Health Sector Bulletin
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nationwide School Assessment Libya Ministry
Ministry of Education º«∏©àdGh á«HÎdG IQGRh Ministry of Education Nationwide School Assessment Libya Nationwide School Assessment Report - 2012 Assessment Report School Nationwide Libya LIBYA Libya Nationwide School Assessment Report 2012 Libya Nationwide School Assessment Report 2012 º«∏©àdGh á«HÎdG IQGRh Ministry of Education Nationwide School Assessment Libya © UNICEF Libya/2012-161Y4640/Giovanni Diffidenti LIBYA: Doaa Al-Hairish, a 12 year-old student in Sabha (bottom left corner), and her fellow students during a class in their school in Sabha. Doaa is one of the more shy girls in her class, and here all the others are raising their hands to answer the teacher’s question while she sits quiet and observes. The publication of this volume is made possible through a generous contribution from: the Russian Federation, Kingdom of Sweden, the European Union, Commonwealth of Australia, and the Republic of Poland. The contents of this publication are the sole responsibility of the authors and can in no way be taken to reflect the views of the donors. © Libya Ministry of Education Parts of this publication can be reproduced or quoted without permission provided proper attribution and due credit is given to the Libya Ministry of Education. Design and Print: Beyond Art 4 Printing Printed in Jordan Table of Contents Preface 5 Map of schools investigated by the Nationwide School Assessment 6 Acronyms 7 Definitions 7 1. Executive Summary 8 1.1. Context 9 1.2. Nationwide School Assessment 9 1.3. Key findings 9 1.3.1. Overall findings 9 1.3.2. Basic school information 10 1.3.3. -

Covid-19 Epi Weekly Libya 9 May 2021.Pdf (English)
Libya COVID-19 Surveillance Weekly Bulletin Epidemiological Week 19 (3 – 9 May) Data as received from the National Center for Disease Center (NCDC) Total New Total Total New Total New Total New tested tested active confirmed confirmed recovered recovered deaths deaths 995,373 12,241 10,474 180,226 1,891 166,680 2,484 3,072 25 Highlights: • 23 COVID-19 labs (out of 32) reported 12,241 new 12,000 11,310 lab tests done for Epi-week 19. Out of the total 995,373 tests done in Libya since the beginning of the 10,000 response, 180,226 (18.1%) were confirmed positive for 8,000 SARS-CoV-2 (COVID-19). • As compared to Epi-week 18, there was a 22% 6,000 decrease in overall national testing: by regions a 24% decrease in the West and 62% decrease in the South. 4,000 The East reported a 95% increase (-see fig. 1) 1,684 2,000 795 • The national positivity rate for Epi-week 19 further 187 5 136 20 3 17 decreased from 16.4% to 15.4%; this is attributable to - overall decreased case numbers in the West and East South West Lab tests Cases Deaths South, positivity rates of 14.7%. It cannot be generalized based on a much higher positivity rate in Fig. 1: COVID-19 cases, deaths, and lab tests for Epi week 19 by region the East (23.5%) than the national-level positivity rate. • The overall number of new cases reported shows a 27% decrease compared to the prior week, with West reporting a 30% decrease in new patients. -

