Air Pollution & Its Health Effects in China
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chinese Cities of Opportunities 2018 Report
Beijing Harbin Lanzhou Jinan Wuhan Ningbo Guangzhou Kunming Shanghai Shenyang Xi’an Qingdao Wuxi Fuzhou Shenzhen Guiyang Tianjin Dalian Taiyuan Zhengzhou Suzhou Xiamen Zhuhai Chongqing Urumqi Shijiazhuang Nanjing Hangzhou Changsha Chengdu Chinese Cities of Opportunity 2018 Cities: Creating a beautiful life and new opportunities In modern society, cities are the most Changsha-Zhuzhou-Xiangtan Region, offers a comprehensive evaluation of the important spaces in which people can the Guanzhong Plain urban cluster, competitiveness, influence and potential pursue a better life. China has the Chengdu-Chongqing Economic Zone, of urban development to provide largest urban population in the world. In the central-southern of Liaoning and benchmarks for overall urban 2017, over 58% of China’s population, or Harbin-Changchun urban cluster. development, and has come to exert an more than 800 million people, lived in People gravitate toward areas with extensive influence in China. On the cities, and the urbanisation rate for economic opportunities and high quality basis of Chinese Cities of Opportunity residents is increasing by over one public services. Therefore, enhancing 2017, the number of sample cities percentage point every year. The the inclusiveness, balance and observed this year has increased to 30, advancement of urbanisation has sustainability of the development of and special attention has been given to pushed forward the intensive and urban clusters with large cities is a the development of national strategic efficient use of resources, promoted significant undertaking at the core of regions such as Guangdong-Hong innovation and enabled the economy to resolving “the principal contradiction Kong-Macau Greater Bay Area and prosper, while providing better basic between unbalanced and inadequate Xiong’an New Area. -

Appendix 1: Rank of China's 338 Prefecture-Level Cities
Appendix 1: Rank of China’s 338 Prefecture-Level Cities © The Author(s) 2018 149 Y. Zheng, K. Deng, State Failure and Distorted Urbanisation in Post-Mao’s China, 1993–2012, Palgrave Studies in Economic History, https://doi.org/10.1007/978-3-319-92168-6 150 First-tier cities (4) Beijing Shanghai Guangzhou Shenzhen First-tier cities-to-be (15) Chengdu Hangzhou Wuhan Nanjing Chongqing Tianjin Suzhou苏州 Appendix Rank 1: of China’s 338 Prefecture-Level Cities Xi’an Changsha Shenyang Qingdao Zhengzhou Dalian Dongguan Ningbo Second-tier cities (30) Xiamen Fuzhou福州 Wuxi Hefei Kunming Harbin Jinan Foshan Changchun Wenzhou Shijiazhuang Nanning Changzhou Quanzhou Nanchang Guiyang Taiyuan Jinhua Zhuhai Huizhou Xuzhou Yantai Jiaxing Nantong Urumqi Shaoxing Zhongshan Taizhou Lanzhou Haikou Third-tier cities (70) Weifang Baoding Zhenjiang Yangzhou Guilin Tangshan Sanya Huhehot Langfang Luoyang Weihai Yangcheng Linyi Jiangmen Taizhou Zhangzhou Handan Jining Wuhu Zibo Yinchuan Liuzhou Mianyang Zhanjiang Anshan Huzhou Shantou Nanping Ganzhou Daqing Yichang Baotou Xianyang Qinhuangdao Lianyungang Zhuzhou Putian Jilin Huai’an Zhaoqing Ningde Hengyang Dandong Lijiang Jieyang Sanming Zhoushan Xiaogan Qiqihar Jiujiang Longyan Cangzhou Fushun Xiangyang Shangrao Yingkou Bengbu Lishui Yueyang Qingyuan Jingzhou Taian Quzhou Panjin Dongying Nanyang Ma’anshan Nanchong Xining Yanbian prefecture Fourth-tier cities (90) Leshan Xiangtan Zunyi Suqian Xinxiang Xinyang Chuzhou Jinzhou Chaozhou Huanggang Kaifeng Deyang Dezhou Meizhou Ordos Xingtai Maoming Jingdezhen Shaoguan -

