Try Scuba & Try Scuba Diving
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ecological and Socio-Economic Impacts of Dive
ECOLOGICAL AND SOCIO-ECONOMIC IMPACTS OF DIVE AND SNORKEL TOURISM IN ST. LUCIA, WEST INDIES Nola H. L. Barker Thesis submittedfor the Degree of Doctor of Philosophy in Environmental Science Environment Department University of York August 2003 Abstract Coral reefsprovide many servicesand are a valuableresource, particularly for tourism, yet they are suffering significant degradationand pollution worldwide. To managereef tourism effectively a greaterunderstanding is neededof reef ecological processesand the impactsthat tourist activities haveon them. This study explores the impact of divers and snorkelerson the reefs of St. Lucia, West Indies, and how the reef environmentaffects tourists' perceptionsand experiencesof them. Observationsof divers and snorkelersrevealed that their impact on the reefs followed certainpatterns and could be predictedfrom individuals', site and dive characteristics.Camera use, night diving and shorediving were correlatedwith higher levels of diver damage.Briefings by dive leadersalone did not reducetourist contactswith the reef but interventiondid. Interviewswith tourists revealedthat many choseto visit St. Lucia becauseof its marineprotected area. Certain site attributes,especially marine life, affectedtourists' experiencesand overall enjoyment of reefs.Tourists were not alwaysable to correctly ascertainabundance of marine life or sedimentpollution but they were sensitiveto, and disliked seeingdamaged coral, poor underwatervisibility, garbageand other tourists damagingthe reef. Some tourists found sitesto be -

3. Technical Divemaster
TDI Standards and Procedures Part 3: TDI Leadership Standards 3. Technical Divemaster 3.1 Introduction This program is designed to develop the skills and knowledge necessary for an individual to lead certified technical divers in the open water environment. 3.2 Qualifications of Graduates Upon successful completion of this course, graduates may: 1. Assist an active TDI Instructor during approved diving courses provided the activities are similar to the graduate’s prior training 2. Supervise and conduct dives for certified technical divers provided the activities are similar to the graduate’s prior training 3. This program does not cover overhead environment with the exception of advanced wreck 3.3 Who May Teach 1. Any active TDI Instructor may teach this program 3.4 Student to Instructor Ratio Academic 1. Unlimited, so long as adequate facility, supplies and time are provided to ensure comprehensive and complete training of subject matter Confined Water (swimming pool-like conditions) 1. N/A Open Water (ocean, lake, quarry, spring, river or estuary) 1. A maximum of 4 students per instructor; it is the instructor’s discretion to reduce this number as conditions dictate Version 0221 33 TDI Standards and Procedures Part 3: TDI Leadership Standards 3.5 Student Prerequisites 1. Minimum age 18 2. Certified as an SDI Divemaster (equivalent ratings from other agencies are not accepted for this TDI Divemaster prerequisite) Must have all current SDI Divemaster materials 3. Provide copies of current CPR and first aid training 4. Have a current medical examination 5. Provide proof of 50 logged dives 6. Certified as a technical diver 3.6 Course Structure and Duration Open Water Execution 1. -

Love the Oceans Dive Policy Standards and Procedures
LOVE THE OCEANS DIVE POLICY STANDARDS AND PROCEDURES CONTENTS 1. Introduction 1 1.1 Definition of a dive 1 2. Love The Oceans Dive Standards 1 2.1 Maximum bottom time 1 2.2 Maximum depth 2 2.3 Air requirements 2 2.4 Safety stops 2 2.5 Surface interval 2 2.6 Repetitive diving 2 2.7 Flying after diving 3 2.8 Over-profiling 3 2.9 Supervision 3 2.10 PADI training courses 3 2.11 All course dives and snorkels 4 2.12 All non-course and non-training dives and snorkels 4 3. Love The Oceans Dive Procedures 4 3.1 General dive and boat procedures 5 3.2 Emergency procedures 5 3.3 Missing diver procedures 6 3.4 Injured diver procedures 6 3.5 Boat recall procedures 6 4. Dive equipment requirements 6 4.1 PADI dive training 6 4.2 Certified divers/science staff volunteers 6 5. Required safety equipment 7 6. Definitions of Roles and Responsibilities 7 6.1 Dive Operations Manager 7 6.2 Dive instructors 8 6.3 Divemasters and Dive leaders 8 6.4 Certified divers and science staff volunteers 8 7. Insurance 9 8. Night dive specific standards and protocols 9 9. Environmental Awareness 10 9.1 Code of Conduct for Whale Shark Encounters 10 9.2 Code of Conduct for Manta Ray Encounters 10 9.3 Code of Conduct for Humpback Whale Encounters 11 9.4 General Code of Conduct for Diving 12 These dive policy standards and procedures were last reviewed on 21st February 2019 1 1. -

