URI Dive Medical V2018 2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Darling Marine Center Local Shore Diving Guide
Darling Marine Center Local Shore Diving Guide University of Maine Scientific Diving Program Table of Contents Recommended Equipment List……………………………………………………………..2 Local Information…………………………………………………………………………...3 Recompression Chambers…………………………………………………………………..3 General Emergency Action Plan…………………………………………………………….3-4 Documentation……………………………………………………………………………….4 Dive Sites DMC Pier……………………………………………………………………………5-6 Kresge Point………………………………………………………………………….7-8 Lowes Cove Mooring Field…………………………………………………………..9-10 Pemaquid Point……………………………………………………………………….11-12 Rachel Carson Preserve………………………………………………………………13-15 Sand Cove…………………………………………………………………………….16-17 Thread of life…………………………………………………………………………18-19 Appendix………………………………………………………………………………………20 1 Recommended Equipment List • Dive flag • DAN oxygen and first aid kit • Spare tank • Extra weights • Save-a-dive kit • Dive slate/underwater paper (recording purposes) Recommended Personal Equipment • Exposure suit- minimum7mm wetsuit o Booties o Gloves o Hood o Wool socks • Fins • BCD • Mask, Snorkel • Weights • Surface marker buoy • Dive watch • Dive computer • Knife/cutting tool 2 Local Information: Fire, Medical, Police 911 Emergency Dispatch Lincoln County Emergency (207)563-3200 Center Nearest Hospital Lincoln Health-Miles (207)563-1234 Campus USCG Boothbay (207)633-2661 Divers Alert Network Emergency hotline 1-919-684-9111 Medical information 1-919-684-2948 Diving Safety Officer Christopher Rigaud (207)563-8273 Recompression Chambers: In the event of a diving accident, call 911 and facilitate transport of victim to a hospital or medical facility. The medical staff will determine whether hyperbaric treatment is needed. St. Mary’s Regional Lewiston, ME (207)777-8331 Will NOT accept Medical Center divers after 4:30pm St. Joseph’s Hospital Bangor, ME (207)262-1550 Typically, available after hours Wound and Beverly, MA (978)921-1210 Hyperbaric Medicine Basic Emergency Information: See Appendix for the approved Emergency Action Plan by the UMaine DCB. -

Medical Aspects of Harsh Environments, Volume 2, Chapter
Military Diving Operations and Medical Support Chapter 31 MILITARY DIVING OPERATIONS AND MEDICAL SUPPORT † RICHARD D. VANN, PHD*; AND JAMES VOROSMARTI, JR, MD INTRODUCTION BREATH-HOLD DIVING CENTRAL NERVOUS SYSTEM OXYGEN TOXICITY IN COMBAT DIVERS UNDERWATER BREATHING APPARATUS Open-Circuit Self-Contained Underwater Breathing Apparatus: The Aqualung Surface-Supplied Diving Closed-Circuit Oxygen Scuba Semiclosed Mixed-Gas Scuba Closed-Circuit, Mixed-Gas Scuba THE ROLE OF RESPIRATION IN DIVING INJURIES Carbon Dioxide Retention and Dyspnea Interactions Between Gases and Impaired Consciousness Individual Susceptibility to Impaired Consciousness DECOMPRESSION PROCEDURES No-Stop (No-Decompression) Dives In-Water Decompression Stops Surface Decompression Repetitive and Multilevel Diving Dive Computers Nitrogen–Oxygen Diving Helium–Oxygen and Trimix Diving Omitted Decompression Flying After Diving and Diving at Altitude The Safety of Decompression Practice SATURATION DIVING Atmospheric Control Infection Hyperbaric Arthralgia Depth Limits Decompression THERMAL PROTECTION AND BUOYANCY TREATMENT OF DECOMPRESSION SICKNESS AND ARTERIAL GAS EMBOLISM Therapy According to US Navy Treatment Tables Decompression Sickness in Saturation Diving MEDICAL STANDARDS FOR DIVING SUBMARINE RESCUE AND ESCAPE SUMMARY *Captain, US Navy Reserve (Ret); Divers Alert Network, Center for Hyperbaric Medicine and Environmental Physiology, Box 3823, Duke University Medical Center, Durham, North Carolina 27710 †Captain, Medical Corps, US Navy (Ret); Consultant in Occupational, Environmental, and Undersea Medicine, 16 Orchard Way South, Rockville, Maryland 20854 955 Military Preventive Medicine: Mobilization and Deployment INTRODUCTION Divers breathe gases and experience pressure land) teams and two SEAL delivery vehicle (SDV) changes that can cause different injuries from those teams. SEALs are trained for reconnaissance and encountered by most combatant or noncombatant direct action missions at rivers, harbors, shipping, military personnel. -