Air Polution Index (Api) Real Time Monitoring System
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by UTHM Institutional Repository AIR POLUTION INDEX (API) REAL TIME MONITORING SYSTEM NORHAFIZAH BINTI RUSLAN A thesis submitted in partial fulfilment of the requirements for the award of Degree of Master of Electrical Engineering Fakulti Kejuruteraan Elektrik Dan Elektronik Universiti Tun Hussein Onn Malaysia JANUARY 2015 ABSTRACT This project is to develop a low cost, mobile Air Pollutant Index (API) Monitoring System, which consists of Sharp GP2Y1010AU0F optical dust detector as a sensor for dust, Arduino Uno and LCD Keypad Shield. A signal conditioner has been used to amplify and extend the range of the sensor reading for a more accurate result. Readings from the sensor has been compared with reference data from the Department of Environment, Malaysia to ensure the results validity of the developed system. The developed dust detector is expected to provide a relatively accurate API reading and suitable to be used for the detection and monitoring of dust concentrations for industrial areas around Parit Raja, Johor. ABSTRAK Projek ini adalah untuk membangunkan alat mudah alih berkos rendah, Indeks Pencemaran mudah alih Udara (IPU) Sistem Pemantauan, yang terdiri daripada Sharp GP2Y1010AU0F pengesan debu optik sebagai sensor bagi habuk, Arduino Uno dan LCD Keypad Shield. Satu penyaman isyarat akan digunakan untuk menguatkan dan melanjutkan pelbagai bacaan sensor untuk keputusan yang lebih tepat. Bacaan dari sensor akan dibandingkan dengan data rujukan daripada Jabatan Alam Sekitar, Malaysia bagi memastikan kesahihan keputusan yang sistem yang dibangunkan. Pengesan debu dibangunkan dijangka menyelesaikan masalah-masalah projek ini dan sesuai digunakan untuk mengesan dan memantau kepekatan debu bagi kawasan perindustrian di seluruh Parit Raja, Johor. -

Long-Term Air Pollution Trend Analysis in Malaysia
Justin Sentian et al., Int. J. Environ. Impacts, Vol. 2, No. 4 (2019) 309–324 LONG-TERM AIR POLLUTION TREND ANALYSIS IN MALAYSIA JUSTIN SENTIAN, FRANKY HERMAN, CHAN YIT YIH AND JACKSON CHANG HIAN WUI Faculty of Science and Natural Resources, University Malaysia Sabah, Malaysia ABstract Air pollution has become increasingly significant in the last few decades as a major potential risk to public health in Malaysia due to rapid economic development, coupled with seasonal trans-boundary pollution. Over the years, air pollution in Malaysia has been characterised by large seasonal variations, which are significantly attributed to trans-boundary pollution. The aim of this study is to analyse the long-term temporal dynamic (1997–2015) of CO, NOx and PM10 at 20 monitoring stations across Ma- laysia. Long-term pollutant trends were analysed using the Mann–Kendall test. For potential pollutant source analysis, satellite data and Hybrid Single-Particle Lagrangian Integrated Trajectory (HYSPLIT) backward trajectories model were employed. In all monitoring sites, we observed that the annual aver- age concentrations of PM10 were varied, with large coefficient variations. Meanwhile, CO and NOx were found to be less varied, with smaller coefficient variations, except in certain monitoring sites. Long-term analysis trends for CO attested to insignificant decreasing trends in 11 monitoring stations and increasing trends in seven stations. Meanwhile, NOx showed no significant trends in most sta- tions. For PM10, five monitoring stations showed increasing trends, whereas 15 other stations showed decreasing trends. HYSPLIT backward trajectory analyses have shown that high seasonal PM10 levels in most parts of Malaysia are due to trans-boundary pollution. -

Ancient Genomes Reveal Tropical Bovid Species in the Tibetan Plateau Contributed to the Prevalence of Hunting Game Until the Late Neolithic
Ancient genomes reveal tropical bovid species in the Tibetan Plateau contributed to the prevalence of hunting game until the late Neolithic Ningbo Chena,b,1, Lele Renc,1, Linyao Dud,1, Jiawen Houb,1, Victoria E. Mulline, Duo Wud, Xueye Zhaof, Chunmei Lia,g, Jiahui Huanga,h, Xuebin Qia,g, Marco Rosario Capodiferroi, Alessandro Achillii, Chuzhao Leib, Fahu Chenj, Bing Sua,g,2, Guanghui Dongd,j,2, and Xiaoming Zhanga,g,2 aState Key Laboratory of Genetic Resources and Evolution, Kunming Institute of Zoology, Chinese Academy of Sciences (CAS), 650223 Kunming, China; bKey Laboratory of Animal Genetics, Breeding and Reproduction of Shaanxi Province, College of Animal Science and Technology, Northwest A&F University, 712100 Yangling, China; cSchool of History and Culture, Lanzhou University, 730000 Lanzhou, China; dCollege of Earth and Environmental Sciences, Lanzhou University, 730000 Lanzhou, China; eDepartment of Earth Sciences, Natural History Museum, London SW7 5BD, United Kingdom; fGansu Provincial Institute of Cultural Relics and Archaeology, 730000 Lanzhou, China; gCenter for Excellence in Animal Evolution and Genetics, Chinese Academy of Sciences, 650223 Kunming, China; hKunming College of Life Science, University of Chinese Academy of Sciences, 100049 Beijing, China; iDipartimento di Biologia e Biotecnologie “L. Spallanzani,” Università di Pavia, 27100 Pavia, Italy; and jCAS Center for Excellence in Tibetan Plateau Earth Sciences, Institute of Tibetan Plateau Research, Chinese Academy of Sciences, 100101 Beijing, China Edited by Zhonghe Zhou, Chinese Academy of Sciences, Beijing, China, and approved September 11, 2020 (received for review June 7, 2020) Local wild bovids have been determined to be important prey on and 3,000 m a.s.l. -