Dive Master Course Outline
Dive Master Course Outline www.ScubaNashville.com Congratulations on your decision to become a PADI Divemaster. Of all the certifying agencies PADI is the largest, offers you the most support and is the most widely recognized. Most dive shops and resorts require their dive industry employees to be a PADI Professional. The course consists of three modules, diving skills assessment, academic learning, and internship. You must complete all three modules to a reasonable level of proficiency before you may become a Divemaster. Module One assesses, and if necessary, remediates the candidates’ general diving skill level including peak performance bouncy. You must demonstrate adequate diving skills before you may proceed to module three. Module Two academic is designed to increase the candidate's diving theory knowledge to a higher level through the use of independent study and written exams. You will take eight required written exams, covering the following topics: Divemaster Conducted Programs, Supervising Certified Divers, Assisting with Student Divers in Training, Physics, Physiology, Equipment, Skills and Environment, The Recreational Dive Planner. The first three exams must be successfully completed before starting your internship. The remaining five exams may be taken anytime. The information for these exams may be found through self-guided study in the current Divemaster Manual, The Encyclopedia of Recreational Diving, and the Diving Knowledge Workbook. The Divemaster Manual has Knowledge Reviews that must be completed and turned in as well. All exams are 20 questions and have a minimum passing score of 75%. Module Three, the internship is most important and involves the Divemaster candidate in actual training and supervisory situations under the direction of a PADI Instructor. -

SDI Divemaster Course Checklist
SDI Standards and Procedures Part 4: SDI Leadership Standards 3. Divemaster 3.1 Introduction This program is designed to develop the skills and knowledge necessary for an individual to lead certified divers in the open water environment. 3.2 Qualifications of Graduates Upon successful completion of this course, graduates may: 1. Assist an active SDI Instructor during approved diving courses provided the activities are similar to the graduate’s prior training 2. Supervise and conduct dives for certified divers and any specialized scuba diving activities that they have been trained in, provided the activities are similar to the graduate’s prior training 3. Plan and execute emergency procedures appropriate for the diving environment and activities 3.3 Who May Teach An active SDI Instructor 3.4 Student to Instructor Ratio Academic 1. Unlimited, so long as adequate facility, supplies and time are provided to ensure comprehensive and complete training of subject matter Confined Water (swimming pool-like conditions) 1. A maximum of 8 students per instructor Open Water (ocean, lake, quarry, spring, river or estuary) 1. A maximum of 8 students per instructor are allowed; it is the instructor’s discretion to reduce this number as conditions dictate 3.5 Student Prerequisites 1. Minimum age 18 2. Certified SDI Advanced Adventure Diver or equivalent; advanced certification must include verifiable experience in deep, navigation, night, and limited visibility specialties 18 Version 0221 SDI Standards and Procedures Part 4: SDI Leadership Standards 3. Certified SDI Rescue Diver or equivalent 4. Provide proof of current CPR, first aid and oxygen provider*, where local law permits 5. -

Standards, Criteria and Guidance Document F Recreational Scuba Diving Operations
Standards, criteria and guidance document F Recreational Scuba Diving Operations 1.0 Introduction The aim of this document is to establish service standards and other requirements for the running of a recreational scuba diving operation or dive centre. It also aims to ensure that the highest safety operational standards are maintained by all recreational scuba diving service providers. The primary purpose of these standards is to ensure that the licensee and/or the operator and staff are sufficiently qualified and competent to provide diving services, and that the operation is supported by the required infrastructure, equipment and other provisions necessary. Licensees are obliged to comply with these standards and must be covered by sufficient third party liability insurance. Unlicensed recreational dive centres are prohibited from advertising any diving services. These standards shall apply to any licensed person offering recreational diving services to the public and any other person employed by such physical or legal person to carry out any of the services provided by the diving centre. The provision of recreational diving services is to be considered a tourism operation in terms of the Act and shall therefore be subject to the provisions of the Act and to any relevant standards made thereunder. 2.0 Interpretation 2.1 In these standards, unless the context otherwise requires: "the Act" means the Malta Travel and Tourism Services Act; Cap. 409. "the Authority" means the Malta Tourism Authority; "breathing gas" means a mixture of inert -
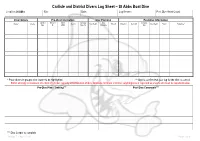
Carlisle and District Divers Log Sheet – St Abbs Boat Dive
Carlisle and District Divers Log Sheet – St Abbs Boat Dive Location: St Abbs Site: Date: Log Keeper: Post Dive Head Count: Diver Details Pre-Dive Information Dive Planning Post-Dive Information Cylinder Nitrox % Nitrox Aux Gas Max Aux Gas Name* Grade Gas In Max Depth Time In Duration Gas Out Max Depth Stops Signature** Size O2 MOD Size / In Duration Out * Place divers in groups; dive leader to be highlighted. ** Sign to confirm that your log for the dive is correct. BSAC strongly recommend one third of cylinder capacity at termination of dive. Absolute minimum is 40 bar; anything less is regarded as unsafe and must be reported below. Pre-Dive Plan / Training*** Post Dive Comments*** *** Dive Leader to complete Version 7 – April 2013 Page 1 of 4 Carlisle and District Divers Dive Specific Assessment – St Abbs Boat Dive Location: St Abbs Date: Dive Manager: Assistant Dive Manager: Location of Phones or Radios: UK Emergencies at Sea: First Aider / Oxygen Administrator: Deputy First Aider / Oxygen Administrator: Coastguard: VHF DSC / Channel 16 Lives in danger: Mayday, Mayday DCI: Pan, Pan Location of Nearest A&E Facility: UK Emergencies on Land: Location of First Aid and Oxygen Kits: Access to First Aid and Oxygen Kits: Berwick Infirmary, DCI: 07831 151523 Infirmary Square, Berwick-upon-Tweed, DCI Scotland: 0845 408 6008 Northumberland. TD15 1LT DCI: 999 / 112 (Coastguard) 0844 811 8111 Near Drowning: 999 / 112 (Ambulance) Approximately 13 miles Lost Diver: 999 / 112 (Police) Weather Forecast: Wind Direction / Speed: Air Temperature: Anticipated -

