Diving Fatality Reporting Form
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ecological and Socio-Economic Impacts of Dive
ECOLOGICAL AND SOCIO-ECONOMIC IMPACTS OF DIVE AND SNORKEL TOURISM IN ST. LUCIA, WEST INDIES Nola H. L. Barker Thesis submittedfor the Degree of Doctor of Philosophy in Environmental Science Environment Department University of York August 2003 Abstract Coral reefsprovide many servicesand are a valuableresource, particularly for tourism, yet they are suffering significant degradationand pollution worldwide. To managereef tourism effectively a greaterunderstanding is neededof reef ecological processesand the impactsthat tourist activities haveon them. This study explores the impact of divers and snorkelerson the reefs of St. Lucia, West Indies, and how the reef environmentaffects tourists' perceptionsand experiencesof them. Observationsof divers and snorkelersrevealed that their impact on the reefs followed certainpatterns and could be predictedfrom individuals', site and dive characteristics.Camera use, night diving and shorediving were correlatedwith higher levels of diver damage.Briefings by dive leadersalone did not reducetourist contactswith the reef but interventiondid. Interviewswith tourists revealedthat many choseto visit St. Lucia becauseof its marineprotected area. Certain site attributes,especially marine life, affectedtourists' experiencesand overall enjoyment of reefs.Tourists were not alwaysable to correctly ascertainabundance of marine life or sedimentpollution but they were sensitiveto, and disliked seeingdamaged coral, poor underwatervisibility, garbageand other tourists damagingthe reef. Some tourists found sitesto be -

3. Technical Divemaster
TDI Standards and Procedures Part 3: TDI Leadership Standards 3. Technical Divemaster 3.1 Introduction This program is designed to develop the skills and knowledge necessary for an individual to lead certified technical divers in the open water environment. 3.2 Qualifications of Graduates Upon successful completion of this course, graduates may: 1. Assist an active TDI Instructor during approved diving courses provided the activities are similar to the graduate’s prior training 2. Supervise and conduct dives for certified technical divers provided the activities are similar to the graduate’s prior training 3. This program does not cover overhead environment with the exception of advanced wreck 3.3 Who May Teach 1. Any active TDI Instructor may teach this program 3.4 Student to Instructor Ratio Academic 1. Unlimited, so long as adequate facility, supplies and time are provided to ensure comprehensive and complete training of subject matter Confined Water (swimming pool-like conditions) 1. N/A Open Water (ocean, lake, quarry, spring, river or estuary) 1. A maximum of 4 students per instructor; it is the instructor’s discretion to reduce this number as conditions dictate Version 0221 33 TDI Standards and Procedures Part 3: TDI Leadership Standards 3.5 Student Prerequisites 1. Minimum age 18 2. Certified as an SDI Divemaster (equivalent ratings from other agencies are not accepted for this TDI Divemaster prerequisite) Must have all current SDI Divemaster materials 3. Provide copies of current CPR and first aid training 4. Have a current medical examination 5. Provide proof of 50 logged dives 6. Certified as a technical diver 3.6 Course Structure and Duration Open Water Execution 1. -

