Unilateral Opercular Polymicrogyria in a Girl with 22Q13 Deletion Syndrome
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dual Proteome-Scale Networks Reveal Cell-Specific Remodeling of the Human Interactome
bioRxiv preprint doi: https://doi.org/10.1101/2020.01.19.905109; this version posted January 19, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Dual Proteome-scale Networks Reveal Cell-specific Remodeling of the Human Interactome Edward L. Huttlin1*, Raphael J. Bruckner1,3, Jose Navarrete-Perea1, Joe R. Cannon1,4, Kurt Baltier1,5, Fana Gebreab1, Melanie P. Gygi1, Alexandra Thornock1, Gabriela Zarraga1,6, Stanley Tam1,7, John Szpyt1, Alexandra Panov1, Hannah Parzen1,8, Sipei Fu1, Arvene Golbazi1, Eila Maenpaa1, Keegan Stricker1, Sanjukta Guha Thakurta1, Ramin Rad1, Joshua Pan2, David P. Nusinow1, Joao A. Paulo1, Devin K. Schweppe1, Laura Pontano Vaites1, J. Wade Harper1*, Steven P. Gygi1*# 1Department of Cell Biology, Harvard Medical School, Boston, MA, 02115, USA. 2Broad Institute, Cambridge, MA, 02142, USA. 3Present address: ICCB-Longwood Screening Facility, Harvard Medical School, Boston, MA, 02115, USA. 4Present address: Merck, West Point, PA, 19486, USA. 5Present address: IQ Proteomics, Cambridge, MA, 02139, USA. 6Present address: Vor Biopharma, Cambridge, MA, 02142, USA. 7Present address: Rubius Therapeutics, Cambridge, MA, 02139, USA. 8Present address: RPS North America, South Kingstown, RI, 02879, USA. *Correspondence: [email protected] (E.L.H.), [email protected] (J.W.H.), [email protected] (S.P.G.) #Lead Contact: [email protected] bioRxiv preprint doi: https://doi.org/10.1101/2020.01.19.905109; this version posted January 19, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. -

A Framework to Identify Contributing Genes in Patients with Phelan
A framework to identify contributing genes in patients with Phelan-McDermid syndrome Anne-Claude Tabet, Thomas Rolland, Marie Ducloy, Jonathan Levy, Julien Buratti, Alexandre Mathieu, Damien Haye, Laurence Perrin, Céline Dupont, Sandrine Passemard, et al. To cite this version: Anne-Claude Tabet, Thomas Rolland, Marie Ducloy, Jonathan Levy, Julien Buratti, et al.. A frame- work to identify contributing genes in patients with Phelan-McDermid syndrome. Genomic Medicine, Springer Verlag, 2017, 2, pp.32. 10.1038/s41525-017-0035-2. hal-01738521 HAL Id: hal-01738521 https://hal.umontpellier.fr/hal-01738521 Submitted on 20 Mar 2018 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution| 4.0 International License www.nature.com/npjgenmed ARTICLE OPEN A framework to identify contributing genes in patients with Phelan-McDermid syndrome Anne-Claude Tabet 1,2,3,4, Thomas Rolland2,3,4, Marie Ducloy2,3,4, Jonathan Lévy1, Julien Buratti2,3,4, Alexandre Mathieu2,3,4, Damien Haye1, Laurence Perrin1, Céline Dupont 1, Sandrine -

