Mapping of Community Home-Based Care Services in Five Regions of the Tanzania Mainland
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Water Access and Distribution in Dar Es Salaam, Tanzania
From Public Pipes to Private Hands Water Access and Distribution in Dar es Salaam, Tanzania Marianne Kjellén Department of Human Geography Stockholm University 2006 Abstract In cities around the world, public water systems have increasingly come to be operated by private companies. Along with an internationally funded investment program to refurbish the dilapidated water infrastructure, private operations were tested also in Dar es Salaam, Tanzania. Only about a third of the households, however, are reached by the piped water system; most households purchase water from those with pipe-connections or private boreholes. Thus, water distribution was informally privatized by way of water vending long before formal private sector participation began. This thesis explores individual and collective endeavors in water development, distribution, and access, along with the global and local influences that shaped the privatization exercise. With regard to the lease of Dar es Salaam’s water system, the institutional set-up has been found to mix the British and French models, having influenced the local situation through development assistance and conditionalities tied to loans. The institutional contradictions may have contributed to the conflictive cancellation of the lease arrangement. Due to the public utility company’s lack of operating capital and investment planning, infrastructure development has responded mainly to immediate individual demands, resulting in a spaghetti-like network and structural leakage. The long-standing under-performance and low coverage of the piped water system have forced many people to devise their own ways to access water. This thesis argues that the individually devised artisan ways of water provisioning constitute the lifeline of Dar es Salaam’s water system. -

Spatial Uncertainties in Fluoride Levels and Health Risks in Endemic Fluorotic
Groundwater for Sustainable Development 14 (2021) 100618 Contents lists available at ScienceDirect Groundwater for Sustainable Development journal homepage: www.elsevier.com/locate/gsd Research paper Spatial uncertainties in fluoridelevels and health risks in endemic fluorotic regions of northern Tanzania Julian Ijumulana a,b,c,*, Fanuel Ligate a,b,d, Regina Irunde a,b,e, Prosun Bhattacharya a,g, Jyoti Prakash Maity f, Arslan Ahmad g,h,i, Felix Mtalo b a KTH-International Groundwater Arsenic Research Group, Department of Sustainable Development, Environmental Science and Engineering, KTH Royal Institute of Technology, Teknikringen 10B, SE-100 44 Stockholm, Sweden b Department of Water Resources Engineering, College of Engineering and Technology, University of Dar Es Salaam, Dar Es Salaam, Tanzania c Department of Transportation and Geotechnical Engineering, College of Engineering and Technology, University of Dar Es Salaam, Dar Es Salaam, Tanzania d Department of Chemistry, Mkwawa College of Education, University of Dar Es Salaam, Tanzania e Department of Chemistry, College of Natural and Applied Sciences, University of Dar Es Salaam, Tanzania f Department of Earth and Environmental Sciences, National Chung Cheng University, 168 University Road, Min-Hsiung, Chiayi County, 62102, Taiwan g KWR Water Cycle Research Institute, Groningenhaven 7, 3433 PE Nieuwegein, The Netherlands h SIBELCO Ankerpoort NV, Op de Bos 300, 6223 EP Maastricht, the Netherlands i Department of Environmental Technology, Wageningen University and Research (WUR), Wageningen, The Netherlands ARTICLE INFO ABSTRACT Keywords: Spatial uncertainty caused by large-scale variation in fluoride(F ) occurrence remains a setback for water supply Groundwater authorities in the F belts of the world. It is estimated that approximately 80 million people in the East African Fluoride contamination Rift Valley (EARV) regions and volcanic areas exhibit a wide variety of fluorosissymptoms due to drinking water Probability kriging with F‾ concentrations higher than 1.5 mg/L (WHO guideline limit). -

Assessment of Water Scarcity and Distribution in Arumeru District -Tanzania
