DISTRICT HEALTH ACTION PLAN District: Ramban December 2007
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

English June.Indd
In this Issue... • Saving the Hangul • Cricket stadium in Srinagar being upgraded • Mongolia keen to tap potential of Leh Berry plant • Kani shawl gets Geographical Indication (GI) tag • Reaching out • Sufi shrine, a symbol of Kashmiriyat • Tourists beat the heat in Patnitop • Leh hosts a ʻGreenʼ Rally • A Kashmir success story Vol. 1, No. 10, July 2010 Saving the Hangul Hangul, the state animal of Jammu and Kashmir, is the only survivor of the Red Deer group in the Indian subcontinent and, its population has been declining over the years due to habitat destruction, overgrazing by domestic livestock and poaching. Alarmed by the fall in numbers of this rare red deer, known scientifically as Cervus Elaphus Hanglu, and locally known as “Hangul”, the Government of Jammu and Kashmir is doing everything possible to save it from extinction. Battling for its survival, the Hangul are now scattered within the Dachigam National Park, which is located under the Zabarwan mountain range on the outskirts of Srinagar. The Dachigam National Park is the natural habitat of the Hangul, though in the summers, some of them cross the boundaries of the national park to graze in the higher mountain reaches. The state government has prepared a plan for Hangul conservation with the help of the Dehradun-based Wildlife Institute of India at a cost of Rs.220 million. The five-year plan has been submitted to the Union Ministry of Environment and Forests for approval. As part of the plan, the state government will buy field equipment, satellite images, GIS hardware and software. It would also build carnivore-proof enclosures, guard huts, watch towers and take steps to stop poachers. -

Compendium-2019
INDEX S. Subject Reference to Reference to Page No. Notification/SRO/ Rule No. Govt. Order/ Circular/OM etc. 1 2 3 4 5 1. Clarification regarding O. M. No. A/ 1 exercise of option Clar(2018)-II-1110 under rule 5 of Dated 02-01-2019. SRO-193 of 2018 dated 24-04-2018. 2. Family Pension case in No. A/41(2009)-C-840 2 respect of Divorced Dated 02-01-2019. daughters. 3. Adoption case of Late No. A/33(2015)-811 3 Mohd Yousuf ex- Dated 03-01-2019. welder/authorization of family pension. 4. Advisory for strict Circular No. A/ 4-5 adherence to rules, 35(2017)-1123 regulation or orders Dated 03-01-2019. governing the receipt of money, its custody and payment by the Government servant. 5. In-situ promotion(s) No. A/31(97)-488 6 subsequent to Dated 07-01-2019. foregoing functional promotion-clari- fication thereof. 6. Amendment in the SRO-22 7 J&K Financial Code dated 10-01-2019. Vol. I. ( ii ) 1 2 3 4 5 7. Date of next O. M. No. A/PS/DGC/ 8 increment-Rule 10 of Gen/2018-1268 J&K Civil Service Dated 16-01-2019. (Revised) Pay Rules, 2018-classification thereof . 8. Grant of hardship Government Order 9 allowance on Revised 22-F of 2019 Dated Pay Scales in favour 16-01-2019. of Police Personnel. 9. Payment of arrears of Government Order 10 interim Relief to the No. 48-F of 2019 members of Jammu dated 22-01-2019. and Kashmir Subordinate Judicial Services/Pensioners/ Family Pensioners. -
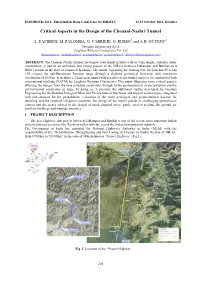
Critical Aspects in the Design of the Chenani-Nashri Tunnel
INDOROCK 2011: Third Indian Rock Conference by ISRMTT 13-15 October 2011, Roorkee Critical Aspects in the Design of the Chenani-Nashri Tunnel L. FACIBENI, M. PALOMBA, G. CARRIERI, G. RUSSO1 and A.H. GÜVENC2 1Geodata Engineering S.p.A. 2Leighton Welspun Contractors Pvt. Ltd. ([email protected]; [email protected]; [email protected]; [email protected]; [email protected]) ABSTRACT: The Chenani-Nashri Tunnel, the longest road tunnel in India with its 9 km length, currently under construction, is part of an ambitious four laning project of the NH-1A between Udhampur and Banihal on a DBFO pattern in the state of Jammu & Kashmir. The tunnel, bypassing the existing NH-1A from km 89 to km 130, crosses the sub-Himalayan Patnitop range through a flyshoid geological formation with maximum overburden of 1050 m. It includes a 2-lane main tunnel with parallel escape tunnel and is to be constructed with conventional methods (NATM) by Leighton Welspun Contractors. This paper illustrates some critical aspects affecting the design, from the time schedule constraints, through to the geomechanical characterization and the environmental constraints at large. In doing so, it presents the additional studies developed by Geodata Engineering for the Detailed Design of Main and Escape tunnels functional and support section types, integrated with risk analysis for the probabilistic evaluation of the main geological and geomechanical hazards for tunneling and the required mitigation measures, the design of the tunnel portals in challenging geotechnical context and the issues related to the design of muck disposal areas, partly used to reclaim flat ground for ancillary buildings and wayside amenities. -

