ISPI, for Administration Support
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Draft Inverclyde Antisocial Behaviour Strategy 2020-2025
Draft Inverclyde Antisocial Behaviour Strategy 2020-2025 Draft Inverclyde Antisocial Behaviour Strategy 2020-2025 Inverclyde Community Safety Partnership 1 | P a g e Draft Inverclyde Antisocial Behaviour Strategy 2020-2025 Contents Page Foreword 3 Section One- Introduction 4 Section Two- Context 5 Section Three- Strategic Themes 7 Section Four- Assessment of Antisocial Behaviour in Inverclyde 9 Section Five: Community Engagement 11 Section Six: Resources and Services 11 Section Seven: Support for Victims of Antisocial Behaviour 12 Section Eight: The Provision of Mediation Services 12 Section Nine: Information Sharing 12 Section Ten: Review of the Strategy 13 Appendix One: Associated Strategies, Plans and Policies 14 2 | P a g e Draft Inverclyde Antisocial Behaviour Strategy 2020-2025 Joint Foreword Although the Antisocial Behaviour etc. (Scotland) Act 2004 requires the Local Authority and Chief Constable of Police Scotland to produce a strategy for dealing with antisocial behaviour this strategy has been endorsed by the Inverclyde Alliance Board and the Inverclyde Community Safety Partnership highlighting the breadth of partners in Inverclyde who respond to antisocial behaviour in Inverclyde. This strategy sets out the several legislative requirements of the Antisocial Behaviour etc. (Scotland) Act 2004 which is detailed below. In addition to this the Community Safety Partnership will also produce an Antisocial Behaviour Policy document, which sets out in more detail, how agencies will respond to antisocial behaviour in Inverclyde. Whilst overall incidents of antisocial behaviour reported to both Inverclyde Council and Police Scotland have reduced over the previous three years, partners do acknowledge that antisocial behaviour can have a serious impact on the lives of our residents and have a negative impact on communities across Inverclyde. -

BCS Paper 2017/74 2018 Review of UK Parliament Constituencies Draft
Boundary Commission for Scotland BCS Paper 2017/74 2018 Review of UK Parliament Constituencies Draft Revised Proposals for Argyll and Bute, Highland and Moray council areas Action required 1. The Commission is invited to consider responses to the initial and secondary consultation on its Initial Proposals and whether it wishes to make changes to its proposals for Argyll and Bute, Highland and Moray council areas. Background 2. These constituency designs are based on a UK electoral quota of 74,769.2 electors and parliamentary electorate figures from the December 2015 Electoral Register. The electorate of constituencies has to be within 5% of the electoral quota, namely no fewer than 71,031 and no more than 78,507, unless the area of a constituency exceeds 12,000 square kilometres. No constituency may exceed 13,000 square kilometres. 3. The total electorate in the 3 council areas is 307,418, giving a theoretical entitlement to 4.11 constituencies. It is possible, therefore, to design 4 constituencies, exactly covering the combined council areas, the electorates of which are within the limits set by the legislation. 4. The Commission's Initial Proposals for this area comprise 4 constituencies which exactly cover the combined extent of these 3 council areas. A map of the constituencies is at Appendix A. Wards Difference Constituency Council areas Area (km2) Electorate (2007–2017) from EQ Argyll, Bute and Argyll and Bute All 10,302 77,574 3.8% Lochaber Highland 12(part),22 Highland Highland 1-5,6(part),7-10,13(part) 12,985 73,147 -2.2% North Inverness 6(part),11,12(part),13(part),14- Highland 9,995 78,220 4.6% and Skye 18,20,21 Moray Moray All 2,612 78,477 5.0% and Nairn Highland 19 Table 1. -

