ACTA BIOMEDICA SUPPLEMENT Atenei Parmensis | Founded 1887
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
OUR PLACE in the UNIVERSE DR CHARLES Lineweaver
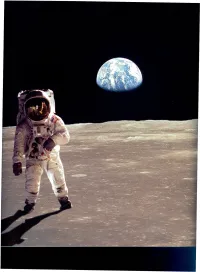
• I. WHERE ARE WE? Fig. 5b Earth from Moon with astronaut in foreground. In a canoe called the Earth, we are drifting down an unknown river. We Courtesy NASA (68·H·1401 and ASll-40-5903) What lies around the next bend? Some of us hear an ominous roar ahead - a water~ Some of us see the stream broadening and an immense unknown ocean on the horizon. We are on a journey through time. We may encounter other life forms or there may be j OrCharles Lineweaver is an billions of lifeless shores. We paddle and stab at the water trying to avoid jutting Australian Research Fellow in the School of Physics at the University of New South Wales. boulders and eddies. Many of us are bailing. We bail for about 80 years, then we give He studied undergraduate physics at Ludwig Maximillian Universitat, Germany and at our scoops and paddles to our children. If our canoe holds - if we can see far enough Kyoto University, Japan. He obtained his PhD from the University of California at ahead to avoid waterfalls and whirlpools, then surely our children's children's children... Berkeley for research on COBE satellite observations of the cosmic microwave background. will live to see this river empty into a placid infinite ocean. In the dark of the night, we After a postdoctoral fellowship in Strasbourg, France, he came gaze at the heavens and wonder who we are. How did we get on this canoe? to UNSWin 1997. He speaks four languages and has played semi· professional soccer. -

Light in and Sound Out: Emerging Translational Strategies for Photoacoustic Imaging
Published OnlineFirst February 10, 2014; DOI: 10.1158/0008-5472.CAN-13-2387 Cancer Review Research Light In and Sound Out: Emerging Translational Strategies for Photoacoustic Imaging S. Zackrisson1,2,3,4,5, S.M.W.Y. van de Ven1,2,3,4, and S.S. Gambhir1,2,3,4 Abstract Photoacoustic imaging (PAI) has the potential for real-time molecular imaging at high resolution and deep inside the tissue, using nonionizing radiation and not necessarily depending on exogenous imaging agents, making this technique very promising for a range of clinical applications. The fact that PAI systems can be made portable and compatible with existing imaging technologies favors clinical translation even more. The breadth of clinical applications in which photoacoustics could play a valuable role include: noninvasive imaging of the breast, sentinel lymph nodes, skin, thyroid, eye, prostate (transrectal), and ovaries (transvaginal); minimally invasive endoscopic imaging of gastrointestinal tract, bladder, and circulating tumor cells (in vivo flow cytometry); and intraoperative imaging for assessment of tumor margins and (lymph node) metastases. In this review, we describe the basics of PAI and its recent advances in biomedical research, followed by a discussion of strategies for clinical translation of the technique. Cancer Res; 74(4); 979–1004. Ó2014 AACR. Introduction In this review, we will first describe the basics of PAI, Photoacoustic imaging (PAI), also referred to as optoacous- followed by a comprehensive overview of its clinical applica- tic imaging, is an emerging new imaging technique with tions. We will then discuss strategies for future translation to significant promise for biomedical applications. The key clinical practice. -

Deliverable D.8.3 Literature Review of On-Line Bioprocess Monitoring
NANOBE SEVENTH FRAMEWORK PROGRAMME THEME 2 Food, Agriculture and Fisheries, and Biotechnology Grant Agreement no: 227243 Project acronym: NANOBE Project title: Nano- and microtechnology –based analytical devices for online measurements of bioprocesses Funding Scheme: CA Deliverable D.8.3 Literature review of on-line bioprocess monitoring Report Due date of delivery: Month 18 Actual date of delivery: November 26th 2010 Responsible authors: Juha-Pekka Pitkänen (VTT), Heidi Turkia (VTT) Co-operative authors: Heli Sirén (VTT), Anna Rissanen (VTT), Guillaume Mernier (EPFL), Frédéric Reymond (DiagnoSwiss), Karen Lemke (iba), Francois Brunelle (CNRS-IEMN), Päivi Heimala (VTT) Project co-funded by the European Community's Seventh Framework Programme FP7 (2007-2013) Dissemination level PU Public PU PP Restricted to other programme participants (including the Commission Services) Restricted to a group specified by the consortium (including the Commission RE Services) Confidential, only for members of the consortium (including the Commission CO Services) Deliverable D.8.3 NANOBE GA no. 227243 TABLE OF CONTENTS TABLE OF CONTENTS 2 1 SUMMARY 3 2 PURPOSE AND SCOPE 3 3 INTRODUCTION 3 4 MEASUREMENT APPROACHES 8 4.1 Optical measurements 8 4.1.1 Optical single point measurements 8 4.1.2 Imaging measurements 9 4.2 Electrical measurements 10 4.3 Measurements based on chromatography-like separation 12 4.3.1 On-line capillary electrophoresis 12 4.3.2 On-line liquid chromatography 12 4.3.3 On-line gas chromatography 14 4.4 Direct mass spectrometric measurements 14 4.5 Measurements where biological component aids in recognition 15 5 SAMPLING AND SAMPLE TREATMENT APPROACHES 15 5.1 Automated sampling 16 5.2 Sample fractionation 18 5.3 Cell lysis 18 6 CONCLUSIONS 19 7 REFERENCES 19 2/25 Deliverable D.8.3 NANOBE GA no. -