PARTICIPANT INFORMATION SHEET DAN Rebreather Study 2020 - Caustic Cocktail IRB #025-20-20 (Expiry: 2021-08-05)
PARTICIPANT INFORMATION SHEET DAN Rebreather Study 2020 - Caustic Cocktail IRB #025-20-20 (expiry: 2021-08-05) CONCISE SUMMARY This survey aims to collect data from rebreather divers regarding their experiences with caustic cocktail(s) while diving. You qualify for participation in this study if you are a certified rebreather diver and you have experienced a caustic cocktail or dived with someone who experienced a caustic cocktail. There are no individual benefits and no currently foreseeable risks to you in participating in this study. If you are interested in learning more about the study, please continue reading and review the following pages carefully before agreeing to participate. INTRODUCTION You are invited to complete a short survey about rebreather diving. The study is entirely sponsored by DAN. PURPOSE OF THE STUDY The purpose of this study is to collect information from adult rebreather divers and their experiences with a “Caustic Cocktail”. BACKGROUND When water mixes with the carbon-dioxide absorbent in rebreathers, e.g. due to a leak in the unit, a solution of caustic soda is produced. When a diver ingests this poisonous mixture, known as a “Caustic Cocktail”, it is important to provide appropriate first aid. It is uncertain how common suffering a caustic cocktail is among certified rebreather divers, or what immediate first-aid treatments are being employed. This survey will gather information on rebreather divers and their diving experience, including whether they have suffered a caustic cocktail event and how it was treated. HOW THE STUDY WORKS Certified rebreather divers aged 18 years or older at the time of completing the survey are invited to participate. -
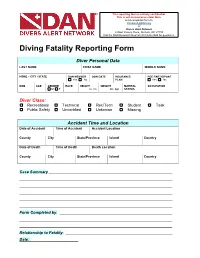
Diving Fatality Reporting Form
This reporting form is entirely confidential. This is not an insurance claim form. send completed form to: [email protected] or Divers Alert Network 6 West Colony Place, Durham, NC 27705 Call the DAN Research Dept at (919) 684-2948 for questions. Diving Fatality Reporting Form Diver Personal Data LAST NAME FIRST NAME MIDDLE NAME HOME – CITY / STATE DAN MEMBER JOIN DATE INSURANCE PDE PARTICIPANT Yes No PLAN Yes No DOB AGE GENDER RACE HEIGHT WEIGHT MARITAL OCCUPATION M F in cm lbs kgs STATUS Diver Class: Recreational Technical Rec/Tech Student Task Public Safety Uncertified Unknown Missing Accident Time and Location Date of Accident Time of Accident Accident Location County City State/Province Island Country Date of Death Time of Death Death Location County City State/Province Island Country Case Summary Form Completed by: Relationship to Fatality: Date: Name: Case #: Diver Experience CERTIFIED DIVER YEAR of INITIAL CERTIFYING AGENCY(s) Yes No CERTIFICATION # DIVES in LAST 12 MONTHS # DIVES in LAST 5 YEARS LAST DIVE PRECEDING ACCIDENT Days Months Years CERTIFICATION LEVEL Student Rescue Technical Military Basic/Open Water Master/Asst. Instructor Commercial None Advanced/Specialty Instructor and Above Scientific Other: GENERAL EXPERIENCE LEVEL Uncertified Inexperienced (6-20) Advanced (41-60) Novice (0-5 dives) Intermediate (21-40) Experienced (61+ dives) Diver Health PREVIOUS DIVE ACCIDENT If yes, what year SMOKE CIGARETTES # packs / week # years smoking Yes No Yes No Past PREVIOUS CONDITIONS CURRENT CONDITIONS CURRENT MEDICATIONS MEDICATION -

