Unaids Executive Director Report Profound Change Often Occurs in the Context of Crisis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Conversation Living Feminist Politics - Amina Mama Interviews Winnie Byanyima
Conversation Living Feminist Politics - Amina Mama interviews Winnie Byanyima Winnie Byanyima is MP for Mbarara Municipality in Western Uganda. The daughter of two well-known politicians, she was a gifted scholar and won awards to pursue graduate studies in aeronautical engineering. However, she chose to join the National Resistance Movement under Museveni's leadership, and later became one of the first women to stand successfully for direct elections. Winnie is best known for her gender advocacy work with non- governmental organisations, her anti-corruption campaigns, and her opposition to Uganda's involvement in the conflict in the Democratic Republic of Congo. She is currently affiliated to the African Gender Institute, where she is writing a memoir of three generations of women – her grandmother, her mother and her own life in politics. Here she is interviewed by Amina Mama on behalf of Feminist Africa. Amina Mama: Let's begin by talking about your early life, and some of the formative influences. Winnie Byanyima: I grew up pretty much my father's daughter. I admired him very much, and people said I was like him. I had a more difficult relationship with my mother. But in the last few years as I've tried to reflect on who I am and why I believe the things that I believe, I've found myself coming back to my mother and my grandmother, and having to face the fact that I take a lot from those women. It's tough, because it means that I must recognise all that I didn't take as important about my mother's struggles. -

Political Theologies in Late Colonial Buganda
POLITICAL THEOLOGIES IN LATE COLONIAL BUGANDA Jonathon L. Earle Selwyn College University of Cambridge This dissertation is submitted for the degree of Doctor of Philosophy 2012 Preface This dissertation is the result of my own work and includes nothing which is the outcome of work done in collaboration except where specifically indicated in the text. It does not exceed the limit of 80,000 words set by the Degree Committee of the Faculty of History. i Abstract This thesis is an intellectual history of political debate in colonial Buganda. It is a history of how competing actors engaged differently in polemical space informed by conflicting histories, varying religious allegiances and dissimilar texts. Methodologically, biography is used to explore three interdependent stories. First, it is employed to explore local variance within Buganda’s shifting discursive landscape throughout the longue durée. Second, it is used to investigate the ways that disparate actors and their respective communities used sacred text, theology and religious experience differently to reshape local discourse and to re-imagine Buganda on the eve of independence. Finally, by incorporating recent developments in the field of global intellectual history, biography is used to reconceptualise Buganda’s late colonial past globally. Due to its immense source base, Buganda provides an excellent case study for writing intellectual biography. From the late nineteenth century, Buganda’s increasingly literate population generated an extensive corpus of clan and kingdom histories, political treatises, religious writings and personal memoirs. As Buganda’s monarchy was renegotiated throughout decolonisation, her activists—working from different angles— engaged in heated debate and protest. -

Press Review September 2016, Edition 15
PRESS REVIEW John Paul II Justice and Peace Centre “Faith Doing Justice” EDITION 15 SEPTEMBER 2016 THEMATIC AREAS Plot 2468 Nsereko Road-Nsambya Education P.O. Box 31853, Kampala-Uganda Environment Tel: +256414267372 Health Mobile: 0783673588 Economy Email: [email protected] Religion and Society [email protected] Politics Website: www.jp2jpc.org Youth Christian Reflection EDUCATION MPs decry varsity staff shortage. Lawmakers on parliament’s Education Committee have asked government to increase funding to public universities so that they can fill the vacant positions, particularly the teaching staff, which are needed to lift the quality of education in the country. Dokolo north MP Paul Amoru said the low staffing level at MUST (Mbarara University of Science and Technology) is a serious concern because it was set up to be developed as governments major science institution. Govt nursery schools to start next year. Plans are underway by the Education Ministry to introduce nursery classes in its public primary schools across the country in the next academic year. Rosemary Seninde, State Minister for primary education, emphasised that the education ministry would now put much emphasis on the children’s early childhood education which is nursery education. Teachers reject govt transfer plan. A number of the head teachers joined the Anglican Bishop of Ankole diocese in rejecting a looming policy which bars teachers who are married from working at the same station. Ms Nakatte Kikomeko, the head teacher of Nabbingo girl’s school, however, said administrative issues could arise in case the man is a director of studies and his wife is teaching in the school. -