Whole Exome Sequencing in Families at High Risk for Hodgkin Lymphoma: Identification of a Predisposing Mutation in the KDR Gene
Hodgkin Lymphoma SUPPLEMENTARY APPENDIX Whole exome sequencing in families at high risk for Hodgkin lymphoma: identification of a predisposing mutation in the KDR gene Melissa Rotunno, 1 Mary L. McMaster, 1 Joseph Boland, 2 Sara Bass, 2 Xijun Zhang, 2 Laurie Burdett, 2 Belynda Hicks, 2 Sarangan Ravichandran, 3 Brian T. Luke, 3 Meredith Yeager, 2 Laura Fontaine, 4 Paula L. Hyland, 1 Alisa M. Goldstein, 1 NCI DCEG Cancer Sequencing Working Group, NCI DCEG Cancer Genomics Research Laboratory, Stephen J. Chanock, 5 Neil E. Caporaso, 1 Margaret A. Tucker, 6 and Lynn R. Goldin 1 1Genetic Epidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 2Cancer Genomics Research Laboratory, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 3Ad - vanced Biomedical Computing Center, Leidos Biomedical Research Inc.; Frederick National Laboratory for Cancer Research, Frederick, MD; 4Westat, Inc., Rockville MD; 5Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; and 6Human Genetics Program, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD, USA ©2016 Ferrata Storti Foundation. This is an open-access paper. doi:10.3324/haematol.2015.135475 Received: August 19, 2015. Accepted: January 7, 2016. Pre-published: June 13, 2016. Correspondence: [email protected] Supplemental Author Information: NCI DCEG Cancer Sequencing Working Group: Mark H. Greene, Allan Hildesheim, Nan Hu, Maria Theresa Landi, Jennifer Loud, Phuong Mai, Lisa Mirabello, Lindsay Morton, Dilys Parry, Anand Pathak, Douglas R. Stewart, Philip R. Taylor, Geoffrey S. Tobias, Xiaohong R. Yang, Guoqin Yu NCI DCEG Cancer Genomics Research Laboratory: Salma Chowdhury, Michael Cullen, Casey Dagnall, Herbert Higson, Amy A. -

Combined Deletion 18Q22.2 and Duplication/Triplication 18Q22.1 Causes Microcephaly, Mental Retardation and Leukencephalopathy
Gene 523 (2013) 92–98 Contents lists available at SciVerse ScienceDirect Gene journal homepage: www.elsevier.com/locate/gene Short communication Combined deletion 18q22.2 and duplication/triplication 18q22.1 causes microcephaly, mental retardation and leukencephalopathy Sylvie Nguyen-Minh a, Katrin Drossel b, Denise Horn c, Imma Rost d, Birgit Spors e, Angela M. Kaindl a,b,f,⁎ a Department of Pediatric Neurology, Charité-Universitätsmedizin Berlin, Campus Virchow-Klinikum, Augustenburger Platz 1, 13353 Berlin, Germany b SPZ Pediatric Neurology, Charité-Universitätsmedizin Berlin, Campus Virchow-Klinikum, Augustenburger Platz 1, 13353 Berlin, Germany c Institute of Human Genetics, Charité-Universitätsmedizin Berlin, Campus Virchow-Klinikum, Augustenburger Platz 1, 13353 Berlin, Germany d Center for Human Genetics and Laboratory Medicine, Lochhamerstr. 29, 82152 Martinsried, Germany e Department of Pediatric Radiology, Charité-Universitätsmedizin Berlin, Campus Virchow-Klinikum, Augustenburger Platz 1, 13353 Berlin, Germany f Institute of Neuroanatomy and Cell Biology, Charité-Universitätsmedizin Berlin, Campus Mitte, Charitéplatz 1, 10115 Berlin, Germany article info abstract Article history: Chromosome 18 abnormalities rank among the most common autosomal anomalies with 18q being the most fre- Accepted 15 March 2013 quently affected. A deletion of 18q has been attributed to microcephaly, mental retardation, short stature, facial Available online 5 April 2013 dysmorphism, myelination disorders, limb and genitourinary malformations and -

