the sport, bruises or contusions are very common in lacrosse. Contusions How can lacrosse injuries be prevented? are best initially treated with ice, compression, and elevation of the affected area. • Stay active year round Knee Injuries • Incorporate strength training and stretching into your normal routine Lacrosse players commonly injure their knees. Sprains of the medial and lateral collateral ligaments • Wear properly fitted equipment (MCL/LCL) occur. More serious injuries of the anterior and posterior cruciate ligaments (ACL/PCL) and to the • Hydrate adequately before, during, and menisci (cartilage of the knee) can also happen. -

Shoulder Pain Advice and Exercises
Shoulder Pain Advice and Exercises 0523 - Oct 2018 (v1.2) April 2018 April 2021 Please note that if your shoulder pain started after a recent trauma please Simple Exercises contact your GP. Please complete all exercises below as your symptoms allow; aim for no more than 10-15 repetitions of each exercise, 2-3 times a day. Some exercises may cause This booklet has been produced by senior physiotherapists working for discomfort but should not cause significant pain. If your symptoms are not DynamicHealth. It offers simple advice and exercises to help you safely manage improving in 6 - 8 weeks or are worsening please call our Physio Advice Line for your shoulder problem, often the right advice and exercises are all that is needed. further support on 0300 555 0210. This leaflet has been made available to your GP, who may ask you to try the advice and exercises prior to physiotherapy assistance. About the Shoulder A. Shoulder Rolls The shoulder is the most mobile joint in the body. The main shoulder joint is a 1. Sit or stand. ball and socket joint, which allows a wide range of movement. The joint is surrounded by a tough fibrous sleeve called the capsule, which helps to support 2. Roll your shoulders backwards. the joint. A group of four muscles and their tendons make up the rotator cuff, which 3. Repeat up to 10-15 times. Frequency: 2-3 times per day. controls movement and also helps to support the joint. There’s another smaller joint where the top of the shoulder blade meets the collarbone. -

Shoulder Pain: Differential Diagnosis with Mechanical Diagnosis and Therapy Extremity Assessment E a Case Report
Manual Therapy 18 (2013) 354e357 Contents lists available at SciVerse ScienceDirect Manual Therapy journal homepage: www.elsevier.com/math Case report Shoulder pain: Differential diagnosis with mechanical diagnosis and therapy extremity assessment e A case report A. Menon a,S.Mayb,* a Shri Giridhari Physical Therapy Center, Mumbai, India b Faculty of Health and Wellbeing, 38 Collegiate Crescent Campus, Sheffield Hallam University, Sheffield S10 2BP, UK article info abstract Article history: Mechanical Diagnosis and Therapy (MDT) is now probably the only non-specific classification system Received 29 May 2012 that can be used with both spinal and non-spinal patients. Derangement syndrome, which presents with Received in revised form rapid changes in symptoms or mechanical response with the use of repeated movements, appears to be 20 June 2012 common in both spinal and extremity cases. Shoulder problems can be attributed to specific shoulder Accepted 26 June 2012 problems, but may also be referred from the neck. The case report describes a patient presenting with shoulder pain and limitations to shoulder function, and who tested positive to functional shoulder tests. Keywords: However, repeated neck movements demonstrated the ability to worsen and improve the shoulder pain McKenzie ‘ ’ Mechanical diagnosis and therapy and limitations. MDT was an effective tool at making the differential diagnosis between genuine and Shoulder referred shoulder pain. Classification Ó 2012 Elsevier Ltd. All rights reserved. 1. Introduction prognosis and facilitates research (Long et al., 2004; Cook et al., 2005). Shoulder pain is reported to be the most common musculo- The McKenzie Method of Mechanical Diagnosis and Therapy skeletal disorder after spinal pain (Eltayeb et al., 2007). -

Shoulder Pain
Health News from Ponte Vedra Wellness Center Family Chiropractic Care in Ponte Vedra Beach & Nocatee Town Center Dr. Erika Hamer, DC, DIBCN, DIBE CHIROPRACTIC FROM HEAD TO TOE – SHOULDER PAIN he shoulder is a very unique and complex joint. It is the only articulation in the body whose stability is granted primarily by muscular balance instead of being held Ttogether by the integrity of its ligaments. Have you ever heard of the ROTATOR CUFF? This is the collection of four shoulder muscles that help perform this function: namely the supraspinatus, the infraspinatus, the teres minor and subscapularis. In addition, there are multiple bones that come togeth- er to make up the shoulder joint: the humerus (upper arm), the scapula (the shoulder blade) and the clavicle (the collar bone). Therefore, problems with the align- ment of any of these bones will directly aff ect shoulder function, potentially leading to dysfunction and painful symptoms in this joint. Finally, many nerves lead to the shoulder, infl uencing motor control of the shoulder and providing sensory feedback from the shoulder to the brain. The main source of these nerves is the cervical spine (the neck). How Chiropractic Helps Shoulders So, how can your chiropractor help when you have a shoulder problem? Just like every other joint in the body, the shoulder works best when all its moving parts are in proper alignment. As you will discover below, the most important factor contributing to the proper function of the shoulder is the alignment of your spine, with each major area of the spine contributing in a signifi cant way to the health of your shoulder. -