Love the Oceans Dive Policy Standards and Procedures
LOVE THE OCEANS DIVE POLICY STANDARDS AND PROCEDURES CONTENTS 1. Introduction 1 1.1 Definition of a dive 1 2. Love The Oceans Dive Standards 1 2.1 Maximum bottom time 1 2.2 Maximum depth 2 2.3 Air requirements 2 2.4 Safety stops 2 2.5 Surface interval 2 2.6 Repetitive diving 2 2.7 Flying after diving 3 2.8 Over-profiling 3 2.9 Supervision 3 2.10 PADI training courses 3 2.11 All course dives and snorkels 4 2.12 All non-course and non-training dives and snorkels 4 3. Love The Oceans Dive Procedures 4 3.1 General dive and boat procedures 5 3.2 Emergency procedures 5 3.3 Missing diver procedures 6 3.4 Injured diver procedures 6 3.5 Boat recall procedures 6 4. Dive equipment requirements 6 4.1 PADI dive training 6 4.2 Certified divers/science staff volunteers 6 5. Required safety equipment 7 6. Definitions of Roles and Responsibilities 7 6.1 Dive Operations Manager 7 6.2 Dive instructors 8 6.3 Divemasters and Dive leaders 8 6.4 Certified divers and science staff volunteers 8 7. Insurance 9 8. Night dive specific standards and protocols 9 9. Environmental Awareness 10 9.1 Code of Conduct for Whale Shark Encounters 10 9.2 Code of Conduct for Manta Ray Encounters 10 9.3 Code of Conduct for Humpback Whale Encounters 11 9.4 General Code of Conduct for Diving 12 These dive policy standards and procedures were last reviewed on 21st February 2019 1 1. -
Darling Marine Center Local Shore Diving Guide
Darling Marine Center Local Shore Diving Guide University of Maine Scientific Diving Program Table of Contents Recommended Equipment List……………………………………………………………..2 Local Information…………………………………………………………………………...3 Recompression Chambers…………………………………………………………………..3 General Emergency Action Plan…………………………………………………………….3-4 Documentation……………………………………………………………………………….4 Dive Sites DMC Pier……………………………………………………………………………5-6 Kresge Point………………………………………………………………………….7-8 Lowes Cove Mooring Field…………………………………………………………..9-10 Pemaquid Point……………………………………………………………………….11-12 Rachel Carson Preserve………………………………………………………………13-15 Sand Cove…………………………………………………………………………….16-17 Thread of life…………………………………………………………………………18-19 Appendix………………………………………………………………………………………20 1 Recommended Equipment List • Dive flag • DAN oxygen and first aid kit • Spare tank • Extra weights • Save-a-dive kit • Dive slate/underwater paper (recording purposes) Recommended Personal Equipment • Exposure suit- minimum7mm wetsuit o Booties o Gloves o Hood o Wool socks • Fins • BCD • Mask, Snorkel • Weights • Surface marker buoy • Dive watch • Dive computer • Knife/cutting tool 2 Local Information: Fire, Medical, Police 911 Emergency Dispatch Lincoln County Emergency (207)563-3200 Center Nearest Hospital Lincoln Health-Miles (207)563-1234 Campus USCG Boothbay (207)633-2661 Divers Alert Network Emergency hotline 1-919-684-9111 Medical information 1-919-684-2948 Diving Safety Officer Christopher Rigaud (207)563-8273 Recompression Chambers: In the event of a diving accident, call 911 and facilitate transport of victim to a hospital or medical facility. The medical staff will determine whether hyperbaric treatment is needed. St. Mary’s Regional Lewiston, ME (207)777-8331 Will NOT accept Medical Center divers after 4:30pm St. Joseph’s Hospital Bangor, ME (207)262-1550 Typically, available after hours Wound and Beverly, MA (978)921-1210 Hyperbaric Medicine Basic Emergency Information: See Appendix for the approved Emergency Action Plan by the UMaine DCB. -

Spearfishing in Great Barrier Reef Marine Park
· Great • Reef Marine Park Authoiity LAw Bu • Issue Number 18 SPEARFISHING IN GREAT BARRIER REEF MARINE PARK Where am I allowed to spearfish? Seasonal Closure Areas You may spearfish in all gerieral use zones in the Seasonal Closure Areas are areas closed to all access Marine Park, and in all non-zoned sections of the during the breeding or nesting periods of birds or Marine Park. You should note that some Queensland other marine life. The closure of these areas is waters are closed to spearfishing - there are details advertised. of those areas in the Queensland Harbours ahd What equipment can I use? Marine Tide Tables. You may only spearfish using a snorkel and a hand Where am I NOT allowed to spearfish? spear or speargun. You may not use any other You may not spearfish in Marine National Park 'A', underwater breathing equipment (such as scuba or Marine National Park Buffer and Marine National hookah) and you may only use a powerhead for Park 'B' Zones, nor in Scientific Research or protection against a shark attack. Preservation Zones. You also may not spearfish in areas where periodic restrictions are in operation. Can I sell fish I spear? These areas may be Replenishment Areas, Reef Spearfishing for the purpose of sale or trade is not Appreciation Areas, Reef Research Areas or Seasonal allowed in the Marine Park, with one exception, in Closure Areas. the Far Northern Section of the Marine Park it is permitted to spear crayfish for purposes of sale or Replenishment Areas trade (you can also use scuba or hookah in this A Replenishment Area is an area closed for a circumstance - but only for crayfish). -