Summer | 2016 LUXURY Diving Holidays GROUP DIVING
Summer | 2016 LUXURY Diving Holidays GROUP DIVING Inspiration DUMAGUETE Dive Dispatch UP CLOSE in Socorro Ari Atoll Paradise Earlier this year, regular Dive Worldwide clients Cynthia & Simon returned to Vilamendhoo Island Resort in the Maldives and found that it more than matched up to the memories from their previous visit. he holiday was great. The flights, including the seaplane transfers, all went according to plan. TVilamendhoo is as wonderful as ever, truly a desert island. The resort staff are so friendly and helpful, they really do understand the meaning of customer service. It is amazing how some of them even remembered us, especially as it was two years ago when we were last there! Simon and I managed to each do 17 dives, and I achieved my 400 dive milestone. Simon is just a couple short of 800 dives. We went out twice on the all-day manta boat trip. On the first day we only saw two mantas very fleetingly over the two dives; so Simon persuaded me to go again the second week - and this time we were rewarded with lots of mantas on both dives. They really are awesome creatures, and we got really close at the end of the second dive when they swam around us as we did our five metre safety stop! We didn’t get to see a whale shark this time, but several smaller white- Ari Atoll Diving Experience tip and black-tip reef sharks, plus my favourite, turtles. We also saw Vilamendhoo Island Resort offers the perfect base to huge shoals of most of the other common reef fish. -

SCUBA DRILLS Snorkeling Gear Prep, Entry, Snorkel Clear, Kicks Gear Prep: Mask (Ant Fogged) –Fins, Gloves, Boots, Ready by Entry Point Access
(616) 364-5991 SCUBA DRILLS WWW.MOBYSDIVE.COM Snorkeling Gear Prep, Entry, Snorkel clear, Kicks Gear prep: Mask (ant fogged) –fins, gloves, boots, ready by entry point access. (it is crucial that the mask-fins-boots are properly designed and fitted before the aquatic session to prevent delays in training due to gear malfunction ) Equipment nicely assembled by entry point for easy donning and water access ENABLED EQUIPMENT NICELY ASSEMBLED – BUDDY CHECK – LOGBOOK CHECK – ENTRY – DRILL REVIEW Equipment Nicely Assembled: (Each Diver needs to develop the practice of properly assembling their scuba gear by themselves) Full tank secured until ready for gear assembly. Tank upright, BCD tank band straps are loosened as to allow easy placement of strap around the tank. NOTE: Hard pack BCD’s usually have ONE tank band, Soft pack BCD’s usually have TWO tank bands. Most bands have a buckle / cam strap and need to be weaved a particular way to stay secured. Ensure the BCD’s placement on the tank so the tank valve is level with where the diver’s neck will be and that the front part of the valve (where the air is released) is facing the back of the diver. Secure the strap or straps so they are tight enough to pick up the BCD and tank and not slip while shaking. Regulator placement: The First stage (dust cap removed) is placed over the tank valve so the intake of the 1st stage covers the o-ring on the tank valve, (o-ring should be in place – if not, lack of seal will cause air leak). -
Snorkel Diver, Try Freediving and Try Mermaid Participant Registration Form
Snorkel Diver, Try Freediving and Try Mermaid Participant Registration Form First Name Last Name Date of Birth (DD/MM/YY) Mailing Address Email Address Cell Phone Emergency Contact Name Relationship Email Address Cell Phone Privacy Policy This Privacy Policy explains why SSI Training Centers obtain your personal data for the purposes of conducting your training, issuing certifications, administration of your private information and any other necessary specifics regarding the performance of this agreement. By registering in MySSI, you are consenting to share your personal data: Name (First and Last), Address (Postbox), Postcode (Zip), City, State, Country, Email Address, Telephone Numbers (optional), Date of Birth, Photo, Language, Gender, SSI Master ID, Course Type, Course Progress and Certification Information (Name, SSI Training Center, Certifying Instructor, Year You Started Diving, Level of Experience, Number of Dives and Issue Date), plus your Training Center Affiliation. By giving your consent, SSI Training Centers may subsequently access your personal data described above in order to identify you, verify or confirm the status of your training and certifications and to offer you continued training and services based on your diving experience. For more information you may go to the SSI Privacy Policy at https://my.divessi.com/myssi_privacy. Download the free MySSI App, available for iOS or Android! SSI designed the MySSI App to be that “All-In-One Tool” for your diving experiences and to give you access to your Digital Learning Materials, Digital Logbook and Digital Recognition Cards, all in the palm of your hand. There are a variety of features like news, local events, training dates, fun 360º videos and even dive tables and hand signals to review before your next dive. -