Shoulder Dislocation
Shoulder Dislocation The human shoulder is an amazing machine. The unique us (ball) and the glenoid (socket) help prevent the anatomy of the shoulder enables the greatest range of joint from dislocating. The labrum, a firm tissue motion of any joint in the body. The shoulder allows over- that surrounds the glenoid, is another important head activities like screwing in a lightbulb and provides structure. When an injury happens, these liga- the strength to do a handstand or throw a 95-mile per ments and the labrum can be damaged, and a hour fastball. shoulder dislocation can result. Under normal circumstances, we rarely stop to think Causes about our shoulders. When an injury to the shoulder The normal shoulder joint can be thought of as a golf ball occurs, however, it often can be impossible to ignore. A balancing on a tee. If a large enough force in the right shoulder dislocation is one of those injuries. This article direction is applied to the arm, the ball will dislocate from covers the important aspects of shoulder dislocation: nor- the socket. This causes pain, and the shoulder will ap- mal anatomy, anatomy of a dislocation, diagnosis, treat- pear and feel abnormal. It will be difficult to move the ment, and future considerations after a dislocation. shoulder and arm. Sometimes the shoulder will go back into place on its own. When the shoulder will not go back Normal Anatomy of the Shoulder into place on its own, a reduction is required. This usually When most people think of the shoulder joint, the “ball involves a trip to the emergency room or other health and socket” comes to mind. -

A Miniature from the 15Th Century That Narrates Shoulder Reduction
DOI: 10.14744/ejmo.2017.46855 EJMO 2017;1(3):179-182 Letter to the Editor A Miniature From the 15th Century That Narrates Shoulder Reduction Engin Kesgin Private Antalya Medical Center, Antalya, Turkey Cite This Article: Kesgin E. A Miniature From 15th Century That Narrates Shoulder Reduction. EJMO. 2017; 1(3): 179-182 erefeddin Sabuncuoglu (1385–1470 A.D.) was a sur- gical textbook in Anatolian medicine.[2] Sgeon who lived in Amasya, which is in the northern part Sabuncuoglu was a master of Turkish, his mother lan- of middle Anatolia, in the 15th century during the period of guage. Although he knew Arabic, Greek, and Persian, he the Ottoman Empire. During his lifetime, he wrote detailed consciously wrote his book in Turkish because most phy- explanations of surgical methods and used miniatures to sicians and majority of the Anatolian public spoke Turkish demonstrate these methods. He made a significant con- at that time. The other reason was that medical books were tribution to the field of medical sciences, which included commonly written in other languages; thus, the public of the fields of obstetrics, gynecology, vascular surgery, nerve Anatolia was deprived of this knowledge in his era.[2] surgery, ophthalmology, oncology, dentistry, and plastic surgery.[1, 2] The 3rd volume of Sabuncuoglu’s manuscript’s, which deals with fractures and dislocations, includes a very de- His main book, Cerrahiyyet’ul Haniyye (Imperial Surgery), has tailed classification, definition, and treatment methods for three volumes: treatment by cauterization, surgical inter- shoulder dislocation with the inclusion of individual minia- ventions, and fractures and dislocations. -

Welcome Pack
Jing Certificate in Advanced Clinical Massage WELCOME PACK JING INSTITUTE OF ADVANCED MASSAGE TRAINING PO BOX 5291, BRIGHTON BN50 8AG l VAT NO: 866374290 CONTACT US www.jingmassage.com 1 2 Table of Contents Section 1: Syllabus and summary of modules Section 2: Guidance notes for students and contract Section 3: Reading list Section 4: Notes on assessment Section 5: Structuring your study; guidelines and sample quizzes 3 4 Certificate in Advanced Clinical Massage – Student syllabus Learning Assessment Criteria Underpinning knowledge Outcome UnitIntroduction to Advanced Massage Techniques – 120 learning hours 1 1.1 Utilise 1.1.1 Evaluate Client assessment – record taking based on appropriate assessment HOPRS; basic visual assessment; range of assessment techniques based movement; pain levels techniques for on HOPRS Client communication – explanation of presenting 1.1.2 Utilise correct treatment; importance of communication & client assessment conditions techniques for feedback; basic listening & questioning based on presenting client skills; non verbal communication in HOPRS conditions assessment 1.2 Demonstrate 1.2.1 Perform all specific Techniques – effleurage; petrissage; the ability to techniques tapotement; trigger point therapy; perform all correctly on neuromuscular techniques; muscle energy specific superficial muscles technique; myofascial release including techniques 1.2.2 Perform all specific indirect and direct fascial approaches, correctly and techniques appropriately appropriately using structural integration, basics of craniosacral -