The Human TTAGGG Repeat Factors 1 and 2 Bind to a Subset of Interstitial Telomeric Sequences and Satellite Repeats
npg Extratelomeric binding of TRF1 and TRF2 Cell Research (2011) 21:1028-1038. 1028 © 2011 IBCB, SIBS, CAS All rights reserved 1001-0602/11 $ 32.00 npg ORIGINAL ARTICLE www.nature.com/cr The human TTAGGG repeat factors 1 and 2 bind to a subset of interstitial telomeric sequences and satellite repeats Thomas Simonet1, Laure-Emmanuelle Zaragosi2, Claude Philippe3, Kevin Lebrigand2, Clémentine Schouteden1, Adeline Augereau1, 3, Serge Bauwens1, Jing Ye1, 3, Marco Santagostino4, Elena Giulotto4, Frederique Magdinier1, Béatrice Horard1, Pascal Barbry2, Rainer Waldmann2, Eric Gilson1, 3, 5 1Laboratoire de Biologie Moléculaire de la Cellule-UMR 5239 CNRS/ENS Lyon/ Université Lyon, Ecole Normale Supérieure de Lyon, 46 allée d’Italie, Lyon 69364, France; 2CNRS and University of Nice Sophia Antipolis, Institut de Pharmacologie Molé- culaire et Cellulaire, 06560 Sophia Antipolis, France; 3Laboratory of Biology and Pathology of Genomes of University of Nice Sophia-Antipolis, CNRS UMR6267/INSERM U998, Faculty of Medicine, Nice, France; 4Dipartimento di Genetica e Microbiologia Adriano Buzzati-Traverso, Università di Pavia, Pavia, Italy; 5Department of Medical Genetics, CHU of Nice, Nice, France The study of the proteins that bind to telomeric DNA in mammals has provided a deep understanding of the mech- anisms involved in chromosome-end protection. However, very little is known on the binding of these proteins to nontelomeric DNA sequences. The TTAGGG DNA repeat proteins 1 and 2 (TRF1 and TRF2) bind to mammalian te- lomeres as part of the shelterin complex and are essential for maintaining chromosome end stability. In this study, we combined chromatin immunoprecipitation with high-throughput sequencing to map at high sensitivity and resolution the human chromosomal sites to which TRF1 and TRF2 bind. -

University of Groningen Unravelling the Genetic Basis of Hereditary
University of Groningen Unravelling the genetic basis of hereditary disorders by high-throughput exome sequencing strategies Jazayeri, Omid IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2016 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Jazayeri, O. (2016). Unravelling the genetic basis of hereditary disorders by high-throughput exome sequencing strategies. University of Groningen. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 07-10-2021 Unravelling the genetic basis of hereditary disorders by high-throughput exome sequencing strategies Omid Jazayeri | Omid Jazayeri Unravelling the genetic basis of hereditary disorders by high-throughput exome sequencing strategies The research presented in this thesis was performed at the Department of Genetics, Uiversity Medical Center Groningen, University of Groningen, Groningen, The Netherlands. -

Variation in Protein Coding Genes Identifies Information Flow
bioRxiv preprint doi: https://doi.org/10.1101/679456; this version posted June 21, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Animal complexity and information flow 1 1 2 3 4 5 Variation in protein coding genes identifies information flow as a contributor to 6 animal complexity 7 8 Jack Dean, Daniela Lopes Cardoso and Colin Sharpe* 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Institute of Biological and Biomedical Sciences 25 School of Biological Science 26 University of Portsmouth, 27 Portsmouth, UK 28 PO16 7YH 29 30 * Author for correspondence 31 [email protected] 32 33 Orcid numbers: 34 DLC: 0000-0003-2683-1745 35 CS: 0000-0002-5022-0840 36 37 38 39 40 41 42 43 44 45 46 47 48 49 Abstract bioRxiv preprint doi: https://doi.org/10.1101/679456; this version posted June 21, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Animal complexity and information flow 2 1 Across the metazoans there is a trend towards greater organismal complexity. How 2 complexity is generated, however, is uncertain. Since C.elegans and humans have 3 approximately the same number of genes, the explanation will depend on how genes are 4 used, rather than their absolute number. -
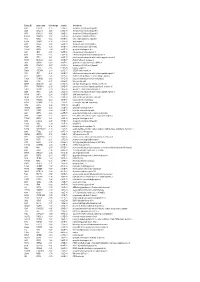
Entrez ID Gene Name Fold Change Q-Value Description
Entrez ID gene name fold change q-value description 4283 CXCL9 -7.25 5.28E-05 chemokine (C-X-C motif) ligand 9 3627 CXCL10 -6.88 6.58E-05 chemokine (C-X-C motif) ligand 10 6373 CXCL11 -5.65 3.69E-04 chemokine (C-X-C motif) ligand 11 405753 DUOXA2 -3.97 3.05E-06 dual oxidase maturation factor 2 4843 NOS2 -3.62 5.43E-03 nitric oxide synthase 2, inducible 50506 DUOX2 -3.24 5.01E-06 dual oxidase 2 6355 CCL8 -3.07 3.67E-03 chemokine (C-C motif) ligand 8 10964 IFI44L -3.06 4.43E-04 interferon-induced protein 44-like 115362 GBP5 -2.94 6.83E-04 guanylate binding protein 5 3620 IDO1 -2.91 5.65E-06 indoleamine 2,3-dioxygenase 1 8519 IFITM1 -2.67 5.65E-06 interferon induced transmembrane protein 1 3433 IFIT2 -2.61 2.28E-03 interferon-induced protein with tetratricopeptide repeats 2 54898 ELOVL2 -2.61 4.38E-07 ELOVL fatty acid elongase 2 2892 GRIA3 -2.60 3.06E-05 glutamate receptor, ionotropic, AMPA 3 6376 CX3CL1 -2.57 4.43E-04 chemokine (C-X3-C motif) ligand 1 7098 TLR3 -2.55 5.76E-06 toll-like receptor 3 79689 STEAP4 -2.50 8.35E-05 STEAP family member 4 3434 IFIT1 -2.48 2.64E-03 interferon-induced protein with tetratricopeptide repeats 1 4321 MMP12 -2.45 2.30E-04 matrix metallopeptidase 12 (macrophage elastase) 10826 FAXDC2 -2.42 5.01E-06 fatty acid hydroxylase domain containing 2 8626 TP63 -2.41 2.02E-05 tumor protein p63 64577 ALDH8A1 -2.41 6.05E-06 aldehyde dehydrogenase 8 family, member A1 8740 TNFSF14 -2.40 6.35E-05 tumor necrosis factor (ligand) superfamily, member 14 10417 SPON2 -2.39 2.46E-06 spondin 2, extracellular matrix protein 3437 -