California Regulatory Notice Register 2008, Volume No. 26-Z
ARNOLD SCHWARZENEGGER, GOVERNOR OFFICE OF ADMINISTRATIVE LAW REGISTER 2008, NO. 27–Z PUBLISHED WEEKLY BY THE OFFICE OF ADMINISTRATIVE LAW JULY 4, 2008 PROPOSED ACTION ON REGULATIONS TITLE 2. FAIR POLITICAL PRACTICES COMMISSION Conflict of Interest Code — Notice File No. Z2008–0618–01 . 1123 STATE AGENCY: Office of Information Security and Privacy Protection MULTI COUNTY: Desert Community College District Lowell Joint School District TITLE 2. FAIR POLITICAL PRACTICES COMMISSION Conflict of Interest Code — Notice File No. Z2008–0623–02 . 1124 Tulare County Office of Education TITLE 3. DEPARTMENT OF FOOD AND AGRICULTURE Light Brown Apple Moth Interior Quarantine — Notice File No. Z2008–0623–04 . 1125 TITLE 3. DEPARTMENT OF PESTICIDE REGULATION Notification & Application—Specific Information — Notice File No. Z2008–0624–05 . 1127 TITLE 8. OCCUPATIONAL SAFETY AND HEALTH STANDARDS BOARD General Industry Safety Orders — Aerosol Transmissible Diseases — Zoonotics — Notice File No. Z2008–0624–09 . 1129 TITLE 9. DEPARTMENT OF REHABILITATION Accreditation of Community Rehabilitation Programs — Notice File No. Z2008–0623–01 . 1151 TITLE 11. PEACE OFFICER STANDARDS AND TRAINING Child Safety When a Caretaker Parent or Guardian is Arrested — Notice File No. Z2008–0624–11 . 1155 TITLE 11. PEACE OFFICER STANDARDS AND TRAINING Training and Testing Specifications — DA Invest — Notice File No. Z2008–0624–10 . 1156 TITLE 15. DEPARTMENT OF CORRECTIONS AND REHABILITATION Division of Audit Parole Operations Revisions — Notice File No. Z2008–0619–01 . 1158 (Continued on next page) Time- Dated Material GENERAL PUBLIC INTEREST DEPARTMENT OF FAIR EMPLOYMENT AND HOUSING List of Prospective Contractors Ineligible to Enter Into State Contracts . 1161 DEPARTMENT OF FISH AND GAME CESA Consistency Determination Request for San Pablo Dam Seismic Upgrade Project, Contra Costa County . -

Dive Master Course Outline
Dive Master Course Outline www.ScubaNashville.com Congratulations on your decision to become a PADI Divemaster. Of all the certifying agencies PADI is the largest, offers you the most support and is the most widely recognized. Most dive shops and resorts require their dive industry employees to be a PADI Professional. The course consists of three modules, diving skills assessment, academic learning, and internship. You must complete all three modules to a reasonable level of proficiency before you may become a Divemaster. Module One assesses, and if necessary, remediates the candidates’ general diving skill level including peak performance bouncy. You must demonstrate adequate diving skills before you may proceed to module three. Module Two academic is designed to increase the candidate's diving theory knowledge to a higher level through the use of independent study and written exams. You will take eight required written exams, covering the following topics: Divemaster Conducted Programs, Supervising Certified Divers, Assisting with Student Divers in Training, Physics, Physiology, Equipment, Skills and Environment, The Recreational Dive Planner. The first three exams must be successfully completed before starting your internship. The remaining five exams may be taken anytime. The information for these exams may be found through self-guided study in the current Divemaster Manual, The Encyclopedia of Recreational Diving, and the Diving Knowledge Workbook. The Divemaster Manual has Knowledge Reviews that must be completed and turned in as well. All exams are 20 questions and have a minimum passing score of 75%. Module Three, the internship is most important and involves the Divemaster candidate in actual training and supervisory situations under the direction of a PADI Instructor. -