ASSESSMENT OF WATER SCARCITY AND DISTRIBUTION IN ARUMERU DISTRICT -TANZANIA BY MESHACK ELPHACE BAE/12064/61/DF A DISSERTATION SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE AWARD OF THE DEGREE OF BACHELOR OF ARTS WITH EDUCATION OF KAMPALA INTERNATIONAL UNIVERSITY JANUARY 2009 DECLARATION I Meshack Elphace, Registration number BAE/12064/61/DF declare that the work presented in this dissertation is my own and has never been presented in any university or institution. N\ta ttfteb( j:=k,P A-Cf; Name ---------- ------- ------------ -----------rt-- ----------- Signature ----.---------~~-------------- i l 1 <l o.,o o 7 . Date --- -------------------~~ -or-------- --------------------- 11 APPROVAL FOR SUBMISSION This is to acknowledge that, this dissertation entitled "ASSESSMENT OF WATER SCARCITY AND DISTRIBUTION IN ARUMERU DISTRICT TANZANIA" has been approved under my supervision and ready for submission for the award of the degree of Bachelor of Arts with education of Kampala International University. ~ Signatar eC -::::::::::::.. _- ------------- ----------- -------- Date --~~ _Jg~J~j ___ -------------------- -- -- -- --- ---- lll DEDICATION This research is dedicated to my wife Elizabeth Meshack, my child Shadrack Meshack, my parents Elphace Lembalai and Bertha Elphace, my brothers Lazaro Elphace, Micheal, Petro Elphace and my sisters Anne, Lilly, Joyce, Einoth Ndavu and Rizick. All you are a great aspiration to my life. Special thanks go to them for their moral and financial support they offered me through out the three years that finally made this research successful. IV ACKNOWLEDGEMENT I wish to express my thanks to the almighty God for granting me health and all those who assisted me materially and morally to be able to complete this research successfully. Special thanks to my supervisor Mr. -

Arumeru District Catherine W
Conservation agriculture as practised in Tanzania Conservation agriculture in Africa series Series editors Bernard Triomphe Josef Kienzle Martin Bwalya Soren Damgaard-Larsen Titles Conservation agriculture as practised in Ghana Philip Boahen, Benjamin Addo Dartey, Genevieve Delali Dogbe, E. Asare Boadi, Bernard Triomphe, Soren Daamgard-Larsen, John Ashburner Conservation agriculture: a Uganda case study Paul Nyende, Anthony Nyakuni, John Peter Opio, Wilfred Odogola Conservation agriculture in Zambia: a case study of Southern Province Frédéric Baudron, Herbert M. Mwanza, Bernard Triomphe, Martin Bwalya Conservation agriculture as practised in Kenya: two case studies Pascal Kaumbutho, Josef Kienzle, editors Laikipia District Tom Apina, Paul Wamai, Philip Mwangi Siaya District Philip K. Mwangi, Kennedy O. Okelo, Tom Apina Conservation agriculture as practised in Tanzania: three case studies Richard Shetto, Marietha Owenya, editors Arumeru District Catherine W. Maguzu, Dominick E. Ringo, Wilfred Mariki, Marietha Owenya, Flora Kola, Charles Leseyo Karatu District Dominick E. Ringo, Catherine W. Maguzu, Wilfred Mariki, Marietha Owenya, Njumbo, Frank Swai Mbeya District Saidi Mkomwa, Ahaz Mussei, Remmy Mwakimbwala, Ndabhemeye Mulengera, Elimpaa Kiranga Conservation agriculture as practised in Tanzania: three case studies Richard Shetto, Marietha Owenya, editors Arumeru District Karatu District Mbeya District Publishers African Conservation Tillage Network (ACT) PO Box 14733, Westlands Nairobi 00800, Kenya tel and fax: +254 20 445 1391 website: -

Table of Contents
TABLE OF CONTENTS Arusha City Council | Five Years Strategic Plan – 2016/2017 – 2020/2021 Page 1 Abbreviations TSD Cord - Teachers Service Department Coordinator WE - Water Engineer CALDO - City Agriculture and Livestock Development Officer LO - Land Officer CNRO - City Natural Resources Officer ROSA - Resource Oriented sanitation MVC - Most Vulnerable Children C/MENG - Municipal/City Engineer BE - Building Engineer RAS - Regional Administrative Secretariat IT - Information Technology MKURABITA – Mkakati wa Kuratibisha Rasilimali PLHIV - People Living with HIV AUWSA - Arusha Urban water Supply and Sewerage Authority MSO/CSO - Municipal/City Supplies officer MS/CS - Municipal/City Solicitor IA - Internal Auditor MECOM/CICOM - Municipal/City Economic Officer MT/CT - Municipal/City Treasurer MTO/CTO - Municipal/City Trade Officer CMOOH - City Medical Officer of Health CCDO - City Community Development Officer CEO(S) - City Education Officer (Secondary) NMS - National Minimum Standards CHMT - Council Health Management Team MEK - Mratibu Elimu Kata TSD - Teachers Service Department OUT - Open