Health Cluster Bulletin
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Aid in Danger Monthly News Brief, Nigeria February 2017
The Aid in Danger February Monthly News Brief 2017 Security Incidents This monthly digest comprises threats and incidents of violence affecting the delivery Africa of humanitarian assistance. It Cameroon is prepared by Insecurity 31 January 2017: In the vicinity of Hosere Jongbi area, near the town Insight from information of Kontcha, an unknown armed group attacked a UN Technical available in open sources. Monitoring Team, killing five individuals, including a UN independent contractor, three Nigerians and one Cameroonian, and injuring All decisions made on the several others. Sources: Premium Times and The News basis of, or with consideration to, such information remains Central African Republic the responsibility of their 02 February 2017: In Bocaranga sub-prefecture, Ouham-Pendé respective organisations. prefecture, an unspecified armed group attacked and plundered the compounds of three non-governmental organisations (NGOs): Editorial team: MENTOR, CORDAID and DRC. Source: RJDH Christina Wille Insecurity Insight 10 February 2017: In the capital Bangui, gunmen stormed a hospital Larissa Fast in PK5 neighbourhood twice within five days to kill patients. Source: Insecurity Insight The Citizen Adelicia Fairbanks European Interagency Security Democratic Republic of the Congo Forum (EISF) 22 February 2017: In Kasai Oriental and Upper Katanga, unidentified assailants broke into and vandalised a number of churches engaged Research team: in poverty work for the local population. Source: Radio Okapi Insecurity Insight Kenya Visit our website to download 24 February 2017: In Baringo county, local residents blocked seven previous Aid in Danger Kenya Red Cross Society vehicles carrying 96.8 metric tonnes of Monthly News Briefs. humanitarian assistance, which led to looting of relief aid and harassment of aid staff. -
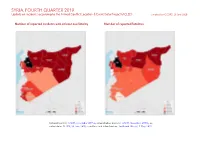
SYRIA, FOURTH QUARTER 2019: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 23 June 2020
SYRIA, FOURTH QUARTER 2019: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 23 June 2020 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; in- cident data: ACLED, 20 June 2020; coastlines and inland waters: Smith and Wessel, 1 May 2015 SYRIA, FOURTH QUARTER 2019: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 23 JUNE 2020 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Explosions / Remote Conflict incidents by category 2 3058 397 1256 violence Development of conflict incidents from December 2017 to December 2019 2 Battles 1023 414 2211 Strategic developments 528 6 10 Methodology 3 Violence against civilians 327 210 305 Conflict incidents per province 4 Protests 169 1 9 Riots 8 1 1 Localization of conflict incidents 4 Total 5113 1029 3792 Disclaimer 8 This table is based on data from ACLED (datasets used: ACLED, 20 June 2020). Development of conflict incidents from December 2017 to December 2019 This graph is based on data from ACLED (datasets used: ACLED, 20 June 2020). 2 SYRIA, FOURTH QUARTER 2019: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 23 JUNE 2020 Methodology GADM. Incidents that could not be located are ignored. The numbers included in this overview might therefore differ from the original ACLED data. -

Field Developments in Idleb 51019
Field Developments in Idleb, Northern Hama Countryside, Western Situation Report and Southern Aleppo Countryside During March and April 2019 May 2019 Aleppo Countrysides During March and April 2019 the Information Management Unit 1 Field Developments in Idleb, Northern Hama Countryside, Western and Southern Aleppo Countryside During March and April 2019 The Assistance Coordination Unit (ACU) aims to strengthen the decision-making capacity of aid actors responding to the Syrian crisis. This is done through collecting, analyzing and sharing information on the humanitarian situation in Syria. To this end, the Assistance Coordination Unit through the Information Management Unit established a wide net- work of enumerators who have been recruited depending on specific criteria such as education level, association with information sources and ability to work and communicate under various conditions. IMU collects data that is difficult to reach by other active international aid actors, and pub- lishes different types of information products such as Need Assessments, Thematic Reports, Maps, Flash Reports, and Interactive Reports. 