SDI Divemaster Course Checklist
SDI Standards and Procedures Part 4: SDI Leadership Standards 3. Divemaster 3.1 Introduction This program is designed to develop the skills and knowledge necessary for an individual to lead certified divers in the open water environment. 3.2 Qualifications of Graduates Upon successful completion of this course, graduates may: 1. Assist an active SDI Instructor during approved diving courses provided the activities are similar to the graduate’s prior training 2. Supervise and conduct dives for certified divers and any specialized scuba diving activities that they have been trained in, provided the activities are similar to the graduate’s prior training 3. Plan and execute emergency procedures appropriate for the diving environment and activities 3.3 Who May Teach An active SDI Instructor 3.4 Student to Instructor Ratio Academic 1. Unlimited, so long as adequate facility, supplies and time are provided to ensure comprehensive and complete training of subject matter Confined Water (swimming pool-like conditions) 1. A maximum of 8 students per instructor Open Water (ocean, lake, quarry, spring, river or estuary) 1. A maximum of 8 students per instructor are allowed; it is the instructor’s discretion to reduce this number as conditions dictate 3.5 Student Prerequisites 1. Minimum age 18 2. Certified SDI Advanced Adventure Diver or equivalent; advanced certification must include verifiable experience in deep, navigation, night, and limited visibility specialties 18 Version 0221 SDI Standards and Procedures Part 4: SDI Leadership Standards 3. Certified SDI Rescue Diver or equivalent 4. Provide proof of current CPR, first aid and oxygen provider*, where local law permits 5. -

SPEARFISHING Valid: Sept 1 – Aug 31 Resident – Non-Resident
Section III – S . 1 SPEARFISHING Valid: Sept 1 – Aug 31 Resident – Non-Resident Alabama Game, Fish and Wildlife Law; Article 5; beginning with 9-11-170 PRIVILEGE: • Allows person completely submerged, to spear commercial or non-game fish in freshwater or saltwater state. NOTE: • Possession of speargun or spearing device in a boat or on the bank of a body of water is prima facie evidence of its use. • Appropriate freshwater and/or saltwater fishing license is also required for spearfishing in freshwater. • License not required to frog gig. COST: • Resident Annual ..................... $6.00 • Non-Resident Annual .............. $8.50 • Non-Resident 7-Day Trip ........ $3.50 HOW TO PURCHASE YOUR LICENSE: • Visit www.outdooralabama.com/alabama-license-information • Call 1-888-848-6887 (Immediate confirmation code is given. Processing fees apply) • Visit the Marine Resources Office o 999 Commerce Street, Gulf Shores, AL 36547 o 2 North Iberville, Dauphin Island, AL 36542 • Visit the Montgomery Office (64 North Union St., Ste. 567, Montgomery, AL 36104) o 64 N Union Street, Ste. 567, Montgomery, AL • Mail a completed application (download at www.outdooralabama.com/licenses) to Dept. of Conservation, Wildlife & Freshwater Fisheries, Attn: License Sales: o PO Box 301456, Montgomery, AL 36130-1456 o 64 N Union St., Ste. 567, Montgomery, AL 36104 (overnight/express) Wildlife & Freshwater Fisheries Division – License Manual Revised: 09/17 Revised: 09/17 Section III – S. 2 DEPARTMENT OF CONSERVATION AND NATURAL RESOURCES WILDLIFE AND FRESHWATER FISHERIES DIVISION SPEARFISHING LICENSE Valid: Sept 1 – Aug 31 Resident LICENSE HOLDER: all information is required. PRINT OR TYPE ONLY INCOMPLETE APPLICATIONS WILL BE RETURNED Name: ____________________________________________________________ Sex: Male Female (1) Social Security #: - - Driver’s License # __________________ Wt. -