1 China Xi'an-Ankang Railway Construction Project
China Xi’an-Ankang Railway Construction Project (1)-(3) (CXVII-P73, CXVIII-P73, CXIX-P73) External Evaluator: Mitsue Mishima (OPMAC) Field Survey: October 2004 1. Project Profile and Japan’s ODA Loan Mongolia Beijing North Korea China South Korea Project site Xian Nepal Ankang Bhutan India Taiwan Myanmar Vietnam Laos Project site location map (Xian-Ankang, Shannxi Province) Qingcha Tunnel 1.1 Background The project site (Xian- Ankang) is located in the southern part of Shaanxi Province where the 3000-meter high Qinling Mountains extend over 1500 kilometers, and was therefore undeveloped due to difficulties in transportation and remoteness from cities. Southwest of the project site is Sichuan Province, the largest province with a population of 110 million accounting for 10% of the population of China. However, as there is no other transport route to Sichuan Province than taking a detour around the Qinling Mountains, there were only limited routes to transport energy and everyday commodities from the north. Railway transport from other regions to Sichuan Province depended on Baoching Line (Baoji-Chengdu) from the north and Xiangyu Line (Xiangfan-Ankang-Chongquing) from the east, and both lines were operating to full capacity. It was particularly difficult to double-track Baoching Line, which takes a detour to avoid the Qinling Mountains because of 1) long distance of transport, 2) large cost to transport on a gradient at an angel of 3%, and 3) the topographical problem. The opening of the electrified single track of Xian-Ankang Line not only helped increase the transport capacity within Shaanxi Province but also shortened the traveling distance to Chongquing and eased the transportation load on Baoching Line. -
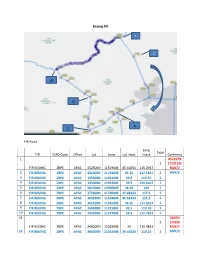
Shanghai FIR
Beijing FIR 1 2 19 15 8 11 FIR Point Long Type FIR ICAO Code Office Lat Long Lat Input Input Comment 1 452317N 1 1152115E FIR BEIJING ZBPE APAC 452500N 1151900E 45.40054 115.2947 RAN/2 2 FIR BEIJING ZBPE APAC 431500N 1173100E 43.25 117.5167 1 RAN/2 3 FIR BEIJING ZBPE APAC 395400N 1192100E 39.9 119.35 1 4 FIR BEIJING ZBPE APAC 393000N 1195200E 39.5 119.8667 1 5 FIR BEIJING ZBPE APAC 381500N 1200000E 38.25 120 1 6 FIR BEIJING ZBPE APAC 372900N 1173000E 37.48333 117.5 1 7 FIR BEIJING ZBPE APAC 363200N 1151800E 36.53333 115.3 1 8 FIR BEIJING ZBPE APAC 362100N 1145500E 36.35 114.9167 1 9 FIR BEIJING ZBPE APAC 360600N 1142100E 36.1 114.35 1 10 FIR BEIJING ZBPE APAC 345400N 1124700E 34.9 112.7833 1 11 3405N 1 11029E FIR BEIJING ZBPE APAC 340000N 1102900E 34 110.4833 RAN/2 12 FIR BEIJING ZBPE APAC 343200N 1101500E 34.53333 110.25 1 RAN/2 13 FIR BEIJING ZBPE APAC 353200N 1101800E 35.53333 110.3 1 14 FIR BEIJING ZBPE APAC 372800N 1104400E 37.46667 110.7333 1 15 FIR BEIJING ZBPE APAC 382200N 1103600E 38.36666 110.6 1 16 FIR BEIJING ZBPE APAC 384400N 1094100E 38.73333 109.6833 1 17 FIR BEIJING ZBPE APAC 402000N 1070100E 40.33333 107.0167 1 18 FIR BEIJING ZBPE APAC 404300N 1055500E 40.71667 105.9167 1 19 414451N 1 1051345E FIR BEIJING ZBPE APAC 414400N 1051300E 41.74361 105.218 RAN/2 Along political boundary to (1) Note: 1. -