Essa, Wisam Hindawi Hoidy, Spectrophotometric Determination
160 Nano Biomed. Eng., 2020, Vol. 12, Iss. 2 Nano Biomed Eng 2020, 12(2): 160-166. doi: 10.5101/nbe.v12i2.p160-166. Research Article Spectrophotometric Determination of Cobalt(II) and Lead(II) Using (1,5-Dimethyl-2-Phenyl-4-((2,3,4- Trihydroxy Phenyl) Diazenyl)-1H-Pyrazol-3(2H)-One) as Organic Reagent: Using It as Antimicrobial and Antioxidants Shaimaa Mohsen. Essa , Wisam Hindawi Hoidy Department of Chemistry, College of Education, University of Al-Qadisiyah, Al-Qadisiyah, Iraq. Corresponding author. E-mail: [email protected] Received: Mar. 27, 2020; Accepted: Apr. 17, 2020; Published: Jun. 3, 2020 Citation: Shaimaa Mohsen. Essa, Wisam Hindawi Hoidy, Spectrophotometric Determination of Cobalt(II) and Lead(II) Using (1,5-Dimethyl-2- Phenyl-4-((2,3,4-Trihydroxy Phenyl) Diazenyl)-1H-Pyrazol-3(2H)-One) as Organic Reagent: Using It as Antimicrobial and Antioxidants. Nano Biomed. Eng., 2020, 12(2): 160-166. DOI: 10.5101/nbe.v12i2.p160-166. Abstract The azo organic reagent (1,5-dimethyl-2-phenyl-4-((2,3,4-trihydroxy phenyl) diazenyl)-1H-pyrazol- 3(2H)-one) (DPTPD) was prepared and used for the spectrophotometric determination of cobalt(II) and Lead(II), by the selective and surfactant-sensitized method based on the ternary complexes formation of Co(II) and Pb(II). The reagent had absorption maximum at 381 nm, and reacted with 2+ Co to form a purple reddish complex with λmax = 430 nm at pH = 7.5, while it formed a red complex 2+ with Pb of λmax = 417 nm at pH= 6. Beer's law for the determination over the range of 1-25 ppm and 1-33 ppm for Co(II) and Pb(II), respectively. -

Nanobacterial System Towards Biofilm Forming Pseudomonas Oryzihabitans
Nano Biomed. Eng., 2019, Vol. 11, Iss. 3 297 Nano Biomed Eng 2019, 11(3): 297-305. doi: 10.5101/nbe.v11i3.p297-305. Research Article Silver Nanoparticles as an Effective Anti- Nanobacterial System towards Biofilm Forming Pseudomonas oryzihabitans Shaimaa Obaid Hasson1 , Mohammed Jabber Al-Awady2, Mohanad Jawad Kadhim2, Hayder Shkhair Al-Janabi2 1Department of Microbiology, College of Veterinary, Al-Qasim Green University, Babylon, Iraq. 2Department of Genetic Engineering, Faculty of Biotechnology, Al Qasim Green University, Babylon, Iraq. Corresponding author. E-mail: [email protected] Received: Jun. 18, 2019; Accepted: Aug. 22, 2019; Published: Aug. 23, 2019. Citation: Shaimaa Obaid Hasson, Mohammed Jabber Al-Awady, Mohanad Jawad Kadhim, and Hayder Shkhair Al-Janabi, Silver Nanoparticles as an Effective Anti-Nanobacterial System towards Biofilm FormingPseudomonas oryzihabitans. Nano Biomed. Eng., 2019, 11(3): 297-305. DOI: 10.5101/nbe.v11i3.p297-305. Abstract Silver nanoparticles have been considered a powerful antimicrobial agents recently especially after increasing incidence of diseases associated with biofilm and multi-drug resistant pathogens required to find a novel path to eradicate that challenge. The present study aims to evaluate the antibacterial activity of biosynthesized silver nanoparticles (AgNPs) using a cell-free extract of Enterobacter cloacae and chemo synthesis by sodium borohydride (NaBH4) on biofilm-forming Pseudomonas oryzihabitans. Antimicrobial effect of silver nanoparticles in both types and in combination with imipenem were evaluated by agar well diffusion method. The results revealed a good response to inhibit biofilm-forming Pseudomonas oryzihabitans growth by silver nanoparticles antibacterial activity in both types (biological and chemical) and in combination with imipenem; the antimicrobial effect was increased and enhanced. -