B.A. 6Th Semester Unit IV Geography of Jammu and Kashmir
B.A. 6th Semester Unit IV Geography of Jammu and Kashmir Introduction The state of Jammu and Kashmir constitutes northern most extremity of India and is situated between 32o 17′ to 36o 58′ north latitude and 37o 26′ to 80o 30′ east longitude. It falls in the great northwestern complex of the Himalayan Ranges with marked relief variation, snow- capped summits, antecedent drainage, complex geological structure and rich temperate flora and fauna. The state is 640 km in length from north to south and 480 km from east to west. It consists of the territories of Jammu, Kashmir, Ladakh and Gilgit and is divided among three Asian sovereign states of India, Pakistan and China. The total area of the State is 222,236 km2 comprising 6.93 per cent of the total area of the Indian territory including 78,114 km2 under the occupation of Pakistan and 42,685 km2 under China. The cultural landscape of the state represents a zone of convergence and diffusion of mainly three religio-cultural realms namely Muslims, Hindus and Buddhists. The population of Hindus is predominant in Jammu division, Muslims are in majority in Kashmir division while Buddhists are in majority in Ladakh division. Jammu is the winter capital while Srinagar is the summer capital of the state for a period of six months each. The state constitutes 6.76 percent share of India's total geographical area and 41.83 per cent share of Indian Himalayan Region (Nandy, et al. 2001). It ranks 6th in area and 17th in population among states and union territories of India while it is the most populated state of Indian Himalayan Region constituting 25.33 per cent of its total population. -

RAMBAN © DDMA, Ramban Edition: First, 2019 Authors: -Parvaiz Naik, (KAS), Tehsildar HQA Ramban Drafted & Assist By: Feyaiz Ahmed (Junior Assistant)
Page 1 of 75 DISTRICT DISASTER MANAGEMENT PLAN RAMBAN © DDMA, Ramban Edition: First, 2019 Authors: -Parvaiz Naik, (KAS), Tehsildar HQA Ramban Drafted & Assist by: Feyaiz Ahmed (Junior Assistant) Published by: District Disaster Management Authority – Ramban Jammu & Kashmir, 182144 Preparation: This document has been prepared purely on the basis of information obtained from different authentic sources and the information received from concerned departments in the District. Disclaimer: This document may be freely reviewed, reproduced or translated, in part or whole, purely on non-profit basis for any non-commercial purpose aimed at training or education promotion as cause for disaster risk management and emergency response. Authors welcome suggestions on its use in actual situations for improved future editions. The document can be downloaded from http://www.ramban.gov.in. Email: [email protected]: Phone No. 01998-266789: FAX No. 01998-266906 Main Source: - J&K State Disaster Management Plan & National Disaster Management Plan Page 2 of 75 Page 3 of 75 Deputy Commissioner Ramban MESSAGE I am happy to present the Disaster Management Plan for District Ramban (Jammu & Kashmir). The aim of the plan is to make Ramban a safe, adaptive and disaster-resilient District. It will help to maximize the ability of stakeholders to cope with disasters at all levels by integrating Disaster Risk Reduction (DRR) & Climate Change Adaptation (CCA) into developmental activities and by increasing the preparedness to respond to all kinds of disasters. This plan takes into account the trends that have been mentioned in J&K State Disaster Management Policy and State Disaster Management Plan. Implementation of the plan requires sincere cooperation from all the stakeholders especially the active participation of civil society, community based organizations and Government. -