Mlml Scuba Diving Injury Protocol
MLML SCUBA DIVING INJURY PROTOCOL 1. Protect yourself and victim from further injury. 2. Assess victim, follow EMERGENCY FLOWCHART- next page 3. Contact EMS, and DAN for diving emergencies, Coast Guard if offshore (VHF 16). 4. Administer CPR/First Aid and Oxygen as needed, begin transport unless EMS recommends otherwise If victim is a member of DAN and you are more than 50 miles from campus, you can call 1-800-DAN-EVAC You can call 911 and request an ambulance You can use a private or university vehicle 5. Check and monitor victim's dive buddy for any signs or symptoms of DCI. Administer CPR/First Aid, Oxygen and treat for shock as needed. 6. If victim is unstable, check and record vital signs every 5 min during transport/while awaiting care. Check: pulse/min, blood pressure, respirations/min If stable, check and record every 15 minutes 7. Begin filling out PATIENT INFORMATION sheet, to give to EMS. 8. If conscious, perform FIELD NEUROLOGICAL EXAMINATION, record results 9. Contact Diving Safety Officer (831-771-4440 or 831-588-5591-cell), Supervisor/PI or member of Diving Emergency Personel as soon as is practical. See EMERGENCY TELEPHONE NUMBERS sheet. 10. Retain victim's diving equipment: Leave gear assembled, turn off air (count number of turns it takes to close valve), and rinse with fresh water (do not exhaust air from reg) 11. Gather dive history and other important information, fill out PATIENT INFO sheet: Take note of any dive data from a computer, depth gauge, timing device, SPG. Get the names, phone numbers and addresses of any witnesses. -

Watriama and Co Further Pacific Islands Portraits
Watriama and Co Further Pacific Islands Portraits Hugh Laracy Watriama and Co Further Pacific Islands Portraits Hugh Laracy Published by ANU E Press The Australian National University Canberra ACT 0200, Australia Email: [email protected] This title is also available online at http://epress.anu.edu.au National Library of Australia Cataloguing-in-Publication entry Author: Laracy, Hugh, author. Title: Watriama and Co : further Pacific Islands portraits / Hugh Laracy. ISBN: 9781921666322 (paperback) 9781921666339 (ebook) Subjects: Watriama, William Jacob, 1880?-1925. Islands of the Pacific--History. Dewey Number: 995.7 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying or otherwise, without the prior permission of the publisher. Cover design and layout by ANU E Press Printed by Griffin Press This edition © 2013 ANU E Press Contents Preface . ix 1 . Pierre Chanel of Futuna (1803–1841): The making of a saint . 1 2 . The Sinclairs Of Pigeon Bay, or ‘The Prehistory of the Robinsons of Ni’ihau’: An essay in historiography, or ‘tales their mother told them’ . 33 3 . Insular Eminence: Cardinal Moran (1830–1911) and the Pacific islands . 53 4 . Constance Frederica Gordon-Cumming (1837–1924): Traveller, author, painter . 69 5 . Niels Peter Sorensen (1848–1935): The story of a criminal adventurer . 93 6 . John Strasburg (1856–1924): A plain sailor . 111 7 . Ernest Frederick Hughes Allen (1867–1924): South Seas trader . 127 8 . Beatrice Grimshaw (1870–1953): Pride and prejudice in Papua . 141 9 . W .J . Watriama (c . 1880–1925): Pretender and patriot, (or ‘a blackman’s defence of White Australia’) . -

The Return of the Lama
Historical Diver, Volume 9, Issue 1 [Number 26], 2001 Item Type monograph Publisher Historical Diving Society U.S.A. Download date 09/10/2021 02:39:45 Link to Item http://hdl.handle.net/1834/30868 The Official Publication of The Historical Diving Societies of South East Asia & Pacific, Canada, Germany, Mexico and the U.S.A. Volume 9 Issue 1 Winter 2001 The Return of the Lama • Hugh Bradner's Wet Suit • Kenny Knott • Lowell Thomas Awards • • Antibes Diving History Seminar • Divair Regulator • E.R. Cross Files • • Anderson's Tales • ADCI, NOGI and DEMA Awards • Bud Swain • HISTORICAL DIVING SOCIETY USA A PUBLIC BENEFIT NONPROFIT CORPORATION 340 S KELLOGG AVE STE E, GOLETACA 93117, U.S.A. PHONE: 805-692-0072 FAX: 805-692-0042 e-mail: [email protected] or HTTP:I/www.hds.org/ ADVISORY BOARD FOUNDING BENEFACTORS Dr. Sylvia Earle Prof. Hans Hass Art Bachrach, Ph.D. Leslie Leaney Dr. Peter B. Bennett Lotte Hass Antonio Badias-Alonso Robert & Caroline Leaney Dick Bonin Dick Long Roger Bankston Andy Lentz Ernest H. Brooks II J. Thomas Millington, M.D. Ernie Brooks II A.L. "Scrap" Lundy Scott Carpenter Bob & Bill Meistrell Ken & Susan Brown Jim Mabry Wayne Brusate Andrew R. Mrozinski Jean-Michel Cousteau Bev Morgan P.K. Chandran Dr. Phil Nuytten E.R. Cross (1913-2000) Phil Nuytten Steve Chaparro Ronald E. Owen Henri Delauze Sir John Rawlins John Rice Churchill Torrance Parker Andre Galerne Andreas B. Rechnitzer, Ph.D. Raymond I. Dawson, Jr. Alese & Morton Pechter Lad Handelman Robert Stenuit Jesse & Brenda Dean Bob Ratcliffe Les Ashton Smith Diving Systems International Lee Selisky Skip & Jane Dunham Robert D. -