Emerging Translational Strategies for Photoacoustic Imaging
Published OnlineFirst February 10, 2014; DOI: 10.1158/0008-5472.CAN-13-2387 Cancer Review Research Light In and Sound Out: Emerging Translational Strategies for Photoacoustic Imaging S. Zackrisson1,2,3,4,5, S.M.W.Y. van de Ven1,2,3,4, and S.S. Gambhir1,2,3,4 Abstract Photoacoustic imaging (PAI) has the potential for real-time molecular imaging at high resolution and deep inside the tissue, using nonionizing radiation and not necessarily depending on exogenous imaging agents, making this technique very promising for a range of clinical applications. The fact that PAI systems can be made portable and compatible with existing imaging technologies favors clinical translation even more. The breadth of clinical applications in which photoacoustics could play a valuable role include: noninvasive imaging of the breast, sentinel lymph nodes, skin, thyroid, eye, prostate (transrectal), and ovaries (transvaginal); minimally invasive endoscopic imaging of gastrointestinal tract, bladder, and circulating tumor cells (in vivo flow cytometry); and intraoperative imaging for assessment of tumor margins and (lymph node) metastases. In this review, we describe the basics of PAI and its recent advances in biomedical research, followed by a discussion of strategies for clinical translation of the technique. Cancer Res; 74(4); 1–26. Ó2014 AACR. Introduction In this review, we will first describe the basics of PAI, Photoacoustic imaging (PAI), also referred to as optoacous- followed by a comprehensive overview of its clinical applica- tic imaging, is an emerging new imaging technique with tions. We will then discuss strategies for future translation to significant promise for biomedical applications. The key clinical practice. -

Ticle Adsorption
C. Meng et al. nanobe.org OPEN ACCESS Article Nano Biomed Eng ISSN 2150-5578 http://nanobe.org Development of a Rapid and Convenient Method for Sampling Airborne Virus based on Nanopar- ticle Adsorption Chun Meng*, Yulin Xiong, Weiliang Zhuang, Hang Wang, Xian’ai Shi, Yanghao Guo Department of Bioengineering, College of Biological Science and Biotechnology, Fuzhou University, Fuzhou, Fujian 350108, China. *Corresponding authors. Email: [email protected], Tel: 86-591-22866379, Fax: 86-591-22866379 Abstract An improved aerobiological virus sampling method was developed based on adding adsorptive nanoparticles in samplers for concentrating viruses in sampling liquid buffers. The objectives of this research were to select effective adsorptive materials and optimize sampling parameters for increasing recovery of airborne viruses, such as influenza A virus or respiratory syndrome virus (RSV). Three kinds of polycation nanoparticles were evaluated for direct effects on absorption and desorption of influenza virus hemagglutinin and DNA. Chitosan particles showed good performance in absorption and desorption for both influenza virus hemagglutinin and DNA. A subsequent study evaluated the effects of collection buffer, pH and sampling time on the recovery of aerosolized viruses using a method for making direct comparisons of three treatments. The results demonstrated that various components in air-sampling collection buffer, impinger model, and sampling time, independently influenced the recovery of viruses. It was shown that adsorptive samplers with air disperser had the highest levels of sensitivity and repeatability in virus sampling. Both unspecifically adsorptive chitosan particles and specifically adsorptive particles labeled specific antibody to virus significantly enhanced recovery rate of aerosolized viruses. We succeeded to sample low level different pathogen viruses in outdoor environments with the optimized sampling system. -