Factors Affecting Recent Vegetation Change in North-East Libya
FACTORS AFFECTING RECENT VEGETATION CHANGE IN NORTH-EAST LIBYA GHADA. M. A. AHWAIDI Ecosystems and Environment Research Centre School of Environment and Life Sciences University of Salford Salford, M5 4WT, UK Submitted in Partial Fulfilment of the Requirements of the Degree of Doctor of Philosophy, 19 July 2017 i Contents Table of contents…………………………………………………………………… ... i List of tables………………………………………………………………………….. v List of figures………………………………………………………………………….. vi Acknowledgements……………………………………………………………………. ix Declaration…………………………………………………………………………….. x Abstract………………………………………………………………………………… xi CHAPTER 1: INTRODUCTION…………………………………………………..… 1 1.1 Introduction to the research……………………………………………… 1 1.2 Research aims and objectives……………………………………………. 4 1.3 Thesis structure………………………………………………………….. 7 CHAPTER 2: LITERATURE REVIEW……………………………………….…... 10 2.1 Introduction ……………………………………………………………... 10 2.2 Vegetation cover change in the Mediterranean region…………………... 11 2.3 Factors affecting vegetation change……………………………………... 12 2.3.1 General factors affecting vegetation change…………………………...… 12 2.3.2 Effects of human activity on vegetation change in the Mediterranean region 13 2.3.3 Effect of climate change on vegetation in the Mediterranean region….… 14 2.4 Approaches to monitoring vegetation change……………………………. 17 2.4.1 Ground based measurement of vegetation……………………………….. 18 2.4.1.1 Vegetation cover …………………………………………………………. 18 2.4.1.2 Leaf area index…………………………………………………………… 19 2.4.1.3 Density…………………………………………………………………… 19 2.4.2 Remote sensing of vegetation change……………………………………. 19 2.4.2.1 Spectral response of vegetation…………………………………………… 20 2.4.2.2 Vegetation Indices (VI)…………………………………………………... 22 2.4.2.2.1 Normalized Difference Vegetation Index (NDVI)……………………….. 22 2.4.2.2.2 Soil Adjusted Vegetation Index (SAVI)………………………………….. 23 2.4.2.2.3 Enhance Vegetation Index (EVI)…………………………………………. 24 2.4.2.3 Image classification………………………………………………………. 25 2.5 Remote sensing of vegetation change in the Mediterranean…………….. -

Libya Is Located in the North of Africa Between Longitude 9O ‐ 25O East and Latitude 18O ‐ 33O North
Libya is located in the north of Africa between longitude 9o ‐ 25o east and latitude 18o ‐ 33o north. It extends from the Mediterranean coast in the north to the Sahara desert in the south, with a total surface area of approximately 1.750 million km2.Itis bounded on the east by Egypt, on the west by Tunisia and Algeria and on the south by Chad, Niger and Sudan. According to 2006 census, the total population of Libya amounted to about 5.658 millions (5.298 Libyans and 0.360 non‐Libyans) The population density varies widely from one area to another. About 70% of Libyan population lives in the coastal cities, where more than 45% live in Tripoli, Benghazi, Misrātah and AzZawayah, with a population density of about 45 person per km2. This density does not exceed 0.3 person per km2 in the interior regions. Location map Rainfall in Libya is characterized by its inconsistency as a result of the contrary effects of the Sahara from one side and the Mediterranean from the other. Intensive thunderstorms of short duration are fairly common. Abou t 96% of Libyan ldland surface receives annual raifllinfall of less than 100 mm. The heaviest rainfall occurs in the northeastern region (Jabal al Akhdar) from 300 to 600mm and in the northwestern region (Jabal Nafūsah and Jifārah plain) from 250 to 370mm. There is no perennial surface runoff in Libya, a part of the precipitation falling on the Jabal Nafūsah and Jabal al Akhdar cause a surface runoff trough many seasonal wadis. Wadis in a desert environment generally are dry during the whole year except after sudden heavy rainfall which often resulting a flash flood. -
0X0a I Don't Know Gregor Weichbrodt FROHMANN
0x0a I Don’t Know Gregor Weichbrodt FROHMANN I Don’t Know Gregor Weichbrodt 0x0a Contents I Don’t Know .................................................................4 About This Book .......................................................353 Imprint ........................................................................354 I Don’t Know I’m not well-versed in Literature. Sensibility – what is that? What in God’s name is An Afterword? I haven’t the faintest idea. And concerning Book design, I am fully ignorant. What is ‘A Slipcase’ supposed to mean again, and what the heck is Boriswood? The Canons of page construction – I don’t know what that is. I haven’t got a clue. How am I supposed to make sense of Traditional Chinese bookbinding, and what the hell is an Initial? Containers are a mystery to me. And what about A Post box, and what on earth is The Hollow Nickel Case? An Ammunition box – dunno. Couldn’t tell you. I’m not well-versed in Postal systems. And I don’t know what Bulk mail is or what is supposed to be special about A Catcher pouch. I don’t know what people mean by ‘Bags’. What’s the deal with The Arhuaca mochila, and what is the mystery about A Bin bag? Am I supposed to be familiar with A Carpet bag? How should I know? Cradleboard? Come again? Never heard of it. I have no idea. A Changing bag – never heard of it. I’ve never heard of Carriages. A Dogcart – what does that mean? A Ralli car? Doesn’t ring a bell. I have absolutely no idea. And what the hell is Tandem, and what is the deal with the Mail coach? 4 I don’t know the first thing about Postal system of the United Kingdom. -
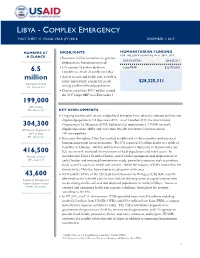
Libya Complex Emergency Fact Sheet #1
YEMEN - COMPLEX EMERGENCY FACT SHEET #7, FISCAL YEAR (FY) 2016 JANUARY 1, 2016 LIBYA - COMPLEX EMERGENCY FACT SHEET #1, FISCAL YEAR (FY) 2018 DECEMBER 1, 2017 NUMBERS AT HIGHLIGHTS HUMANITARIAN FUNDING FOR THE LIBYA RESPONSE IN FY 2016–2017 A GLANCE Insecurity in Libya continues to generate USAID/OFDA1 $4,625,311 displacement, humanitarian needs UN records 23 civilian deaths in State/PRM2 $23,700,000 6.5 October as a result of conflict in Libya million Access to cash and health care, as well as safety and security, remain key needs $28,325,311 Population of Libya UN – September 2017 among conflict-affected populations Donors contribute $85.7 million toward the 2017 Libya HRP as of December 1 199,000 IDPs in Libya IOM – October 2017 KEY DEVELOPMENTS Ongoing conflict, civil unrest, and political instability have adversely affected civilians and displaced populations in Libya since 2011. As of October 2017, the International 304,300 Organization for Migration (IOM) had identified approximately 199,000 internally IDP Returns Registered in displaced persons (IDPs) and more than 304,300 cumulative returnees across 2017 to Date 100 municipalities. IOM – October 2017 Insecurity throughout Libya has resulted in additional civilian casualties and increased humanitarian needs in recent months. The UN reported 23 civilian deaths as a result of hostilities in October. Military activity in northeastern Libya’s city of Darnah since late 416,500 July has severely restricted the movement of local populations and relief actors. In Migrants in Libya northwestern Libya’s Sabratha District, armed clashes prompted rapid displacement in IOM – August 2017 early October and increased humanitarian needs, particularly access to cash to purchase food, as well as access to health care services. -