The Scuba Sports Club of Westchester, New York Our 44Th Year Serving the Local and Northeast Dive Community !
The Scuba Sports Club of Westchester, New York Our 44th year serving the local and northeast dive community ! The Scuba Sport Club’s WINTER 2018 Newsletter The Anchor Line Gary Lehman, Newsletter Editor Denise Blais, President Welcome to the WINTER 2018 issue of The Scuba Sports Club Sea Swells! Hi Everyone, We invite all members of the diving com- munity to contribute; please contact Gary at [email protected] with your Thank you all for a very successful articles and photos! Our Club Newsletter year! The board works hard to put includes features about our Club’s diving together activities that everyone will and social calendar; our diving adven- like participating in. We hope you join tures, social/educational events, occa- us again next year for a year filled with fun, education- sional equipment and health issue discussions, and pro- al and dive trip related activities. files on some of the more colorful and intrepid characters in our local diving community (of which there are many), Having members that are actively involved throughout and features of interest in the broader dive community. the year makes it that much more fun for everyone! We had a year to remember in 2018! Trips to San Salva- It’s been great meeting new members and sharing fun dor, Ustica (Sicily), Tubbataha (Philippines), our annual experiences throughout the year! Gloucester MA. Seal Dive, Grenada, our monthly dive safety briefings, Key Largo, Bonaire-and even a TSSC We hope you take some time as the year comes to a trek to Mt. Everest Base Camp to fight cancer! Can we top close to spend time with your family and friends relax- all THAT in 2019?! YOU BET !!! ing and enjoying the holiday season! It’s a great time to reflect the past year and recharge for the upcoming In this issue we will read about our 2018 Diver of the Year, year. -

Hazardous Marine Life
DIVERS ALERT NETWORK HAZARDOUS MARINE LIFE HEALTH & DIVING REFERENCE SERIES HAZARDOUS MARINE LIFE FOREWARD DAN’s Health & Diving Resource Series is a comprehensive collection of online and printed resources developed from years of DAN- supported research and insights gained from assisting thousands of members through dive and medical emergencies. These materials provide valuable information on topics critical to diver health and safety, as well as common issues encountered by new and experienced divers. As your dive safety association, it is our duty to provide the diving community with these vital education and reference tools. The series offers greater insight into topics such as ears and equalization, cardiovascular health, decompression sickness, hazardous marine injuries, and much more. Through information and education, we hope to enhance diver safety and incident prevention. Bill Ziefle DAN President & CEO CREDITS Managing Editor: Petar Denoble, MD, DSc Editor: Matias Nochetto, MD ISBN: 978-1-941027-31-8 TABLE OF CONTENTS CHAPTER 1: ENVENOMATIONS 4 Fire Coral 5 Portuguese Man-of-War 6 Lionfish 8 Blue-Ringed Octopus 10 Box Jellyfish 12 Cone Snails 15 CHAPTER 2: TRAUMATIC INJURIES AND COMPLICATIONS 16 Skin Abrasions 17 Stingrays 18 Sea Urchins 20 CHAPTER 3: SEAFOOD POISONINGS 23 Ciguatera 24 Scombroid Fish Poisoning 26 Red Tide & Shellfish Poisonings 28 CHAPTER 4: APPENDIX 31 Thermolysis 32 Antivenoms 33 Pressure Immobilization Technique 34 Hazardous Marine Life 3 1 ENVENOMATIONS “ “ Toxicity is in the dose. An envenomation is the process by which a venom or toxin is injected into another being via a bite, puncture or sting. Envenomation is always due to direct contact with an animal (or parts of it like drifting jellyfish tentacles). -

Stages 2 and 3 Public Information Package Public Comment
Stages 2 and 3 Public Information Package Cover image: Concept design for a sculpture of a scientist and a clam by Jason deCaires Taylor Public Comment The Museum of Underwater Art seeks public comment on proposed Stages 2 Palm Island and 3 Magnetic Island (Yunbenun). 10 May 2021 1 All comments and submissions to: Great Barrier Reef Marine Park Authority Environmental Assessment and Protection Unit PO Box 1379 Townsville QLD 4810 Email: [email protected] Website: www.gbrmpa.gov.au/about-us/consultation All comments must be provided to the address above to be considered in the assessment. The applicant is not obliged to forward any comments to the Managing Agency that have been made directly to the applicant. We now seek any public comment under Section 93 of the Great Barrier Reef Marine Park Regulations 2019 (Cth) and section 15 of the Marine Parks Regulation 2017 (Qld). Public submissions will be considered by the Great Barrier Reef Marine Park Authority and Department of Environment and Science (the Managing Agencies) in making a decision on this permit application. Comments will not be regarded as confidential unless confidentiality is specifically requested. Due consideration will be given to public comments before the Managing Agencies make any decisions in relation to the proposed use. The applicant may be provided with a copy of, or summary of, the comments received. All questions and further information to: Museum of Underwater Art Ltd c/- PvW Partners, 52 Walker St, Townsville QLD 4810 Email: [email protected] -