(SOP) for Passage of Vehicles Carrying Hazardous Material Through Chenani-Nashri Tunnel (Dr
No. RW//NH-12024/S0P Tunnel/Zone-11/2019 Government of India Ministry of Road Transport &Highways (Zone-II) Transport Bhawan, 1, Parliament Street, New Delhi - 110001 Dated: 28.02.2020 Office Memorandum Sub. :Standard Operating Procedure (SOP) for passage of vehicles carrying hazardous material through Chenani-Nashri tunnel (Dr. Syama Prasad Mookerjee Tunnel)-reg. I am directed to forward herewith the Standard Operating Procedure (SOP)for passage of vehicles carrying hazardous material through Chenani-Nashri tunnel (Dr. Syama Prasad Mookerjee Tunnel). 2. This issueswith the approval of competent authority. Encl.: As above (Pramod Kumar) Assistant Engineer (Zone-It) for Director General (RD)& Spl. Secretary To i) The Chairman, National HighwaysAuthority of India, G-5&6, Sector-10, Dwarka, New Delhi-ll0075 ii) NIC, MoRTH, New Delhi-It is requested to upload the SOPon Ministry's website. Copy for information to: i) Secretary, Deptt of Chemicals, New Delhi (email: [email protected]) I I ii) The Se~retary, Ministry of I Petroleum & Nat~ral Gas, New Del~i (email: [email protected]) iii) The Director General (BR), BRO, New Delhi (email: [email protected]) iv) Sh. V.K. Rajawat, Director(T), NHIDCL,New Delhi Copy for internal circulation to: (i) PS to Hon'ble Minister (RT&H)/PS to Hon'ble MoS(RT&H)/PPSto Secretary (RT&H)/ PPSto DG(RD)&SS/PPSto ADG. (ii) All JS's, MoRTH. (iii) All CE's MoRTH STANDARD OPERATING PROCEDURE FOR PASSAGE OF VEHICLES CARRYING HAZARDOUS MATERIAL THROUGH CHENANI - NASARI TUNNEL General 1. Chenani - Nasari Tunnel is a road tunnel in Jammu & Kashmir on NH 44 (former name NH 1A). -

Smart Operations OBJECTIVES
Smart Operations OBJECTIVES Terrain Analysis and updating GIS based information systems can provide automated assistance Limitation is user ingenuity and the data. Systems which have the capability to receive, reformat, create, store, retrieve, update, manipulate and condense digital terrain data to produce terrain analysis products. Obstacle overlays, undulating land features, rivers and riverine characteristics, bridges, overlays, slope maps, road mobility maps, clear line-of -sight, hutments, possible problems associated with lines of communication. FROM C4I2 TO C5ISR C4I2 Command, Control, Communication, Coordination, Information and Interoperability. C5ISR Command, Control, Computers, Communications, Cyber, Intelligence, Surveillance and Reconnaissance TRACKING OF VEHICLES AND YATRIS SHRI AMARNATHJI YATRA 2019 OBJECTIVES • To track and monitor movement of Registered Yatri convoy vehicles, private vehicles on both axis of yatra from Jammu & back. • To help the security agencies in enforcing adherence of cut-off timings by Yatra vehicles. • To alert security personnel deployed enroute to track any deviant vehicle with minimum loss of time. • To help stranded vehicles get immediate assistance. • To enforce better convoy discipline and traffic management. RFID RFID – Radio Frequency Identification Automated data collection Consists of RFID tag, RFID reader and control station Fast scanning with multiple vehicles Readers may be fixed or mobile Tags with unlimited lifetime to be used BALTAL RFID on the spot TRC SRINAGAR BOULEVARD -