2002 Released by the Bureau of Democracy, Human Rights, and Labor March 31, 2003
Uganda Page 1 of 26 Uganda Country Reports on Human Rights Practices - 2002 Released by the Bureau of Democracy, Human Rights, and Labor March 31, 2003 President Yoweri Museveni continued to dominate the Government after he was reelected to a second 5-year term in March 2001. He has ruled since 1986 through the dominant political party, The Movement. The Constitution provides for an autonomous, independently elected President and a 295-member unicameral Parliament whose members were elected to 5-year terms. The Parliament was weak compared to the Executive, although it occasionally displayed independence and assertiveness. In the June 2001 parliamentary elections, more than 50 percent of those elected were new legislators; however, Movement supporters remained in control of the legislative branch. Observers believed that the 2001 presidential and parliamentary elections generally reflected the will of the population; however, both were marred by serious irregularities, particularly in the period leading up to the elections, such as restrictions on political party activities, incidents of violence, voter intimidation, and fraud. A 2000 national referendum on the role of political parties formally extended the Movement form of government indefinitely and severely restricted political activities. The Constitutional Review Commission (CRC) continued to work to amend the 1995 Constitution during the year. The judiciary generally was independent but was understaffed and weak; the President had extensive legal powers. The Uganda People's Defense Force (UPDF) was the key security force. The Constitution provides for civilian control of the UPDF, with the President designated as Commander in Chief; a civilian served as Minister of Defense. -

The Cotter Pin by Andrew Rice
AR-7 Sub-Saharan Africa Andrew Rice is a Fellow of the Institute studying life, politics and development in ICWA Uganda and environs. LETTERS The Cotter Pin By Andrew Rice JANUARY 1, 2003 Since 1925 the Institute of KAMPALA, Uganda—The sirens’ wail was getting louder. Outside the Nile Current World Affairs (the Crane- Hotel’s International Conference Center, the hexagonal slab of port-holed con- Rogers Foundation) has provided crete where three decades of Ugandan presidents have welcomed important visi- long-term fellowships to enable tors, the blue-uniformed honor guard stiffened to attention in the late-November outstanding young professionals heat. The ministers and generals took their places on the steps. Reporters pulled to live outside the United States out their notebooks, news photographers lifted their cameras to their shoulders. and write about international All eyes fixed on the front gates. The presidents were about to arrive. areas and issues. An exempt operating foundation endowed by A little after 10a.m., a pickup truck peeled through the gates, loaded with the late Charles R. Crane, the security officers, machine guns at the ready. A pair of motorcycle police followed, Institute is also supported by leading the way for the black Mercedes limousine. It glided to the front of the contributions from like-minded building and stopped. individuals and foundations. The doors of the limousine opened, and the presidents emerged. From one side, His Excellency Daniel Toroitich Arap Moi, president of Kenya, dressed in his customary fashion: a dark blue suit and a garish multicolored necktie. From TRUSTEES the other, His Excellency Yoweri Kaguta Museveni, president of Uganda, nattily Bryn Barnard attired as always. -
Time Line of Key Historical Events*
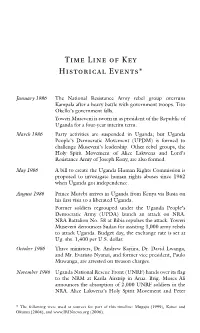
Time Line of Key Historical Events* January 1986 The National Resistance Army rebel group overruns Kampala after a heavy battle with government troops. Tito Okello’s government falls. Yoweri Museveni is sworn in as president of the Republic of Uganda for a four-year interim term. March 1986 Party activities are suspended in Uganda; but Uganda People’s Democratic Movement (UPDM) is formed to challenge Museveni’s leadership. Other rebel groups, the Holy Spirit Movement of Alice Lakwena and Lord’s Resistance Army of Joseph Kony, are also formed. May 1986 A bill to create the Uganda Human Rights Commission is proposed to investigate human rights abuses since 1962 when Uganda got independence. August 1986 Prince Mutebi arrives in Uganda from Kenya via Busia on his first visit to a liberated Uganda. Former soldiers regrouped under the Uganda People’s Democratic Army (UPDA) launch an attack on NRA. NRA Battalion No. 58 at Bibia repulses the attack. Yoweri Museveni denounces Sudan for assisting 3,000 army rebels to attack Uganda. Budget day, the exchange rate is set at Ug. shs. 1,400 per U.S. dollar. October 1986 Three ministers, Dr. Andrew Kayiira, Dr. David Lwanga, and Mr. Evaristo Nyanzi, and former vice president, Paulo Muwanga, are arrested on treason charges. November 1986 Uganda National Rescue Front (UNRF) hands over its flag to the NRM at Karila Airstrip in Arua. Brig. Moses Ali announces the absorption of 2,000 UNRF soldiers in the NRA. Alice Lakwena’s Holy Spirit Movement and Peter * The following were used as sources for part of this timeline: Mugaju (1999), Kaiser and Okumu (2004), and www.IRINnews.org (2006). -