Rotator Cuff Tears
OrthoInfo Basics Rotator Cuff Tears What is a rotator cuff? One of the Your rotator cuff helps you lift your arm, rotate it, and reach up over your head. most common middle-age It is made up of muscles and tendons in your shoulder. These struc- tures cover the head of your upper arm bone (humerus). This “cuff” complaints is holds the upper arm bone in the shoulder socket. shoulder pain. Rotator cuff tears come in all shapes and sizes. They typically occur A frequent in the tendon. source of that Partial tears. Many tears do not completely sever the soft tissue. Full thickness tears. A full or "complete" tear will split the soft pain is a torn tissue into two, sometimes detaching the tendon from the bone. rotator cuff. Rotator Cuff Bursa A torn rotator cuff will Tendon Clavicle (Collarbone) Humerus weaken your shoulder. (Upper Arm) This means that many Normal shoulder anatomy. daily activities, like combing your hair or Scapula getting dressed, may (Shoulder Blade) become painful and difficult to do. Rotator Cuff Tendon A complete tear of the rotator cuff tendon. 1 OrthoInfo Basics — Rotator Cuff Tears What causes rotator cuff tears? There are two main causes of rotator cuff repeating the same shoulder motions again and tears: injury and wear. again. Injury. If you fall down on your outstretched This explains why rotator cuff tears are most arm or lift something too heavy with a jerking common in people over 40 who participate in motion, you could tear your rotator cuff. This activities that have repetitive overhead type of tear can occur with other shoulder motions. -
Sports-Related Injuries Can Occur As the Result of a Single Traumatic Event, Such As an Impact Or Fall, Or from Repeated Overuse
COMMON SPORTS INJURIES Sports-related injuries can occur as the result of a single traumatic event, such as an impact or fall, or from repeated overuse and strain on muscles, tendons, and/or ligaments. Here are a few of the most common sports injuries. BICEPS FEMORIS (LONG HEAD) PULLING YOUR LEG Strains and sprains make up the bulk of sports injuries. Strains happen when muscles or SEMITENDINOSUS tendons are overstretched or torn - if someone has a pulled muscle, that means they have a muscle strain. The most commonly strained muscles are the hamstrings. SEMIMEMBRANOSUS Strains are best prevented by proper stretching, strengthening, and proper warm-ups before athletic activity. 2 SPRAIN, SPRAIN GO AWAY ANTERIOR TALOFIBULAR LIGAMENT Sprains happen when ligaments (PARTIALLY TORN) are overstretched or torn. Sprained ankles often happen when a fall or awkward landing from a jump forces the ankle joint to move in an unusual way, stressing or possibly tearing the ligaments surrounding it. Walking, running, or jumping on an uneven surface can also cause a sprained ankle. Stretching, strengthening, and balance exercises (as well as supportive footwear) can help reduce the risk of ankle sprains. 3 YOU’RE FEMUR TEARING ME APART! Many other muscles, tendons, and ligaments frequently tear. ACL (anterior cruciate ligament tears tend to happen in sports that put stress on the knees through jumping, sudden stops, and rapid changes in direction. Keeping the strength of hamstring PATELLA and quadriceps muscles balanced and (KNEECAP) TIBIA practicing safe landing and pivoting techniques can help prevent ACL tears. Factoid! Around 55% of sports-related injuries involve the knees. -
WCAT Decision 2005-02580
WCAT Decision Number: WCAT-2005-02580 NOTEWORTHY DECISION SUMMARY Decision: WCAT-2005-02580 Panel: Joanne Kembel Decision Date: May 19, 2005 Pre-existing Conditions – Shoulder Dislocation – Wage Loss Benefits – Section 29(1) of the Workers Compensation Act – Section 30(1) of the Act – Policy Item #15.60 of the Rehabilitation Services and Claims Manual, Volume II (RSCM II) This case is noteworthy as an example of the application of those portions of policy item #15.60 of the Rehabilitation Services and Claims Manual, Volume II (RSCM II) which provide rules for the payment of benefits in shoulder dislocation claims where the worker has previously experienced a non-compensable shoulder dislocation. Item #15.60 of the RSCM II provides that if a worker has a prior non-compensable shoulder dislocation and suffers another dislocation at work, the later dislocation will only be compensable if there was a work incident of “sufficient causative significance to induce the further dislocation”. Once the claim is accepted the policy provides rules in respect of the payment of benefits. The policy provides, firstly, that temporary wage loss benefits will “normally endure no more than two weeks,” and secondly, that any surgery, after the injury, which is directed at repairing damage from the prior dislocation will not be compensable except in cases where: a) the shoulder has been stable for many years prior to the dislocation at work, or b) the dislocation at work was induced by “severe trauma.” In this case, the worker dislocated his left shoulder. The worker had a long history of left shoulder dislocations, and had surgery on his left shoulder three years earlier.