Similarities Between Elevations in a Rare Species of Some Locations at Al- Jabal Al- Akhdar in Libya
International Journal of Environment Volume : 06 | Issue : 03 | July-Sept. | 2017 ISSN 2077-4505 Page:78-102 Similarities between elevations in a rare species of some locations at Al- Jabal Al- Akhdar in Libya Abusaief, H. M. A. Agronomy Department, Fac. Agric., Omar Al-Mukhtar Univ., Libya Received: 20 May 2017 / Accepted: 28 June 2017 / Publication Date: 10 July 2017 ABSTRACT Survey of rare species in fifteen sites selected according to elevation of Al-Jabal Al-Akhdar, Libya of 828-232 m M.S.L. The site of Habun and Shahat old city is approaches in altitude from sea level, Habun site elevation 614 M.S.L. while the Shahat old city 580 m M.S.L, indicating the importance of the elevation importance in distribution of rare species in Al-Jabal Al-Akhdar. It was noticed that 85 % of species was perennial and 15 % was annuals. Herbs 43 %, Shrubs 40 %, 17 % Trees. Most of the species following Chamaephytes which represented 37 % of the species, while, Phanerophyte annual plants 30 % followed by Therophytes 15 %, Geophytes and Hemicryptophytes 7 %, as well as Hydrophytes 4 %. The variation in the number of plants per species gave two groups the first group was in the two sites of Slonta and Sidi Alhamri, about 781 – 802 m M.S.L., and 75 %, the second group is divided into the Shahat old city group, Cyrenaica is the largest plant diversity region in Libya.One species of Extinct was Narcissus tazetta L. in IUCN was Endangered. Five species classified Critically Endangered includes Ephedra alata (Decne.), Foeniculm vulgar (Mill. -