2 Field Developments in Idleb, Northern Hama Countryside, Western Situation Report and Southern Aleppo Countryside During March and April 2019 May 2019 During March and April 2019 3 Field Developments in Idleb, Northern Hama Countryside, Western and Southern Aleppo Countryside During March and April 2019 01. The Most Prominent Shelling Operations During March and April 2019, the Syrian regime and its Russian ally shelled Idleb Governorate and its adjacent countrysides of Aleppo and Hama governorates, with hundreds of air strikes, and artillery and missile shells. The regime bombed 14 medical points, including hospitals and dispensaries; five schools, including a kinder- garten; four camps for IDPs; three bakeries and two centers for civil defense, in addition to more than a dozen of shells that targeted the Civil Defense volunteers during the evacuation of the injured and the victims. -
Epidemiological Findings of Major Chemical Attacks in the Syrian War Are Consistent with Civilian Targeting: a Short Report Jose M
Rodriguez-Llanes et al. Conflict and Health (2018) 12:16 https://doi.org/10.1186/s13031-018-0150-4 SHORTREPORT Open Access Epidemiological findings of major chemical attacks in the Syrian war are consistent with civilian targeting: a short report Jose M. Rodriguez-Llanes1, Debarati Guha-Sapir2 , Benjamin-Samuel Schlüter2 and Madelyn Hsiao-Rei Hicks3* Abstract Evidence of use of toxic gas chemical weapons in the Syrian war has been reported by governmental and non-governmental international organizations since the war started in March 2011. To date, the profiles of victims of the largest chemical attacks in Syria remain unknown. In this study, we used descriptive epidemiological analysis to describe demographic characteristics of victims of the largest chemical weapons attacks in the Syrian war. We analysed conflict-related, direct deaths from chemical weapons recorded in non-government-controlled areas by the Violation Documentation Center, occurring from March 18, 2011 to April 10, 2017, with complete information on the victim’s date and place of death, cause and demographic group. ‘Major’ chemical weapons events were defined as events causing ten or more direct deaths. As of April 10, 2017, a total of 1206 direct deaths meeting inclusion criteria were recorded in the dataset from all chemical weapons attacks regardless of size. Five major chemical weapons attacks caused 1084 of these documented deaths. Civilians comprised the majority (n = 1058, 97.6%) of direct deaths from major chemical weapons attacks in Syria and combatants comprised a minority of 2.4% (n = 26). In the first three major chemical weapons attacks, which occurred in 2013, children comprised 13%–14% of direct deaths, ranging in numbers from 2 deaths among 14 to 117 deaths among 923. -

Attacks on Health Care July Monthly News Brief 2019
Attacks on Health Care July Monthly News Brief 2019 SHCC Attacks on Health Care This monthly digest The section aligns with the definition of attacks on health care used by the comprises threats and (SHCC). Safeguarding Health in Conflict Coalition violence as well as Please also see WHO SSA table on the last page of this document protests and other events affecting the delivery of Africa and access to health care. Burkina Faso 26 July 2019: In Konga, Gomboro district, Sourou province, suspected Katiba Macina militants reportedly kidnapped the manager of a It is prepared by pharmacy at an unnamed medical centre. Source: ACLED1 Insecurity Insight from information available in 13 July 2019: In Noukeltouoga, Gourma province, Est region, open sources. suspected JNIM and/or ISGS militants reportedly kidnapped a vaccination volunteer. Source: ACLED1 All decisions made, on the Cameroon basis of, or with 17 July 2019: In Bamenda, Mezam district, Nord-Ouest province, two consideration to, such doctors were reportedly kidnapped by an unidentified armed group information remains the and released 24 hours later. Sources: Maikemsdairy and Journal du responsibility of their Cameroun respective organisations. Central African Republic 05 July 2019: In Ouham prefecture, two national aid workers for an Data from the Attacks on INGO were reportedly assaulted while transporting two patients on Health Care Monthly motorcycles in the Ouham prefecture. The aid workers were ambushed, News Brief is available on robbed, and assaulted by armed men suspected to be MPC/FPRC. HDX Insecurity Insight. Source: AWSD2 Democratic Republic of the Congo Subscribe here to receive 13-14 July 2019: In Mukulia village, North Kivu province, unidentified monthly reports on attackers killed two national Ebola health workers for unascertained insecurity affecting the reasons. -
L:>Rs(Olf/Vof
ORGANISATION FOR THE PROHIBITION OF CHEMICAL WEAPONS Dirutor-Ctntral OPCW The lf<lgue, 18 December 2014 ?014 OEC 2 3 Johan de \V ittl.>"n 31 1./()!)(Jill)5480/14 I q--- II 8 J--i 2517 JR The Ha)!U< !:....... ...��4._�·; i/� ..,.. !.: t l t•l;_ �� Tht' Nethnbnds o:F 'i llc ;,t.Q.l;J:.:ut)'.GE.NERAI. Tdcphone:+ 31(0)704103702/o-t ht: + 31 (o)jo 410 37 91. E-mail: ahmct.uzumcu(t!)opcw.urg Excellency, I have the honour to transmit to you the Third Report of the Organisation t()r the Prohibition of I Chemical Weapons Fact-Finding Mission in Syria. As you know the Mission was mandated to J I establish the !acts surrounding allegations of the usc of toxic chemicals, reportedly chlorine, f()r I hostile purposes in the Syrian Arab Republic. I This repoti will be circulated today in ·nlC I !ague to States Parties to the Chemical Weapons Convention. IIY. Mr Ban K i-tn0l)l1 Sccrdary-Gcncral ol"the United Nations United Nations llcadquartcrs New York l:>rs(olf/vof ORGANISATION FOR THE PROHIBITION OF CHEMICAL WEAPONS Dirutor-General OPCW The Hague, 18 December 2014 Johan de Witdaan 32 1./0DG/195480/14 2517 )R The Hague The Netherlands Telephone: + 31 ( o )70 416 37 02/04 Fax:+ 31 (0)70 416 37 92 E-mail: [email protected] Excellency, I have the honour to transmit to you the Third Report of the Organisation for the Prohibiti on of Chemical Weapons Fact-Finding Mission in Syria. -

September 2016
www.rbs0.com/syria37.pdf 1 Oct 2016 Page 1 of 234 Syria & Iraq: September 2016 Copyright 2016 by Ronald B. Standler No copyright claimed for quotations. No copyright claimed for works of the U.S. Government. Table of Contents 1. Chemical Weapons U.N. Security Council begins to ask who used chemical weapons in Syria? ISIL used mustard in Iraq (11 Aug 2015) 2. Syria United Nations Diverted from Syria death toll in Syria now over 301,000 (30 Sep) Free Syrian Army is Leaderless since June 2015 Turkey is an ally from Hell U.S. troops in Syria Recognition that Assad is Winning the Civil War Peace Negotiations for Syria Future of Assad must be decided by Syrians Planning for Peace Negotiations in Geneva New Russia/USA Agreements (9 Sep) U.N. Security Council meeting (21 Sep) Syrian speech to U.N. General Assembly (24 Sep) more meetings and negotiations 22-30 Sep 2016 Friends of Syria meeting in London (7 Sep) ISSG meetings (20, 22 Sep 2016) occasional reports of violations of the Cessation of Hostilities agreement proposed 48-hour ceasefires in Aleppo siege of Aleppo (1-12 Sep} Violations of new agreements in Syria (12-19 Sep) continuing civil war in Syria (20-30 Sep) bombing hospitals in Syria surrender of Moadamiyeh U.N. Reports war crimes prosecution? 3. Iraq Atrocities in Iraq No Criminal Prosecution of Iraqi Army Officers No Prosecution for Fall of Mosul No Prosecution for Rout at Ramadi No Criminal Prosecution for Employing "Ghost Soldiers" www.rbs0.com/syria37.pdf 1 Oct 2016 Page 2 of 234 Iraq is a failed nation U.S. -

Ongoing Chemical Weapons Attacks in Syria