Immunoengineered Magnetic-Quantum Dot Nanobead
Zhang et al. J Nanobiotechnol (2021) 19:116 https://doi.org/10.1186/s12951-021-00860-1 Journal of Nanobiotechnology RESEARCH Open Access Immunoengineered magnetic-quantum dot nanobead system for the isolation and detection of circulating tumor cells Pengfei Zhang1,2† , Mohamed S. Draz3,4,5†, Anwen Xiong6†, Wannian Yan2, Huanxing Han1,7* and Wansheng Chen1,8* Abstract Background: Highly efcient capture and detection of circulating tumor cells (CTCs) remain elusive mainly because of their extremely low concentration in patients’ peripheral blood. Methods: We present an approach for the simultaneous capturing, isolation, and detection of CTCs using an immuno-fuorescent magnetic nanobead system (iFMNS) coated with a monoclonal anti-EpCAM antibody. Results: The developed antibody nanobead system allows magnetic isolation and fuorescent-based quantifcation of CTCs. The expression of EpCAM on the surface of captured CTCs could be directly visualized without additional immune-fuorescent labeling. Our approach is shown to result in a 70–95% capture efciency of CTCs, and 95% of the captured cells remain viable. Using our approach, the isolated cells could be directly used for culture, reverse transcription-polymerase chain reaction (RT-PCR), and immunocytochemistry (ICC) identifcation. We applied iFMNS for testing CTCs in peripheral blood samples from a lung cancer patient. Conclusions: It is suggested that our iFMNS approach would be a promising tool for CTCs enrichment and detection in one step. Keywords: Magnetic nanoparticle, Quantum dots, Fluorescent magnetic nanobeads, Circulating tumor cells, Simultaneous capture and detection Introduction 5]. Compared with other early cancer diagnostic tools, Circulating tumor cells (CTCs) are free tumor cells shed such as genetic or metabolite omics analysis [6–8], cap- from original or metastatic tumors into the peripheral tured CTCs could provide more information for further blood [1–3]. -

Novel Nano-Organisms from Australian Sandstones
American Mineralogist, Volume 83, pages 1541±1550, 1998 Novel nano-organisms from Australian sandstones PHILIPPA J.R. UWINS,1,* RICHARD I. WEBB,1 and ANTHONY P. TAYLOR1,2 1Centre for Microscopy and Microanalysis, The University of Queensland, St. Lucia, Queensland, Australia 4072 2Department of Microbiology, The University of Queensland, St. Lucia, Queensland, Australia 4072 ABSTRACT We report the detection of living colonies of nano-organisms (nanobes) on Triassic and Jurassic sandstones and other substrates. Nanobes have cellular structures that are strikingly similar in morphology to Actinomycetes and fungi (spores, ®laments, and fruiting bodies) with the exception that they are up to 10 times smaller in diameter (20 nm to 1.0 mm). Nanobes are noncrystalline structures that are composed of C, O, and N. Ultra thin sections of nanobes show the existence of an outer layer or membrane that may represent a cell wall. This outer layer surrounds an electron dense region interpreted to be the cytoplasm and a less electron dense central region that may represent a nuclear area. Nanobes show a positive reaction to three DNA stains, [49,6-diamidino-2 phenylindole (DAPI), Acridine Orange, and Feulgen], which strongly suggests that nanobes contain DNA. Nanobes are communicable and grow in aerobic conditions at atmospheric pressure and ambient tem- peratures. While morphologically distinct, nanobes are in the same size range as the con- troversial fossil nannobacteria described by others in various rock types and in the Martian meteorite ALH84001. INTRODUCTION Molecular analysis indicated that the ``nanobacteria'' iso- The identi®cation and existence of nannobacteria have lated from fetal bovine serum are members of the alpha- been proposed (Folk 1993; Sillitoe et al. -
Tgd Based View About Living Matter and Remote Mental Interactions
1 TGD BASED VIEW ABOUT LIVING MATTER AND REMOTE MENTAL INTERACTIONS Matti Pitk¨anen K¨oydenpunojankatuD 11, 10900, Hanko, Finland iii Preface This book belongs to a series of online books summarizing the recent state Topological Geometro- dynamics (TGD) and its applications. TGD can be regarded as a unified theory of fundamental interactions but is not the kind of unified theory as so called GUTs constructed by graduate stu- dents at seventies and eighties using detailed recipes for how to reduce everything to group theory. Nowadays this activity has been completely computerized and it probably takes only a few hours to print out the predictions of this kind of unified theory as an article in the desired format. TGD is something different and I am not ashamed to confess that I have devoted the last 32 years of my life to this enterprise and am still unable to write The Rules. I got the basic idea of Topological Geometrodynamics (TGD) during autumn 1978, perhaps it was October. What I realized was that the representability of physical space-times as 4-dimensional surfaces of some higher-dimensional space-time obtained by replacing the points of Minkowski space with some very small compact internal space could resolve the conceptual difficulties of general rela- tivity related to the definition of the notion of energy. This belief was too optimistic and only with the advent of what I call zero energy ontology the understanding of the notion of Poincare invariance has become satisfactory. It soon became clear that the approach leads to a generalization of the notion of space-time with particles being represented by space-time surfaces with finite size so that TGD could be also seen as a generalization of the string model. -