Libya Multi-Sector Needs Assessment – April 2020
0 Libya Multi-Sector Needs Assessment – April 2020 Assessment conducted in the framework of: Funded by: With the support of: Cover photo: Ayoub Ahmed 2018 About REACH and ACTED REACH is a programme of ACTED. It strengthens evidence-based decision-making by humanitarian actors through efficient data collection, management and analysis in contexts of crisis. ACTED is an international NGO. Independent, private and non-profit, ACTED respects a strict political and religious impartiality, and operates following principles of non-discrimination and transparency. Since 2011, ACTED has been providing humanitarian aid and has supported civil society and local governance throughout Libya, from its offices in Tripoli, Sebha and Benghazi. 1 Libya Multi-Sector Needs Assessment – April 2020 SUMMARY “The situation is intolerable, our fate is unknown, and there is almost complete dependence on personal relationships for everything. It is bad that you have to be displaced in a sudden circumstance, and there is not even time for reflection or the possibility to try to adapt to new situations.” –Murzuq focus group participant Context Since 2011, Libya has faced waves of conflict, coupled with political and economic instability. This protracted conflict escalated again in early April 2019, leading to large-scale displacement in Tripoli and the surrounding areas. However, the effects of the conflict have extended far beyond the parts of the country where fighting is concentrated. Nine years of civil conflict have resulted in serious governance challenges, which have limited public institutions’ ability to deliver basic services, and which have contributed to insecurity and outbreaks of violence far from the front lines, such as in Murzuq in August 2019. -

2021 Humanitarian Response Plan for Libya
HUMANITARIAN HUMANITARIAN PROGRAMME CYCLE 2021 RESPONSE PLAN ISSUED JANUARY 2021 LIBYA 01 HUMANITARIAN RESPONSE PLAN 2021 About Get the latest updates This document is consolidated by OCHA on behalf of the Human- itarian Country Team and partners. The Humanitarian Response OCHA coordinates humanitarian action to Plan is a presentation of the coordinated, strategic response ensure crisis-affected people receive the assistance and protection they need. It works to devised by humanitarian agencies in order to meet the acute needs overcome obstacles that impede humanitarian of people affected by the crisis. It is based on, and responds to, assistance from reaching people affected by evidence of needs described in the Humanitarian Needs Overview. crises, and provides leadership in mobilizing assistance and resources on behalf of the PHOTO ON COVER humanitarian system UNICEF - LIBYA www.unocha.org/libya www.twitter.com/ocha_libya The designations employed and the presentation of material in the report do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Humanitarian Response aims to be the central website for Information Management tools and services, enabling information exchange between clusters and IASC members operating within a protracted or sudden onset crisis. www.humanitarianresponse.info/en/operations/libya Humanitarian InSight supports decision-makers by giving them access to key humanitarian data. It provides the latest verified informa- tion on needs and delivery of the humanitarian response as well as financial contributions. -

A Preliminary Documentation of the Coral Reefs from Libya
Open Journal of Geology, 2016, 6, 260-269 Published Online April 2016 in SciRes. http://www.scirp.org/journal/ojg http://dx.doi.org/10.4236/ojg.2016.64023 A Preliminary Documentation of the Coral Reefs from Libya Belkasim Khameiss1*, William Hoyt2, Saad K. El Ebaidi3, Ahmed M. Muftah3, James Klaus4, Ann Budd5 1Department of Geological Sciences, Ball State University, Muncie, IN, USA 2Earth and Atmospheric Sciences, University of Northern Colorado, Greeley, CO, USA 3Department of Earth Sciences, Faculty of Science, University of Benghazi, Benghazi, Libya 4Department of Geological Science, University of Miami, Coral Gables, FL, USA 5Department of Geoscience, University of Iowa, Iowa City, IA, USA Received 4 February 2016; accepted 18 April 2016; published 21 April 2016 Copyright © 2016 by authors and Scientific Research Publishing Inc. This work is licensed under the Creative Commons Attribution International License (CC BY). http://creativecommons.org/licenses/by/4.0/ Abstract Corals studies in Libya are very limited, although they play an important role in the oil exploration as they form excellent reservoirs of coral reef buildups at some oil fields of Sirt Basin (e.g. Intisar “Idris” and Sahabi Fields). Both fields are produced from Paleocene coral reefs. Meanwhile, in Cy- renaica, corals are of less importance as they are not reported in subsurface tertiary rocks, which probably in the environmental settings of these sediments out of the core of reef as occurred in the surface. Meanwhile, corals are reported from older (Jurassic) subsurface successions as in Conces- sion NC-152, but the cementation diagenesis leads to blocking and destroying the porosity. -