University of Tanzania UCC - University Computing Centre IAA - Institute of Accountancy Arusha VETA - Vocational Education Training Agency SLO - Statistics and Logistic Officer HRO - Human resource Officer CEO (P) - City Education Officer (Primary) Std - Standard DFT - District facilitation Team WFP - World Food Programme WFT - Ward Facilitation Team TSCP - Tanzania Strategic Cities Project TAHA - Tanzania Horticulture Association Arusha City Council | Five Years Strategic Plan – 2016/2017 – 2020/2021 Page 2 PMO-RALG – Prime Minister’s Office Regional Administration and Local Government MoFE - Ministry of Finance CBOs - Community Based Organizations ICT - Information Communication Technology CCP - Chuo Cha Polisi HoDs - Heads of Department AG - Attorney General WEO - ward Executive officer WDC - Ward Development Committee PMU - Procurement management Unit PPRA - Public Procurement regulatory Authority PSPTB - Procurement and Supply Pro. -
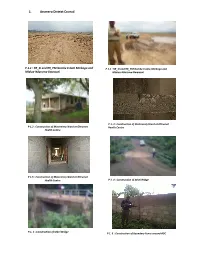
1. Arumeru District Council
1. Arumeru District Council P.1.1 : RR_SI and RR_PM Gombe Estate Mmbogo and P 1.1 : RR_SI and RR_PM Gombe Estate‐Mmbogo and Mlalua‐Nduruma‐Bwawani Mlalua‐Nduruma‐Bwawani P 1. 3 : Construction of Materninty Ward at Oltrumet P 1.2 : Construction of Materninty Ward at Oltrumet Health Centre Health Centre P 1.5 : Construction of Materninty Ward at Oltrumet Health Centre P 1. 4 : Construction of Sekei Bridge P.1. 5 : Construction of Sekei Bridge P 1. 6 : Construction of Boundary Fence around ADC 2. BAHI DISTRICT COUNCIL P 2.1: Aditors at contractor's site office reviewing P2.2: Uncompacted fill and poor concrete drawings workmanship on Kongogo Dam P 2.3: Un‐cemented Riprap at Kongogo Dam P 2.4: Poorly trimmed borrow pit at Kongogo P 2.5: Auditors checking dimensions compliance at Bahi DC P 2.6: Completed Kigwe Mnadani Drift Servant Quarters P 2.7: Auditors confirming a borehole at Mchito P 2.8: Auditors discussing with village leader at Borehole Mundemu on the way forward - dry borehole 3. Bukoba District Council P. 3.1: Cracks can be seen on the floor and walls of a newly constructed Agricultural Centre at Kikomelo P. 3.2: A newly constructed small bridge P 3.3: Oversize, dirty, sand stone coarse aggregates used for bridges/box culverts along Kalebe- Nyakibimbili road P 3.4: A bridge whose width was increased a day after casting without engineer’s approval along Kalebe- Nyakibimbili road 4. Geita District Council P 4.1: Poorly constructed pavement at the New Geita Bus Stand P 4.2: An auditor and PE Technician carrying out P 4.3: Well constructed headwalls and wingwalls and measurements at the New Geita Bus Stand poorly compacted approaches along Geita Town – Katoma Area Roads P 4.4 Poor workmanship on constructed headwall P 4.5 One of the existing “Bridges” along Sungusira and wing walls along Sungusira – Nyakaduha Road Road 5. -

Dar Es Salaam-Ch1.P65
Chapter One The Emerging Metropolis: A history of Dar es Salaam, circa 1862-2000 James R. Brennan and Andrew Burton This chapter offers an overview history of Dar es Salaam. It proceeds chronologically from the town’s inception in the 1860s to its present-day status as one of the largest cities in Africa. Within this sequential structure are themes that resurface in later chapters. Dar es Salaam is above all a site of juxtaposition between the local, the national, and the cosmopolitan. Local struggles for authority between Shomvi and Zaramo, as well as Shomvi and Zaramo indigenes against upcountry immigrants, stand alongside racialized struggles between Africans and Indians for urban space, global struggles between Germany and Britain for military control, and national struggles between European colonial officials and African nationalists for political control. Not only do local, national, and cosmopolitan contexts reveal the layers of the town’s social cleavages, they also reveal the means and institutions of social and cultural belonging. Culturally Dar es Salaam represents a modern reformulation of the Swahili city. Indeed it might be argued that, partly due to the lack of dominant founding fathers and an established urban society pre- dating its rapid twentieth century growth, this late arrival on the East African coast is the contemporary exemplar of Swahili virtues of cosmopolitanism and cultural exchange. Older coastal cities of Mombasa and Zanzibar struggle to match Dar es Salaam in its diversity and, paradoxically, its high degree of social integration. Linguistically speaking, it is without doubt a Swahili city; one in which this language of nineteenth-century economic incorporation has flourished as a twentieth-century vehicle of social and cultural incorporation for migrants from the African interior as well as from the shores of the western Indian Ocean. -