A NEW NORMAL Ongoing Chemical Weapons Attacks in Syria February 2016 SYRIAN AMERICAN MEDICAL SOCIETY C1 Above: Bab Al Hawa Hospital, Idlib, April 21, 2014. On the cover, top: Bab Al Hawa Hospital, Idlib, April 21, 2014; bottom: Binnish, Idlib, March 23, 2015. ABOUT THE SYRIAN AMERICAN MEDICAL SOCIETY The Syrian American Medical Society (SAMS) is a non-profit, non-political, professional and medical relief orga- nization that provides humanitarian assistance to Syrians in need and represents thousands of Syrian American medical professionals in the United States. Founded in 1998 as a professional society, SAMS has evolved to meet the growing needs and challenges of the medical crisis in Syria. Today, SAMS works on the front lines of crisis relief in Syria and neighboring countries to serve the medical needs of millions of Syrians, support doctors and medical professionals, and rebuild healthcare. From establishing field hospitals and training Syrian physicians to advocating at the highest levels of government, SAMS is working to alleviate suffering and save lives. Design: Sensical Design & Communication C2 A NEW NORMAL: Ongoing Chemical Weapons Attacks in Syria Acknowledgements New Normal: Ongoing Chemical Weapons Attacks in Syria was written by Kathleen Fallon, Advocacy Manager of the Syrian Amer- A ican Medical Society (SAMS); Natasha Kieval, Advocacy Associate of SAMS; Dr. Zaher Sahloul, Senior Advisor and Past President of SAMS; and Dr. Houssam Alnahhas of the Union of Medical Care and Relief Or- ganizations (UOSSM), in partnership with many SAMS colleagues and partners who provided insight and feedback. Thanks to Laura Merriman, Advocacy Intern of SAMS, for her research and contribution to the report’s production. -

La Voix De L'opposition De Gauche - Causeries Et Infos En Bref Septembre 2018
La voix de l'Opposition de gauche - Causeries et infos en bref septembre 2018 Causeries septembre 2018 janvier février mars avril mai juin juillet août septembre octobre novembre décembre 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 Le 4 septembre 2018 CAUSERIE ET INFOS Causerie au format pdf (22 pages) La causerie d'août est disponible au format pdf, 178 pages, tu parles de vacances ! J'ai posté trois commentaires sur le blog Les Crises à la suite d'un article sur les banques. Et je dois avouer à ma grande surprise (feinte) que j'ai plus de succès qu'avec les internautes qui se connectent à mon portail, c'est le comble ! On se détend un peu, est-ce que j'ai l'air crispé franchement ? Et pourtant j'aurai de quoi l'être depuis que la CNAV a cessé de me verser ma retraite depuis le mois de mai. Attendez, hier j'ai reçu un message m'apprenant que ma situation pourrait être régularisée au mieux d'ici 4 à 6 semaines ! Quel recours ai-je pour faire valoir mes droits ? Absolument aucun. J'invite les agents de la CNAV à boycotter la journée d'action bidon du 9 octobre pour ne pas retarder davantage le traitement de mon dossier... Heureusement que j'ai pensé à faire des réserves au cas où, comme l'on dit, j'ai de quoi tenir au moins 2 ans! J'ai peut-être l'air con et la vue basse (ou qui baisse c'est vrai), mais depuis que je consacre un peu plus de temps à mes propres affaires, je ne me laisse plus prendre au dépourvu. -

Attacks on Health Care March 2021 Monthly News Brief
March Attacks on Health Care 2021 Monthly News Brief Insecurity Insight publishes data on incidents where health workers were killed, kidnapped or arrested (KKA) and incidents where health facilities were damaged or destroyed by a perpetrator including state and non-state actor groups, criminals, individuals, students and other staff members. Access the data via our website or on HDX. Past editions: February 2021; January 2021 Visit our website, join our mailing list, follow us on Twitter and Facebook. Get in touch to report an incident or if you have additional information on an incident we have reported on. SHCC Attacks on Health Care The section aligns with the definition of attacks on health care used by the Safeguarding Health in Conflict Coalition (SHCC). Africa Cameroon 01 March 2021: In Kikaikilaki locality, Bui department, Northwest province, following a gun battle, soldiers