Holocene Environmental Archaeology of the Yangtze River Valley in China: a Review
land Review Holocene Environmental Archaeology of the Yangtze River Valley in China: A Review Li Wu 1,2,*, Shuguang Lu 1, Cheng Zhu 3, Chunmei Ma 3, Xiaoling Sun 1, Xiaoxue Li 1, Chenchen Li 1 and Qingchun Guo 4 1 Provincial Key Laboratory of Earth Surface Processes and Regional Response in the Yangtze-Huaihe River Basin, School of Geography and Tourism, Anhui Normal University, Wuhu 241002, China; [email protected] (S.L.); [email protected] (X.S.); [email protected] (X.L.); [email protected] (C.L.) 2 State Key Laboratory of Loess and Quaternary Geology, Institute of Earth Environment, Chinese Academy of Sciences, Xi’an 710061, China 3 School of Geograpy and Ocean Science, Nanjing University, Nanjing 210023, China; [email protected] (C.Z.); [email protected] (C.M.) 4 School of Environment and Planning, Liaocheng University, Liaocheng 252000, China; [email protected] * Correspondence: [email protected] Abstract: The Yangtze River Valley is an important economic region and one of the cradles of human civilization. It is also the site of frequent floods, droughts, and other natural disasters. Conducting Holocene environmental archaeology research in this region is of great importance when studying the evolution of the relationship between humans and the environment and the interactive effects humans had on the environment from 10.0 to 3.0 ka BP, for which no written records exist. This Citation: Wu, L.; Lu, S.; Zhu, C.; review provides a comprehensive summary of materials that have been published over the past Ma, C.; Sun, X.; Li, X.; Li, C.; Guo, Q. -

Shengjing Bank Co., Ltd.* (A Joint Stock Company Incorporated in the People's Republic of China with Limited Liability) Stock Code: 02066 Annual Report Contents
Shengjing Bank Co., Ltd.* (A joint stock company incorporated in the People's Republic of China with limited liability) Stock Code: 02066 Annual Report Contents 1. Company Information 2 8. Directors, Supervisors, Senior 68 2. Financial Highlights 4 Management and Employees 3. Chairman’s Statement 7 9. Corporate Governance Report 86 4. Honours and Awards 8 10. Report of the Board of Directors 113 5. Management Discussion and 9 11. Report of the Board of Supervisors 121 Analysis 12. Social Responsibility Report 124 5.1 Environment and Prospects 9 13. Internal Control 126 5.2 Development Strategies 10 14. Independent Auditor’s Report 128 5.3 Business Review 11 15. Financial Statements 139 5.4 Financial Review 13 16. Notes to the Financial Statements 147 5.5 Business Overview 43 17. Unaudited Supplementary 301 5.6 Risk Management 50 Financial Information 6. Significant Events 58 18. Organisational Chart 305 7. Change in Share Capital and 60 19. The Statistical Statements of All 306 Shareholders Operating Institution of Shengjing Bank 20. Definition 319 * Shengjing Bank Co., Ltd. is not an authorised institution within the meaning of the Banking Ordinance (Chapter 155 of the Laws of Hong Kong), not subject to the supervision of the Hong Kong Monetary Authority, and not authorised to carry on banking and/or deposit-taking business in Hong Kong. COMPANY INFORMATION Legal Name in Chinese 盛京銀行股份有限公司 Abbreviation in Chinese 盛京銀行 Legal Name in English Shengjing Bank Co., Ltd. Abbreviation in English SHENGJING BANK Legal Representative ZHANG Qiyang Authorised Representatives ZHANG Qiyang and ZHOU Zhi Secretary to the Board of Directors ZHOU Zhi Joint Company Secretaries ZHOU Zhi and KWONG Yin Ping, Yvonne Registered and Business Address No. -