Balikesir-Ili-Profesyonel-Dalis-Merkezi-Yatirimi-On-Fizibilite-Raporu2020.Pdf
1 GÜNEY MARMARA KALKINMA AJANSI 2 RAPORUN KAPSAMI Bu ön fizibilite raporu, profesyonel ve rekreasyonel dalışın geliştirilmesi amacıyla Balıkesir ilinde dalış merkezi kurulmasının uygunluğunu tespit etmek, yatırımcılarda yatırım fikri oluşturmak ve detaylı fizibilite çalışmalarına altlık oluşturmak üzere Sanayi ve Teknoloji Bakanlığı koordinasyonunda faaliyet gösteren Güney Marmara Kalkınma Ajansı tarafından hazırlanmıştır. HAKLAR BEYANI Bu rapor, yalnızca ilgililere genel rehberlik etmesi amacıyla hazırlanmıştır. Raporda yer alan bilgi ve analizler raporun hazırlandığı zaman diliminde doğru ve güvenilir olduğuna inanılan kaynaklar ve bilgiler kullanılarak, yatırımcıları yönlendirme ve bilgilendirme amaçlı olarak yazılmıştır. Rapordaki bilgilerin değerlendirilmesi ve kullanılması sorumluluğu, doğrudan veya dolaylı olarak, bu rapora dayanarak yatırım kararı veren ya da finansman sağlayan şahıs ve kurumlara aittir. Bu rapordaki bilgilere dayanarak bir eylemde bulunan, eylemde bulunmayan veya karar alan kimselere karşı Sanayi ve Teknoloji Bakanlığı ile Güney Marmara Kalkınma Ajansı sorumlu tutulamaz. Bu raporun tüm hakları Güney Marmara Kalkınma Ajansına aittir. Raporda yer alan görseller ile bilgiler telif hakkına tabi olabileceğinden, her ne koşulda olursa olsun, bu rapor hizmet gördüğü çerçevenin dışında kullanılamaz. Bu nedenle; Güney Marmara Kalkınma Ajansı’nın yazılı onayı olmadan raporun içeriği kısmen veya tamamen kopyalanamaz, elektronik, mekanik veya benzeri bir araçla herhangi bir şekilde basılamaz, çoğaltılamaz, fotokopi veya -

2019 June;49(2)
Diving and Hyperbaric Medicine The Journal of the South Pacific Underwater Medicine Society and the European Underwater and Baromedical Society© Volume 49 No. 2 June 2019 Bullous disease and cerebral arterial gas embolism Does closing a PFO reduce the risk of DCS? A left ventricular assist device in the hyperbaric chamber The impact of health on professional diver attrition Serum tau as a marker of decompression stress Are hypoxia experiences for rebreather divers valuable? Nitrox vs air narcosis measured by critical flicker fusion frequency The effect of medications in diving E-ISSN 2209-1491 ABN 29 299 823 713 CONTENTS Diving and Hyperbaric Medicine Volume 49 No.2 June 2019 Editorials Obituary 77 Risk mitigation in divers with persistent foramen ovale 144 Dr John Knight FANZCA, Dip Peter Wilmshurst DHM, Captain RANR 78 The Editor's offering Original articles SPUMS notices and news 80 The effectiveness of risk mitigation interventions in divers 146 SPUMS Presidents message with persistent (patent) foramen ovale David Smart George Anderson, Douglas Ebersole, Derek Covington, Petar J Denoble 146 ANZHMG Report 88 Serum tau concentration after diving – an observational pilot 147 SPUMS 49th Annual Scientific study Meeting 2020 Anders Rosén, Nicklas Oscarsson, Andreas Kvarnström, Mikael Gennser, Göran Sandström, Kaj Blennow, Helen Seeman-Lodding, Henrik 147 Divers Emergency Service/DAN Zetterberg AP Foundation Telemedicine Scholarship 2019 96 A survey of scuba diving-related injuries and outcomes among French recreational divers 148 Australian