Content Based Search in Gene Expression Databases and a Meta-Analysis of Host Responses to Infection
Content Based Search in Gene Expression Databases and a Meta-analysis of Host Responses to Infection A Thesis Submitted to the Faculty of Drexel University by Francis X. Bell in partial fulfillment of the requirements for the degree of Doctor of Philosophy November 2015 c Copyright 2015 Francis X. Bell. All Rights Reserved. ii Acknowledgments I would like to acknowledge and thank my advisor, Dr. Ahmet Sacan. Without his advice, support, and patience I would not have been able to accomplish all that I have. I would also like to thank my committee members and the Biomed Faculty that have guided me. I would like to give a special thanks for the members of the bioinformatics lab, in particular the members of the Sacan lab: Rehman Qureshi, Daisy Heng Yang, April Chunyu Zhao, and Yiqian Zhou. Thank you for creating a pleasant and friendly environment in the lab. I give the members of my family my sincerest gratitude for all that they have done for me. I cannot begin to repay my parents for their sacrifices. I am eternally grateful for everything they have done. The support of my sisters and their encouragement gave me the strength to persevere to the end. iii Table of Contents LIST OF TABLES.......................................................................... vii LIST OF FIGURES ........................................................................ xiv ABSTRACT ................................................................................ xvii 1. A BRIEF INTRODUCTION TO GENE EXPRESSION............................. 1 1.1 Central Dogma of Molecular Biology........................................... 1 1.1.1 Basic Transfers .......................................................... 1 1.1.2 Uncommon Transfers ................................................... 3 1.2 Gene Expression ................................................................. 4 1.2.1 Estimating Gene Expression ............................................ 4 1.2.2 DNA Microarrays ...................................................... -

Genetic Analysis of Amyotrophic Lateral Sclerosis Identifies Contributing Pathways and Cell Types
University of Massachusetts Medical School eScholarship@UMMS Open Access Publications by UMMS Authors 2021-01-15 Genetic analysis of amyotrophic lateral sclerosis identifies contributing pathways and cell types Sara Saez-Atienzar National Institutes of Health Et al. Let us know how access to this document benefits ou.y Follow this and additional works at: https://escholarship.umassmed.edu/oapubs Part of the Genetics and Genomics Commons, Molecular and Cellular Neuroscience Commons, Nervous System Diseases Commons, and the Neurology Commons Repository Citation Saez-Atienzar S, Landers JE. (2021). Genetic analysis of amyotrophic lateral sclerosis identifies contributing pathways and cell types. Open Access Publications by UMMS Authors. https://doi.org/ 10.1126/sciadv.abd9036. Retrieved from https://escholarship.umassmed.edu/oapubs/4570 Creative Commons License This work is licensed under a Creative Commons Attribution-Noncommercial 4.0 License This material is brought to you by eScholarship@UMMS. It has been accepted for inclusion in Open Access Publications by UMMS Authors by an authorized administrator of eScholarship@UMMS. For more information, please contact [email protected]. SCIENCE ADVANCES | RESEARCH ARTICLE GENETICS Copyright © 2021 The Authors, some rights reserved; Genetic analysis of amyotrophic lateral sclerosis exclusive licensee American Association identifies contributing pathways and cell types for the Advancement Sara Saez-Atienzar1*†, Sara Bandres-Ciga2,3†, Rebekah G. Langston4, Jonggeol J. Kim2, of Science. No claim to 5 6,7,8 original U.S. Government Shing Wan Choi , Regina H. Reynolds , the International ALS Genomics Consortium, Works. Distributed 1,9 1 10 ITALSGEN, Yevgeniya Abramzon , Ramita Dewan , Sarah Ahmed , under a Creative 11 1 7,8 4 2,12 John E. -