WORKING PAPER February 2012
REPORT ON INVESTIGATION OF DAR ES SALAAM’S INSTITUTIONAL ACTIVITIES RELATED TO CLIMATE CHANGE WORKING PAPER February 2012 KASSENGA, Gabriel (ARDHI University) MBULIGWE, Stephen (ARDHI University) The project is co-funded by European Union How to quote: Kassenga Gabriel, Mbuligwe Stephen “Report on Investigation of Dar es Salaam‘s Institutional Activities related to Climate Change” Working Paper, February 2012 Dae es Salaam: Ardhi University. Available at: http://www.planning4adaptation.eu/ This work is licensed under a Creative Commons Attribution-NonCommercial 3.0 Unported License. http://creativecommons.org/licenses/by-nc/3.0/ Table of Contents Figures IV Tables V Annexes VI Acknowledgements VII 1 Introduction 1 1.1 Background and Rationale of the ACC Dar Projectt 1 1.2 Objective and Purpose o the Study 1 1.3 Study Methodology 1 1.4 Scope and Organisation of the Report 2 2 Dar es Salaam City 3 2.1 Introduction 3 2.2 Dar es Salaam City Physical and Social-Economic Characteristics 3 2.3 Survey Findings 5 2.3.1 Names and Details of the Interviews 6 2.3.2 Age Distribution 6 2.3.3 Education Profile 6 2.3.4 Period of Service 7 2.3.5 Competence and Responsibilities 7 2.3.6 Relationship between Institutions 8 2.3.7 Strategies and Programs in PU 8 2.3.8 Specific Policies and Strategies for PU 9 2.3.9 Financial Resources 10 2.3.10 Facility Supply in the PU 10 2.3.11 Development Changes in the PU in Past Years 11 2.3.12 Main Linkage and Interdependencies between City Centre, PU and Rural Areas 11 2.3.13 Informal and Formal Groups, NGOs, CBOs and -
Final Report
Final Report Baseline Study for Hand in Hand Eastern Africa Program in Northern Tanzania August 2017 Table of Contents Table of Contents.................................................................................................................. 2 List of tables.......................................................................................................................... 3 List of figures ........................................................................................................................ 4 List of Abbreviations.............................................................................................................. 5 Acknowledgement................................................................................................................. 6 Executive Summary .............................................................................................................. 7 1. Introduction.................................................................................................................. 13 1.1 Overview of HiH EA Model.................................................................................... 13 1.2 HiH EA Expansion Plan for Tanzania.................................................................... 14 2. The Baseline Study...................................................................................................... 15 2.1 The Scoping Study................................................................................................ 15 2.1.1 Objectives of the Scoping -

Recapping the Meru Land Case, Tanzania by Dr
Global Journal of HUMAN SOCIAL SCIENCES Economics Volume 13 Issue 1 Version 1.0 Year 2013 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Inc. (USA) Online ISSN: 2249-460x & Print ISSN: 0975-587X Recapping the Meru Land Case, Tanzania By Dr. Simeon Mesaki University of Dodoma, Tanzania Abstract - Mt Meru dominates the scenery and economy of the people living on its slopes. The lower slopes of the mountain provided fertile, well-watered land for the Meru and Arusha people for several centuries. Here they have developed "moral economies," innovative and well- managed mixed farming and agro-pastoral systems. The earliest Meru were Chaga speakers from western Kilimanjaro who expanded across the Sanya plains sometimes in the 17th century. They were traditionally organised