shot at the Life Abundant Primary Health Care Project, allegedly mistaking it for a separatist hideout. The health facility caught fire, resulting in unknown amounts of damage to the building. Source: Mimi Mefo Info Democratic Republic of the Congo 13 March 2021: In Kalalangwe village, North Kivu province, alleged ADF militants entered a local clinic and killed three patients, including one woman, with machetes and guns. Source: Actualité Mali 03 March 2021: In Bentia village, Goa region, a local health centre was robbed by armed men. No injuries or deaths were reported; however, the perpetrators stole the health centre’s motorbike. Source: Studio Tamani 15 March 2021: In Diouradougou commune, Koutiala cercle, Sikasso region, unidentified men kidnapped six health workers. -

SYRIA - IDLEB Humanitarian Purposes Only IDP Location - As of 23 Oct 2015 Production Date : 26 Oct 2015
SYRIA - IDLEB Humanitarian Purposes Only IDP Location - As of 23 Oct 2015 Production date : 26 Oct 2015 Nabul Al Bab MARE' JANDAIRIS AFRIN NABUL Tadaf AL BAB Atma ! Qah ² ! Daret Haritan Azza TADAF Reyhanli DARET AZZA HARITAN DANA Deir Hassan RASM HARAM !- Darhashan Harim Jebel EL-IMAM Tlul Dana ! QOURQEENA Saman Antakya Ein Kafr Hum Elbikara Big Hir ! ! Kafr Mu Jamus ! Ta l ! HARIM Elkaramej Sahara JEBEL SAMAN Besnaya - Sarmada ! ! Bseineh Kafr ! Eastern SALQIN ! Qalb Ariba Deryan Kafr ! Htan ! Lozeh ! Kafr Naha Kwaires ! Barisha Maaret ! ! Karmin TURKEY Allani ! Atarib ! Kafr Rabeeta ! Radwa ! Eskat ! ! Kila ! Qourqeena Kafr Naseh Atareb Elatareb Salqin Kafr ! EASTERN KWAIRES Delbiya Meraf ! Kafr Elshalaf Takharim Mars ! Kafr ! Jeineh Aruq ! Ta lt i t a ! Hamziyeh ! Kelly ! Abu ! Ta lh a ATAREB ! Kaftin Qarras KAFR TAKHARIMHelleh ! Abin ! Kafr ! Hazano ! Samaan Hind ! Kafr ! Kuku - Thoran Ein Eljaj ! As Safira Armanaz ! Haranbush ! Maaret Saidiyeh Kafr Zarbah ! Elekhwan Kafr - Kafr ! Aleppo Kafrehmul ! Azmarin Nabi ! Qanater Te ll e m ar ! ! ! ! Dweila Zardana AS-SAFIRA ! Mashehad Maaret Elnaasan ! Biret MAARET TAMSRIN - Maaret Ramadiyeh Elhaski Ghazala -! Armanaz ! ! Mgheidleh Maaret ! ARMANAZKuwaro - Shallakh Hafasraja ! Um Elriyah ! ! Tamsrin TEFTNAZ ! Zanbaqi ! Batenta ! ALEPPO Milis ! Kafraya Zahraa - Maar Dorriyeh Kherbet ! Ta m sa ri n Teftnaz Hadher Amud ! ! Darkosh Kabta Quneitra Kafr Jamiliya ! ! ! Jales Andnaniyeh Baliya Sheikh ! BENNSH Banan ! HADHER - Farjein Amud Thahr Yousef ! ! ! ! Ta lh i ye h ZARBAH Nasra DARKOSH Arshani -

Syria - Displacements from Northern Syria Production Date : 25/08/2016 IDP Locations - As of 16 August 2016
For Humanitarian Purposes Only Syria - Displacements from Northern Syria Production date : 25/08/2016 IDP Locations - As of 16 August 2016 Total number of IDPs: 749,275 BULBUL Raju " RAJU Shamarin Talil Elsham ² Krum Zayzafun - Ekdeh Gender & Age SHARAN Shmarekh Sharan Kafrshush Baraghideh " Tatiyeh Jdideh Maarin Ar-Ra'ee Salama AR-RA'EE " Nayara Ferziyeh A'ZAZ Azaz " Azaz Niddeh 19% MA'BTALI Sijraz Yahmul Maabatli Suran " Jarez " Kafr Kalbein 31% Maraanaz Girls under 18 Al-Malikeyyeh Kaljibrin AGHTRIN Afrin Manaq Akhtrein Boys under 18 " " Sheikh El-Hadid " Mare' Women " A'RIMA Tall Refaat 24% " Men Baselhaya TALL REFAAT AFRIN Deir Jmal MARE' Kafr Naseh Tal Refaat 26% Kafrnaya JANDAIRIS Jandairis " Nabul AL BAB " Al Bab " NABUL Tal Jbine Tadaf " Shelter Type Hayyan T U R K E Y Qah Atma Selwa Random gatherings HARITAN Andan Haritan TADAF Unfinished houses or Daret Azza " " buildings Reyhanli Kafr Bssin Other Qabtan Eljabal Tilaada Individual tents DARET AZZA A L E P P O Babis Deir Hassan - Darhashan Hur Maaret Elartiq Kafr Hamra Rented houses DANA Hezreh - Hezri Termanin Dana Anjara Foziyeh Harim " Bshantara RASM HARAM EL-IMAM Open areas " Tqad Majbineh Aleppo Antakya Ras Elhisn " Total Tlul Kafr Hum Ein Elbikara Aleppo HARIM Tuwama Hoteh Under trees Kafr Mu Tlul Big Hir Jamus QOURQEENA Tal Elkaramej Sahara JEBEL SAMAN Um Elamad Alsafira Besnaya - Bseineh Sarmada Oweijel Htan Tadil Collective center Ariba Qalb Lozeh Barisha Eastern Kwaires " Bozanti Kafr Deryan Kafr Karmin Abzemo Maaret Atarib Allani Radwa Kafr Taal Kafr Naha Home Kafr