Dive Leader Mock Exam Revision
DIVE LEADER MOCK EXAM REVISION – M1 This is a mock paper with model answers for the questions and some extension activities for those who want to practice further questions of each type. The focus of this paper is calculations for dive planning and some basic revision. You will need Pencil, Eraser & Calculator BSAC 88 Decompression Tables Levels 1-4 BSAC Nitrox tables Calculations In breathing gas calculations use 25 litres/minute for the normal breathing rate at the surface. For CNS% calculations use the Oxygen Toxicity Table on p23 of the BSAC Nitrox Tables. 80% CNS is the maximum allowed dose – UPTDs is 180 in a rolling 24-hour period 1. Using the following extract from a tide table, calculate the depth of water in meters at the nearest high water to noon, if the charted depth is 23.8m. All times are GMT: Add 1 hour for BST 31 March to 27 October Time m Jun 0440 1.3 4 1109 5.7 SA 1708 1.6 2333 6.1 A: 25.2, B: 29.9, C: 24.4, D: 29.5, E: 27.6 2. You are planning a dive on or around slack water at Holcombe head. Using chart and tidal diamond, what is the optimum time to dive this site on a neap tide and what direction will the current be flowing and what speed ? A: +1hr & 170 & 0.2kn, B: -4hr & 026 & 0.2kn, C: -4hr & 290 & 0.4kn, D: -6hr & 216 & 0.3kn, E: None are safe dives DIVE LEADER MOCK EXAM REVISION – M1 3. -

Pathways Program
Experience counts. Welcome to High Plains Scuba Center, Northern PATHWAYS Colorado's oldest and largest full-service scuba facility. Thank you for choosing us for your aquatic PROGRAM adventures. Everything you need. High Plains Scuba Center offers the finest in professional education, quality travel services, state of the art equipment, and an onsite heated pool. Whether you are just getting started or you’re an experienced diver, High Plains Scuba Center has what you need. Training. Learn scuba diving from our highly trained and experienced instructors. We conduct courses from entry level through all professional levels. Equipment. Our friendly and knowledgeable retail staff can counsel you in finding the equipment that’s best suited to you. And we stand behind what we sell. Service and Repair. Our service department has the expertise to keep your equipment working safely. Protect your investment with regular maintenance. High Plains Scuba Center 115 WEST HARVARD Travel. Rely on HPSC’s expertise in dive travel. We’ll help you find the right destination, FORT COLLINS, CO 80525 choose the accommodations that fit your interests, and put together a vacation package you’ll love. (970) 493-8562 E-MAIL: [email protected] READY? Let us help you get started on your www.highplainsscuba.com lifetime of SCUBA ADVENTURE!!!! FAX: (970) 493-8588 OPEN WATER DIVER PATH TO MASTER DIVER PATH TO PROFESSIONAL The Open Water Diver rating is the entry point to Open Water Diver diving most of the world with 4 certification dives. (Minimum of 4 logged dives) OR ADVANCED ADVENTURER DIVE GUIDE The Advanced Adventurer program is designed to be a Advanced Adventurer The SSI Dive Guide rating is the transition point from a sampler of 5 specialty dives to explore specialty opportuni- recreational diver to becoming a dive leader.