through “big men” known as vashili (singular nshili who supervised all important matters including traditional prayers, land conflicts, inheritance, farm boundaries, ceremonies and punishment. There were chiefs and elders who met under a large sacred tree, the mringaringa. Colonial occupation since the late 19th century caused the closing of the land frontier on Meru and alienation of most of their land to white settlers. The Meru Land Case was a protest by Meru people, living in the Eastern part of what is now Arumeru District, against the allocation of their land to Europeans for development purposes. It is a tale of the Meru united to demand in an international forum the restitution of their rights to land. It is the story of Kirilo Japhet the first Tanzania to speak at the United Nations and in Kiswahili at that. -

Crime and Policing Issues in Dar Es Salaam Tanzania Focusing On: Community Neighbourhood Watch Groups - “Sungusungu”
CRIME AND POLICING ISSUES IN DAR ES SALAAM TANZANIA FOCUSING ON: COMMUNITY NEIGHBOURHOOD WATCH GROUPS - “SUNGUSUNGU” PRESENTED AT THE 1st SUB SAHARAN EXECUTIVE POLICING CONFERENCE INTERNATIONAL ASSOCIATION OF CHIEFS OF POLICE (IACP) DURBAN, SOUTH AFRICA: 27 – 30 AUGUST, 2000 Contents PREFACE:.........................................................................................................................................................................................I EXECUTIVE SUMMARY............................................................................................................................................................III 1.0 INTRODUCTION............................................................................................................................................................ 7 DAR ES SALAAM IN BRIEF............................................................................................................................................................. 7 1.1 GEOGRAPHICAL LOCATION:......................................................................................................................................... 7 1.2 HISTORICAL:.................................................................................................................................................................. 7 1.3 SOCIO-ECONOMIC AND ENVIRONMENTAL SETTING:.................................................................................................. 9 1.4 ORGANISATIONAL SETTING:.......................................................................................................................................13 -
Progress Report: GMH (#0090): an Integrated Approach to Addressing the Issue of Adolescent Depression In
Progress Report: GMH (#0090): An Integrated Approach to Addressing the Issue of Adolescent Depression in Malawi and Tanzania August 5, 2014 Submitted To: Grand Challenges Canada Submitted By: Farm Radio International Progress against milestones for period ending July 15, 2014 MoUs signed with Ministry Health and Education in Tanzania To date, we have held two stakeholder meetings and one mental health training to secure buy-in from relevant government ministries. Representatives from the regional and district level MoE and MoH were invited to attend the meetings. We have also had one face-to-face meeting with the Director of Mental Health Services in the Ministry of Health in Dar es Salam. Representatives from the ministries have indicated their enthusiasm and support for the project, and their willingness to form a technical advisory group and to sing Memoranda of Understanding for the project. MoUs have been sent to the national MoE and MoH, and are awaiting a reply 35 schools selected for participation in target districts in Tanzania 35 secondary schools have been selected for participation in the program, and we have received clearance to conduct activities by the regional and district level representatives from the Ministry of Education. To date, we have completed a baseline survey of 350 youth from 10 schools, and will survey another 350 youth from an additional 10 schools by the end of August, 2014. Attached (annex 1) is a list of 35 schools selected for participation in the program 2 MOUs signed with radio stations We have selected 2 radio stations in the Arusha region to participate in the communication component of the program in Tanzania.