Table of Codes for Each Court of Each Level
Table of Codes for Each Court of Each Level Corresponding Type Chinese Court Region Court Name Administrative Name Code Code Area Supreme People’s Court 最高人民法院 最高法 Higher People's Court of 北京市高级人民 Beijing 京 110000 1 Beijing Municipality 法院 Municipality No. 1 Intermediate People's 北京市第一中级 京 01 2 Court of Beijing Municipality 人民法院 Shijingshan Shijingshan District People’s 北京市石景山区 京 0107 110107 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Haidian District of Haidian District People’s 北京市海淀区人 京 0108 110108 Beijing 1 Court of Beijing Municipality 民法院 Municipality Mentougou Mentougou District People’s 北京市门头沟区 京 0109 110109 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Changping Changping District People’s 北京市昌平区人 京 0114 110114 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Yanqing County People’s 延庆县人民法院 京 0229 110229 Yanqing County 1 Court No. 2 Intermediate People's 北京市第二中级 京 02 2 Court of Beijing Municipality 人民法院 Dongcheng Dongcheng District People’s 北京市东城区人 京 0101 110101 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Xicheng District Xicheng District People’s 北京市西城区人 京 0102 110102 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Fengtai District of Fengtai District People’s 北京市丰台区人 京 0106 110106 Beijing 1 Court of Beijing Municipality 民法院 Municipality 1 Fangshan District Fangshan District People’s 北京市房山区人 京 0111 110111 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Daxing District of Daxing District People’s 北京市大兴区人 京 0115 -

Analysis of the Spatial and Temporal Variation Characteristics of Ozone in the Pearl River Delta Region from 2016 to 2020
E3S Web of Conferences 245, 02025 (2021) https://doi.org/10.1051/e3sconf/202124502025 AEECS 2021 Analysis of the Spatial and Temporal Variation Characteristics of Ozone in the Pearl River Delta Region from 2016 to 2020 Huang Chuntao 1*, Lu Jifu 1, Liao Qifeng 2 1 Huali College, Guangdong University of Technology, Guangzhou, Guangdong, 511300 2 Guangdong Kedilong Technology Co., Ltd, Guangzhou, Guangdong, 510000 Abstract: Based on the historical data of air ozone monitoring of Pearl River Delta from 2016 to 2020, the temporal and spatial variation characteristics of ozone in the Pearl River Delta were analyzed. The results showed that the mean change curves of Q3 in the seven cities in the Pearl River Delta region from 2016 to 2020 were M-shaped, and the change trend was basically the same, except Huizhou and Zhuhai. The over standard rate of daily mean value of Q3 in Jiangmen City from 2016 to 2020 was more than 10%, and the over standard situation of daily mean value of Q3 was serious. In the Pearl River Delta region, the change trend of the monthly mean value of Q3 in the same year was basically the same. On the whole, the mean value from August to November was higher, and the mean value in June was lower. The peak of Q3 concentration appeared between 12:00 and 16:00 in the daytime, and it was generally low at night. 1 Preface studies on the spatial and temporal distribution characteristics of Q3 in the Pearl River Delta in recent Ozone (Q3) is an important component of the atmosphere, years. -
Report. There Are Six AQI Categories, Namely Good, Satisfactory, Moderately Polluted, Poor, Very Poor, and Severe
Control of Urban Pollution Series: CUPS/ 82 /2014-15 NATIONAL AIR QUALITY INDEX Pl\nto AQI: 95; Satisfactory Responsible Pollutant: P M "tilks CLEAN Wg/ CENTRAL POLLUTION CONTROL BOARD Ministry of Environment, Forests & Climate Change Website: www.cpcb.nic.in 7rfvr AT.A.14. Wzr Frfaa s SHASHI SHEKHAR, IAS i 1c'Ic1I 4 to41 Special Secretary -14 - 110003 GOVERNMENT OF INDIA MEZIF MINISTRY OF ENVIRONMENT, FOREST & ITTUT -11A41 CLIMATE CHANGE Chairman NEW DELHI-110003 CENTRAL POLLUTION CONTROL BOARD Foreword Air pollution levels in most of the urban areas have been a matter of serious concern. It is the right of the people to know the quality of air they breathe. However, the data generated through National Ambient Air Monitoring Network are reported in the form that may not be easily understood by a common person, and therefore, present system of air quality information does not facilitate people's participation in air quality improvement efforts. In view of this, CPCB took initiative for developing a national Air Quality Index (AQI) for Indian cities. AQI is a tool to disseminate information on air quality in qualitative terms (e.g. good, satisfactory, poor) as well as its associated likely health impacts. An Expert Group comprising medical professionals, air quality experts, academia, NGOs, and SPCBs developed National AQI. Necessary technical information was provided by IIT Kanpur. The draft AQI was launched in October 2014 for seeking public comments. It was also circulated to States Governments, Pollution Control Boards, concerned Central Government Ministries and premier research institutes for inputs. Comments received were examined by the Expert Group and a National AQI scheme was finalized, which is presented in this report.