HOSTILE to DEMOCRACY the Movement System and Political Repression in Uganda
HOSTILE TO DEMOCRACY The Movement System and Political Repression in Uganda Human Rights Watch New York $$$ Washington $$$ London $$$ Brussels Copyright 8 August 1999 by Human Rights Watch. All rights reserved. Printed in the United States of America. ISBN 1-56432-239-4 Library of Congress Catalog Card Number 99-65985 Cover design by Rafael Jiménez Addresses for Human Rights Watch 350 Fifth Avenue, 34th Floor, New York, NY 10118-3299 Tel: (212) 290-4700, Fax: (212) 736-1300, E-mail: [email protected] 1522 K Street, N.W., #910, Washington, DC 20005-1202 Tel: (202) 371-6592, Fax: (202) 371-0124, E-mail: [email protected] 33 Islington High Street, N1 9LH London, UK Tel: (171) 713-1995, Fax: (171) 713-1800, E-mail: [email protected] 15 Rue Van Campenhout, 1000 Brussels, Belgium Tel: (2) 732-2009, Fax: (2) 732-0471, E-mail:[email protected] Web Site Address: http://www.hrw.org Listserv address: To subscribe to the list, send an e-mail message to [email protected] with Asubscribe hrw-news@ in the body of the message (leave the subject line blank). Human Rights Watch is dedicated to protecting the human rights of people around the world. We stand with victims and activists to prevent discrimination, to uphold political freedom, to protect people from inhumane conduct in wartime, and to bring offenders to justice. We investigate and expose human rights violations and hold abusers accountable. We challenge governments and those who hold power to end abusive practices and respect international human rights law. We enlist the public and the international community to support the cause of human rights for all. -
Reform Agenda – Political Parties – Political Leaders – Governments – Opposition Groups – Political Violence
Refugee Review Tribunal AUSTRALIA RRT RESEARCH RESPONSE Research Response Number: UGA30810 Country: Uganda Date: 25 October 2006 Keywords: Uganda – Reform Agenda – Political parties – Political leaders – Governments – Opposition groups – Political violence This response was prepared by the Country Research Section of the Refugee Review Tribunal (RRT) after researching publicly accessible information currently available to the RRT within time constraints. This response is not, and does not purport to be, conclusive as to the merit of any particular claim to refugee status or asylum. Questions 1. Please provide information about the group Reform Agenda in Uganda. 2. What was the situation during 2001/2002 for members of Reform Agenda in Uganda? 3. What is the current situation for members of Reform Agenda in Uganda? 4. Which political parties were in power and in opposition in Uganda during 2001/2002 and who were their leaders? 5. Which political party won the 2001 election in Uganda and who was its leader? 6. Were opposition parties subjected to violence / harassment by the government in Uganda during 2001/2002? 7. Which political party is currently in power in Uganda and who is its leader? 8. What are the names of the main opposition political parties currently in Uganda and who are their leaders? 9. Are opposition parties currently subjected to violence / harassment by the government in Uganda? RESPONSE 1. Please provide information about the group Reform Agenda in Uganda. A RRT research response dated 20 July 2004 provides a political history of the Reform Agenda group in Uganda up to that date and lists the group’s office holders in 2002 and 2004 (RRT Country Research 2004, Research Response UGA16861, 20 July – Attachment 1). -
Cmiworkingpaper
CMIWORKINGPAPER Turnaround: The National Resistance Movement and the Re-introduction of a Multiparty System in Uganda Sabiti Makara, Lise Rakner, Lars Svåsand WP 2007: 12 Turnaround: The National Resistance Movement and the Re-introduction of a Multiparty System in Uganda Sabiti Makara, Lise Rakner and Lars Svåsand WP 2007: 12 CMI Working Papers This series can be ordered from: Chr. Michelsen Institute P.O. Box 6033 Postterminalen, N-5892 Bergen, Norway Tel: + 47 55 57 40 00 Fax: + 47 55 57 41 66 E-mail: [email protected] www.cmi.no Price: NOK 50 ISSN 0804-3639 ISBN 978-82-8062-219-8 This report is also available at: www.cmi.no/publications Indexing terms Political systems National resistance Elections Uganda Project title The 2006 Presidential and Parliamentary Elections in Uganda: Institutional and Legal Context Project number 24076 Contents INTRODUCTION ............................................................................................................................................ 1 THE MOVEMENT POLITICAL SYSTEM IN UGANDA .......................................................................... 1 THE DECISION TO RE-INTRODUCE THE MULTI PARTY SYSTEM.......................................................................... 2 WHY DID THE NRM ABANDON ITS MONOPOLY POSITION AND EXPOSE ITSELF TO COMPETITION? ............................................................................................................................................. 3 INTERNAL AND EXTERNAL EXPLANATIONS FOR ORGANISATIONAL CHANGE .................................................. -
Alternative Report
International Federation for Human Rights Foundation for Human Rights Initiative (FHRI) Alternative Report To the Government of Uganda's First Periodic Report Before the United Nations Human Rights Committee “Uganda: a situation of systematic violations of civil and political rights” Acronyms Article 14. The Right to a Fair Hearing Introduction Article 15. Non Retroactive Jurisdiction and Double Jeopardy Country profile Article 16. The Right to Recognition Everywhere as a Person Article 17. The Right to Privacy Article 1. The Right to Self Determination Article 18. Freedom of Thought, Conscience and Religion Article 2. Non Discrimination Article 19. The Right to Hold an Opinion Without Article 3. Equal Rights of Men And Women interference. Article 4. States of Public Emergency Article 21. Right to Peaceful Assembly Article 5. Non Derogeable Rights Article 22. Freedom of Association Article 6. Right to Life Article 23. The Right to Found a Family Article 7. Prohibition from Torture Article 24. Special Measures for the Protection of Children Article 8. Prohibition from Slave Trade Article 25. The Right to Participate in the Conduct of Public Article 9. Right to Liberty Affairs Article 10. Deprivation from Liberty Article 26. The Right not to be discriminated Against Article 11. Civil Suits Article 27. The Right of Ethnic and Religious Minorities Article 12. Freedom of Movement Article 13. The Rights of Aliens Recommendations n° 380/2 - February 2004 “Uganda: a situation of systematic violations of civil and political rights” SUMMARY Acronyms . 4 Introduction . 5 Country profile . 5 Article 1. The Right to Self Determination . 7 Article 2. Non Discrimination . -