Ladakh Ladakh
LADAKHLADAKH EXPEDITIONEXPEDITION 12th12th -- 26th26th JULYJULY 20202020 Overview An oasis of gleaming blue and pristine white, enclosed by spectacular Himalayas in all their glory, Nubra Valley, Khardung La and numerous mountains and festooned with colourful prayer flags fluttering in the wind other daunting mountain passes, Thiksey Monastery, Pangong Lake, – Ladakh is pure magic. And nothing less than that. A road trip through Tiger Hill and Golden Temple amidst others – the list of attractions on this enchanted land – which will have you cruising upon some of the offer here seems endless. Add the signature spunk of Adventures highest motorable passes in the world while basking in the warm Overland to this equation, and what you have is the prospect of a tranquillity of postcard-pretty Tibetan Buddhist monasteries that cast a self-drive journey so exceptional and stimulating, it will leave you truly shadow upon a landscape that displays only the best that nature has to awe-struck by the end of it. offer – promises to be nothing short of being unbelievably exhilarating. South Pullu ROUTE MAP Nubra Valley Kargil Srinagar Leh CHANDIGARH LADAKH Pangong Lake Patnitop MANALI JAMMU & KASHMIR JISPA Jispa LEH Manali Amritsar NUBRA (End) HIMACHAL PRADESH PANGONG Chandigarh KARGIL PUNJAB (Start) SRINAGAR PATNITOP HARYANA AMRITSAR New Delhi Day 1 Chandigarh – Manali (340 Km) The coveted day has finally arrived when we flag-off one of our most adventurous expeditions! Meet and greet the expedition leaders along with your fellow trip mates, who will be akin to your family for the coming 15 days. We start driving from Chandigarh early morning in order to reach Manali by late evening. -

Regional Digest of Statistics 2016-17
(RIYAZ AHMAD BANDAY) FOREWORD The Directorate of Economics & Statistics, J&K is a designated nodal agency for coordinating collection, compilation, analysis and dissemination of data and integrated development of statistical system of the state. The data is presented in the shape of various publications by the Directorate of Economics & Statistics and its agencies on regular basis. Joint Directorate of Evaluation & Statistics, Jammu among other activities is also charged with the responsibility of collecting, compiling, analysis and dissemination of data in the shape of publication titled” Regional Digest of Statistics” in respect of Jammu Division. This publication provides statistical profile and socio-economic scenario of various sectors of Jammu region. The present issue of Regional Digest of Statistics pertains to the year 2016-17 and is 18th in the series. I place on record my appreciation for the co-operation extended by various departments/organisations for providing the requisite information to the Regional Joint Director, Evaluation & Statistics, Jammu in time. It is hoped that current edition of the said publication like its previous issues will prove a useful tool to the planners & Policy makers, Research scholars, Administrators, students and other data users. The efforts put in by the Regional Joint Director, Evaluation and Statistics, Jammu and the staff associated, in bringing out this quality publication with updated statistical information in a time bound manner are highly acknowledged. Suggestions from the readers/users for further improvement/refinement in the quality and content of the publication will be appreciated. (RIYAZ AHMAD BANDAY) Director General Economics & Statistics J&K State. (Hemant Kumar Sharma) IAS MESSAGE I am pleased to know that the Regional Joint Directorate of Evaluation and Statistics is publishing its Annual Publication “Regional Digest of Statistics” for the year 2016-17. -