Seismic Risk Perception in Al-Marj, Libya: a Case Study After the 1963 Earthquake
Open Journal of Earthquake Research, 2020, 9, 349-366 https://www.scirp.org/journal/ojer ISSN Online: 2169-9631 ISSN Print: 2169-9623 Seismic Risk Perception in Al-Marj, Libya: A Case Study after the 1963 Earthquake Somaia S. Suwihli1,2, Thomas R. Paradise1 1Department of Geosciences, University of Arkansas, Fayetteville, USA 2Department of Geography, University of Benghazi, Benghazi, Libya How to cite this paper: Suwihli, S.S. and Abstract Paradise, T.R. (2020) Seismic Risk Percep- tion in Al-Marj, Libya: A Case Study after Individual beliefs, knowledge, and perception play a vital role in understand- the 1963 Earthquake. Open Journal of Earth- ing and coping with the consequences of earthquakes. These perceptions then quake Research, 9, 349-366. mold the broader perceptions of risk and danger held by communities, which https://doi.org/10.4236/ojer.2020.94020 ultimately create public policy. This survey study was designed and conducted Received: July 1, 2020 to assess the perceptions of seismic hazard and risk of earthquake survivors Accepted: August 3, 2020 and residents in Al-Marj, Libya—a city razed in a 1963 tremor. In 2019, 364 Published: August 6, 2020 earthquake survivors and residents were surveyed for their knowledge and Copyright © 2020 by author(s) and perception of earthquakes. Surveys were conducted in Arabic and included Scientific Research Publishing Inc. demographic and narrative questions in addition to Likert-scaled responses. This work is licensed under the Creative A number of predictable, surprising, and valuable correlations were found. It Commons Attribution International was found that during earthquakes most respondents prayed to Allah, or did License (CC BY 4.0). -

Education in Danger Monthly News Brief January 2018 Page 1
Education in Danger Education January Monthly News Brief 2018 Insecurity affecting the provision of education Threats and incidents of violence against This monthly digest comprises threats and educational workers incidents of violence as well as protests and other events Africa affecting education. Cameroon 15 January 2018: In Buea, Limbe and Tiko, Fako division, Southwest It is prepared by Insecurity region, rumours that suspected separatists would attack Insight from information educational facilities led to the evacuation of schools and available in open sources. universities, including the University of Buea. Sources: Cameroon- Info and Journal du Cameroun All decisions made, on the basis of, or with Nigeria consideration to, such 07 January 2018: Update: In Akampa. Cross River state, gunmen information remains the released a medical practitioner from the Cross-River College of responsibility of their Education Medical Centre, kidnapped since 26 December. Sources: respective organisations. Daily Trust and Guardian Editorial team: 08 January 2018: In Calabar, Cross River state, unidentified Christina Wille, Larissa Fast perpetrators kidnapped a senior registrar in the Department of Laurence Gerhardt and Pediatrics, University of Calabar Teaching Hospital. Source: Daily Helen Buck Insecurity Trust Insight Research team: Sudan James Naudi 11 January 2018: In South Kordofan state, a member of the Sudan Insecurity Insight Armed Forces (SAF) entered Delling University armed with a concealed Kalashnikov and shot and killed two students. Then Subscribe here to receive committed suicide. His motive remains unclear. Source: Dabanga monthly reports on Sudan insecurity affecting the provision of education. Asia Afghanistan Suggested citation: 24 January 2018: In Jalalabad, Nangarhar province, gunfire from an Insecurity Insight.