Downloaded from Ensembl
UCSF UC San Francisco Electronic Theses and Dissertations Title Detecting genetic similarity between complex human traits by exploring their common molecular mechanism Permalink https://escholarship.org/uc/item/1k40s443 Author Gu, Jialiang Publication Date 2019 Peer reviewed|Thesis/dissertation eScholarship.org Powered by the California Digital Library University of California by Submitted in partial satisfaction of the requirements for degree of in in the GRADUATE DIVISION of the UNIVERSITY OF CALIFORNIA, SAN FRANCISCO AND UNIVERSITY OF CALIFORNIA, BERKELEY Approved: ______________________________________________________________________________ Chair ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ Committee Members ii Acknowledgement This project would not have been possible without Prof. Dr. Hao Li, Dr. Jiashun Zheng and Dr. Chris Fuller at the University of California, San Francisco (UCSF) and Caribou Bioscience. The Li lab grew into a multi-facet research group consist of both experimentalists and computational biologists covering three research areas including cellular/molecular mechanism of ageing, genetic determinants of complex human traits and structure, function, evolution of gene regulatory network. Labs like these are the pillar of global success and reputation -

Enrichment of Mutations in Chromatin Regulators in People with Rett Syndrome Lacking Mutations in MECP2
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Genet Med Manuscript Author . Author manuscript; Manuscript Author available in PMC 2016 November 14. Enrichment of mutations in chromatin regulators in people with Rett Syndrome lacking mutations in MECP2 Samin A. Sajan, PhD1,2,#, Shalini N. Jhangiani, MS3, Donna M. Muzny, MS3, Richard A. Gibbs, PhD3,4, James R. Lupski, MD, PhD3,4,5, Daniel G. Glaze, MD1, Walter E. Kaufmann, MD6, Steven A. Skinner, MD7, Fran Anese7, Michael J. Friez, PhD7, Lane Jane, RN8, Alan K. Percy, MD8, and Jeffrey L. Neul, MD, PhD1,2,4,# 1Section of Child Neurology and Developmental Neuroscience, Department of Pediatrics, Baylor College of Medicine, Houston, Texas, USA 2Jan and Dan Duncan Neurological Research Institute, Texas Children's Hospital, Houston, Texas, USA 3Human Genome Sequencing Center, Baylor College of Medicine, Houston, Texas, USA 4Department of Molecular and Human Genetics, Baylor College of Medicine, Houston, Texas, USA 5Department of Pediatrics, Baylor College of Medicine and Texas Children's Hospital, Houston, Texas, USA 6Department of Neurology, Boston Children's Hospital, Boston, Massachusetts, USA 7Greenwood Genetic Center, Greenwood, South Carolina, USA 8Department of Pediatrics, University of Alabama at Birmingham, Birmingham, Alabama, USA Abstract Purpose—Rett Syndrome (RTT) is a neurodevelopmental disorder caused primarily by de novo mutations (DNMs) in MECP2 and sometimes in CDKL5 and FOXG1. However, some RTT cases lack mutations in these genes. Methods—Twenty-two RTT cases without apparent MECP2, CDKL5, and FOXG1 mutations were subjected to both whole exome sequencing and single nucleotide polymorphism array-based copy number variant (CNV) analyses. Results—Three cases had MECP2 mutations initially missed by clinical testing.