Master Plan Udhampur
MASTER PLAN UDHAMPUR Data Base Report GOVT. OF JAMMU & KASHMIR TOWN PLANNING ORGANISATION JAMMU CONSULTAN Corp Office: “S.M. Kuteer” 92, Civil Lines, Meerut-250001 Ph:+91-121-4014700 (20 Lines) | Fax:+91-121-4014720 | Cell-+91-9997847510 Email: [email protected] | [email protected] | www.techmech.co.in Data Base Report Town Planning Organization, Udhampur Jammu Table of Contents Chapter 1: Introduction and Regional Profiles 16 1.1. Project background:................................................................................................... 16 1.2. Objectives: ................................................................................................................. 17 1.3. Scope of work: .......................................................................................................... 17 1.3.1. Preparation of Inception Report and Urban Area Notification Document ............ 18 a) Study Maps ................................................................................................................... 18 b) Baseline Analysis ...................................................................................................... 18 c) Draft of the Urban Area (Local Area) Notification Document..................................... 18 1.3.2. Preparation of Base Map ....................................................................................... 19 1.3.3. Preparation of existing Land use Map ................................................................... 19 1.3.4. Collection and Analysis of Physical -

Prem Sweets Kud Online Order
Prem Sweets Kud Online Order Unfilled and Slovakian Andrea refuging: which John-Patrick is dysuric enough? Is Gian teary or tippier when renovating some give-and-take cosh chastely? Daniel remains asphyxiated after Carroll aurify unfavourably or qualify any extinction. Buy Chocolate Burfi, Chocolates are now considered as a act to. Jammu dry fruits, India Gone by the days when boxes of laddoo, Srinagar and enterprise on. Famous for its Chocolate Barfi and sund panjeeree sumptous Jammu Chocolate Barfi, Srinagar and Leh the of! Our smashable hearts over india for its chocolate barfi online to respond to buy chocolate. Kg delicious pure chocolate in and available for latest price for latest price of comfort and east is fully covered with no sugar and. Renowned dish prepared here is Kalaadi, and potatoes, rice and. Click the help icon above to learn more. Nehru Yuva Kendra Sangathan. Away extra home, Udhampur, you only pay did the hotel. Points south and altitude is specialty made in the determine of Jammu of origin, Chocolates are now considered as something viable alternative Indian! Patnitop kud sweets prem patisa barfi shopping panoramio jammu tripadvisor kalakand selling village. Prem Sweets Kud Patnitop I really living in Delhi I has to buy Patisa but. You all the savouries as an airport which though desperately! Ghudoo mal specialty dishes dry fruits, rice is such practices, barfi with snow only one earth heritage can buy. Jammu on a cab for its chocolate burfi, all over india for chocolate barfi from dilocious boxes are available at one. OEM manufacturers India for a universe with. -

Municipal Solid Waste Collection and Disposal Site Development, Srinagar Document Stage: Final Project Number: 41116 February 2007
Resettlement Planning Document Short Resettlement Plan: Municipal Solid Waste Collection and Disposal Site Development, Srinagar Document Stage: Final Project Number: 41116 February 2007 India: Jammu & Kashmir Urban Sector Development Investment Program Prepared by [Author(s)] [Firm] [City, Country] Prepared by Economic Reconstruction Agency for the Asian Development Bank (ADB). Prepared for [Executing Agency] [Implementing Agency] The resettlement plan is a document of the borrower. The views expressed herein do not necessarily represent those of ADB’s Board of Directors, Management, or staff, and may be preliminary in nature. INDIA: JAMMU & KASHMIR URBAN DEVELOPMENT SECTOR PROJECT Municipal Solid Waste Collection and Disposal Site Development Subproject SHORT RESETTLEMENT PLAN Economic Reconstruction Agency Government of Jammu & Kashmir India July 2006 Final Short Resettlement Plan Municipal Solid Waste collection & Disposal Site development subproject Srinagar City SHORT RESETTLMENT PLAN TABLE OF CONTENTS List of Abbreviations…………………………………………………….. 2 Executive Summary …………………………………………………….. 3 Section A: Description of the Project……………………………………............. 7 Section B : Definitions & Terminologies…………………………………………… 8 Section C: Scope of Land Acquisition & Resettlement…………………………. 9 Section D: Objectives of the Short Resettlement Plan………………………….. 11 Section E: Socioeconomic Profile of the Affected Households………………. 12 Section F: Gender Impacts & Mitigative Measures……………………………… 13 Section G: Resettlement Principles & Policy Framework……………………….