A Quantitative Comparison of Recreational Spearwshing and Linewshing on the Great Barrier Reef: Implications for Management of Multi-Sector Coral Reef Wsheries
Coral Reefs (2008) 27:85–95 DOI 10.1007/s00338-007-0293-z REPORT A quantitative comparison of recreational spearWshing and lineWshing on the Great Barrier Reef: implications for management of multi-sector coral reef Wsheries A. J. Frisch · R. Baker · J-P. A. Hobbs · L. Nankervis Received: 3 May 2007 / Accepted: 6 August 2007 / Published online: 25 August 2007 © Springer-Verlag 2007 Abstract This study compared the catch composition, equitably across both Wshing sectors. A management strategy catch per unit eVort, and incidental impacts of spearWshers of this type will simplify enforcement of Wsheries regulations and lineWshers engaged in a structured Wshing program and avoid discrimination of particular Wshers in local whereby Wshing eVort was standardized across time, space communities where both Wshing methods are socially or and skill level. It was found that (1) the catch composition culturally important. of both groups of Wshers overlapped considerably, (2) the numbers of target Wsh caught by spearWshers (156) and Keywords SpearWshing · LineWshing · Catch per unit lineWshers (168) were not signiWcantly diVerent, (3) the eVort · Selectivity · Coral trout · Bycatch mean size of target Wsh caught by spearWshers (1.95 § 0.1 kg, §SE) was signiWcantly larger than the mean size of target Wsh caught by lineWshers (1.27 § 0.06 kg), and (4) spear- Introduction Wshers retained 43% more biomass of target species than did lineWshers (304 versus 213 kg, respectively). However, OverWshing is deemed to be one of the greatest threats to lineWshers used »1 kg of bait for every 3 kg of target Wsh the future of coral reefs (Jackson et al. -

Standards, Criteria and Guidance Document F Recreational Scuba Diving Operations
Standards, criteria and guidance document F Recreational Scuba Diving Operations 1.0 Introduction The aim of this document is to establish service standards and other requirements for the running of a recreational scuba diving operation or dive centre. It also aims to ensure that the highest safety operational standards are maintained by all recreational scuba diving service providers. The primary purpose of these standards is to ensure that the licensee and/or the operator and staff are sufficiently qualified and competent to provide diving services, and that the operation is supported by the required infrastructure, equipment and other provisions necessary. Licensees are obliged to comply with these standards and must be covered by sufficient third party liability insurance. Unlicensed recreational dive centres are prohibited from advertising any diving services. These standards shall apply to any licensed person offering recreational diving services to the public and any other person employed by such physical or legal person to carry out any of the services provided by the diving centre. The provision of recreational diving services is to be considered a tourism operation in terms of the Act and shall therefore be subject to the provisions of the Act and to any relevant standards made thereunder. 2.0 Interpretation 2.1 In these standards, unless the context otherwise requires: "the Act" means the Malta Travel and Tourism Services Act; Cap. 409. "the Authority" means the Malta Tourism Authority; "breathing gas" means a mixture of inert -
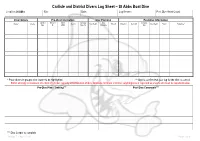
Carlisle and District Divers Log Sheet – St Abbs Boat Dive
Carlisle and District Divers Log Sheet – St Abbs Boat Dive Location: St Abbs Site: Date: Log Keeper: Post Dive Head Count: Diver Details Pre-Dive Information Dive Planning Post-Dive Information Cylinder Nitrox % Nitrox Aux Gas Max Aux Gas Name* Grade Gas In Max Depth Time In Duration Gas Out Max Depth Stops Signature** Size O2 MOD Size / In Duration Out * Place divers in groups; dive leader to be highlighted. ** Sign to confirm that your log for the dive is correct. BSAC strongly recommend one third of cylinder capacity at termination of dive. Absolute minimum is 40 bar; anything less is regarded as unsafe and must be reported below. Pre-Dive Plan / Training*** Post Dive Comments*** *** Dive Leader to complete Version 7 – April 2013 Page 1 of 4 Carlisle and District Divers Dive Specific Assessment – St Abbs Boat Dive Location: St Abbs Date: Dive Manager: Assistant Dive Manager: Location of Phones or Radios: UK Emergencies at Sea: First Aider / Oxygen Administrator: Deputy First Aider / Oxygen Administrator: Coastguard: VHF DSC / Channel 16 Lives in danger: Mayday, Mayday DCI: Pan, Pan Location of Nearest A&E Facility: UK Emergencies on Land: Location of First Aid and Oxygen Kits: Access to First Aid and Oxygen Kits: Berwick Infirmary, DCI: 07831 151523 Infirmary Square, Berwick-upon-Tweed, DCI Scotland: 0845 408 6008 Northumberland. TD15 1LT DCI: 999 / 112 (Coastguard) 0844 811 8111 Near Drowning: 999 / 112 (Ambulance) Approximately 13 miles Lost Diver: 999 / 112 (Police) Weather Forecast: Wind Direction / Speed: Air Temperature: Anticipated