Constraints on Women's Political Effectiveness in Uganda Author(S): Anne Marie Goetz Reviewed Work(S): Source: the Journal of Modern African Studies, Vol
No Shortcuts to Power: Constraints on Women's Political Effectiveness in Uganda Author(s): Anne Marie Goetz Reviewed work(s): Source: The Journal of Modern African Studies, Vol. 40, No. 4 (Dec., 2002), pp. 549-575 Published by: Cambridge University Press Stable URL: http://www.jstor.org/stable/3876025 . Accessed: 06/08/2012 15:32 Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at . http://www.jstor.org/page/info/about/policies/terms.jsp . JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. Cambridge University Press is collaborating with JSTOR to digitize, preserve and extend access to The Journal of Modern African Studies. http://www.jstor.org J. of ModernAfrican Studies, 40, 4 (2002), pp. 549-575.- 2002 Cambridge University Press DOI: Io.Ior7/Soo22278Xo2004032 Printed in the United Kingdom No shortcuts to power: constraints on women's political effectiveness in Uganda Anne Marie Goetz* ABSTRACT Numbers of women in public representative office have increased dramati- cally in Uganda since the introduction of the National Resistance Movement's 'no party' system, because affirmative action measures have been taken to reserve seats for them in Parliament and local government. This article offers an assessment of the impact of these measures on women's political effectiveness, examining how far women in Parliament have been able to advance gender equity concerns in key new legislation. -

Contemporary Art in Uganda: a Nexus Between Art and Politics
Contemporary Art in Uganda: A Nexus between Art and Politics Angelo Kakande Volume 1: Text A thesis submitted to the Faculty of Arts, University of the Witwatersrand, Johannesburg, in fulfilment of the requirements for the degree of Doctor of Philosophy Johannesburg, 2008 ii Contemporary Art in Uganda: A Nexus between Art and Politics Abstract The nexus between Uganda’s contemporary art and politics forms the overarching theme of this thesis. The trajectory of Uganda’s contemporary art as a political expression has been retraced. The different political dispensations which have shaped Uganda’s political art have been analysed. The political postures and visual symbols Uganda’s contemporary artists have engaged have been analysed in the context of the wider socio-political discussions which have shaped, and been shaped by, the country. It has been contended that different political epochs have invited response from Uganda’s artists since the early- 1940s. Whereas this debate has been attempted by varied scholars, it has not been rigorously pursued. Formalist discourses seeking to prioritise formal aesthetics have been engaged; conclusions that after 1986 contemporary Ugandan art[ists] became apolitical have been made. With emphasis on two contemporary artists—Fred Kato Mutebi and Bruno Sserunkuuma—this formalist reading has been decentred; the socio-political relevance of Uganda’s contemporary art has been retraced and prioritised. It has been argued that although initially depoliticised through colonial modernity, Uganda’s contemporary artists have been sensitive to the socio-political conditions affecting their space and time; issues of governance and service delivery have preoccupied them albeit in different but often complementary ways.