TGD Inspired Model for Nerve Pulse Contents
CONTENTS 1 TGD Inspired Model for Nerve Pulse M. Pitk¨anen,January 29, 2011 Email: [email protected]. http://tgd.wippiespace.com/public_html/. Recent postal address: K¨oydenpunojankatu 2 D 11, 10940, Hanko, Finland. Contents 1 Introduction 4 1.1 General vision about living matter as a macroscopic quantum system . .5 1.2 A general view about quantum control, coordination and communication inspired by dark matter hierarchy . .6 1.3 The role of electronic super-conductivity . .6 1.3.1 General mechanisms of bio-superconductivity . .6 1.3.2 Bose-Einstein condensates at magnetic flux quanta in astrophysical length scales7 1.3.3 Experimental evidence for bio-superconductivity . .8 1.3.4 Strange findings about cell membrane . .8 1.4 The role of MEs and magnetic flux tube circuitry . .9 1.4.1 Universe as a conscious hologram . .9 1.4.2 Various kinds of MEs . .9 1.4.3 The strange effects of ELF em fields on vertebrates as a key to the model for hierarchy of EEGs . 10 1.5 The most recent model for the generation of nerve pulse . 10 1.6 What happens at the micro-tubular level during nerve pulse? . 11 2 Exotic charge transfer between cell interior and exterior as fundamental control mechanism 12 2.1 Strange behavior of the intracellular water . 12 2.2 Are channels and pumps really there? . 13 2.2.1 Selectivity problem . 13 2.2.2 Inflation in the number of pumps and channels . 14 2.2.3 Why pumping does not stop when metabolism stops? . 14 2.2.4 How it is possible that ionic currents through silicon rubber membrane are similar to those through cell membrane? . -

Clinical Trial Analysis of Different Stages of HBV Patients Treated with Human CIK Cells
Nano Biomed. Eng., 2016, Vol. 8, Iss. 3 203 Nano Biomed Eng 2016, 8(3): 203-211. doi: 10.5101/nbe.v8i3.p203-211. Research Article Clinical Trial Analysis of Different Stages of HBV Patients Treated with Human CIK Cells Fangfang Xia1, Ruihua Song2, Jingjing Zhang1, Yang Zhu2, Yao Yang1, Ling He1, Yun Cao1, Chenlu Li1, Zheng Wang1, Shangli Cheng1, Jian Ni1, Lijun Ma3 , Ding Li2 , Daxiang Cui1 1Institute of Nano Biomedicine and Engineering, Shanghai Engineering Research Center for Intelligent Diagnosis and Therapy Instrument, Department of Instrument Science and Engineering, School of Electronic Information and Electrical Engineering; National Center for Translational Medicine, Collaborative Innovational Center for System Biology, Shanghai Jiao Tong University, 800 Dongchuan Road, Shanghai 200240, P. R. China. 2Center for Biotechnological Diagnosis and Therapy, The 261 Hospital of PLA, Beijing 100094, China. 3Department of Oncology, Shanghai Tongren Hospital, Shanghai JiaoTong University School of Medicine, 1111 Xianxia Road, Shanghai 200336, P. R. China. Corresponding authors. E-mail: [email protected]; [email protected]; [email protected] Received: Sep. 21, 2016; Accepted: Sep. 28, 2016; Published: Sep. 29, 2016. Citation: Fangfang Xia, Ruihua Song, Jingjing Zhang, Yang Zhu, Yao Yang, Ling He, Yun Cao, Chenlu Li, Zheng Wang, Shangli Cheng, Jian Ni, Lijun Ma, Ding Li and Daxiang Cui, Clinical Trial Analysis of Different Stages of HBV Patients Treated with Human CIK Cells. Nano Biomed. Eng., 2016, 8(3): 203-211. DOI: 10.5101/nbe.v8i3.p203-211. Abstract Cellular immunotherapy has become a potential therapeutic method for different diseases. Herein, we reported clinical trial results of Cytokine-induced killer (CIK) cells used for patients with hepatitis B, cirrhosis and liver cancers from 2000 to 2015.