65 the Relationship Between Output and Unemployment in Scotland: a Regional Analysis
LAND ECONOMY WORKING PAPER SERIES ___________________________________________________________________ Number: 65 The relationship between output and unemployment in Scotland: A regional analysis Corresponding Author: Cesar Revoredo-Giha Land Economy Research Group SAC Research Division SAC Edinburgh EH9 3JG Tel: 0131-535-4344 Email: [email protected] THE RELATIONSHIP BETWEEN OUTPUT AND UNEMPLOYMENT IN SCOTLAND: A REGIONAL ANALYSIS Cesar Revoredo-Giha, Philip Leat and Alan Renwick ABSTRACT The relationship between unemployment and growth (i.e., the so-called Okun’s Law) has long standing in macroeconomics and regional economics. In this paper we estimate such a relationship for Scotland and at the Nomenclature of Territorial Units for Statistics (NUTS) level 3 regions using a panel dataset. The main motivations behind this interest are twofold: first, to test whether such a relationship exists in Scotland and how different these estimates are from those produced for the UK. Second, whether there exist regional differences in the estimates. The latter is particularly important in the context of the current budgetary cuts, which may affect both GDP growth and unemployment in different ways rural and urban areas. Results indicate that the Okun’s coefficient for Scotland is slightly higher than the one computed for the UK (1.7 Scotland versus 1.39 and 1.45 for the UK), and although an Okun relationship seemed to be valid for most of the regions, there were no statistical differences between rural and urban areas. However, as regards the effect of economic growth on unemployment, the results indicate a different and stronger effect in urban areas than in rural areas. -
Ref: SL/AI Date: 10 February 2021 a Meeting of the Inverclyde Council Will Be Held on Thursday 18 February 2021 at 4Pm. This
Municipal Buildings, Greenock PA15 1LY Ref: SL/AI Date: 10 February 2021 A meeting of the Inverclyde Council will be held on Thursday 18 February 2021 at 4pm. This meeting is by remote online access only through the videoconferencing facilities which are available to Members and relevant Officers. The joining details will be sent to Members and Officers prior to the meeting. In the event of connectivity issues, Members are asked to use the join by phone number in the Webex invitation. Please note that this meeting will be recorded. GERARD MALONE Head of Legal and Property Services BUSINESS **Copy to follow 1. Apologies and Declarations of Interest Page NEW BUSINESS 2. Minutes of Meetings of The Inverclyde Council, Committees, Sub-Committees and Boards Appointment Panel – Head of Legal Services ( p 225) Inverclyde Council (pp 226 – 233) General Purposes Board ( p 234) Environment & Regeneration Committee (Special) (pp 235 – 237) Appointment Panel – Head of Legal Services ( p 238) Planning Board (pp 1 – 3) Policy & Resources Committee (Special) (pp 4 – 5) Health & Social Care Committee (pp 6 – 9) Audit Committee ( p 10) Environment & Regeneration Committee (pp 11 – 19) Education & Communities Committee (pp 20 – 21) Human Resources Appeals Board ( p 22) Policy & Resources Committee (pp 23 – 24) ** Planning Board (pp 25 – ) ** Local Police & Fire Scrutiny Committee ( ) ** General Purposes Board ( ) 00 Ag - IC - 18 02 2021 3. Budget Update and Approval of the 2021/22 Band D Council Tax Report by Chief Financial Officer p 4. Resolution: Setting of Band D Council Tax for 2021/22 5. Strathclyde Pension Fund – Notice of Motion by Councillor J McEleny Report by Corporate Director Environment, Regeneration & Resources p 6. -

Publication 2008
COMMISSIONED REPORT Commissioned Report No.291 Public Perceptions of Wild Places and Landscapes in Scotland (ROAME No. F06NC03) For further information on this report please contact: James Fenton Scottish Natural Heritage Great Glen House INVERNESS IV3 8NW Telephone: 01463-725 318 E-mail: [email protected] This report should be quoted as: Market Research Partners, Edinburgh. (2008). Public Perceptions of Wild Places and Landscapes in Scotland. Commissioned Report No.291(ROAME No. F06NC03). This report, or any part of it, should not be reproduced without the permission of Scottish Natural Heritage. This permission will not be withheld unreasonably. The views expressed by the author(s) of this report should not be taken as the views and policies of Scottish Natural Heritage. © Scottish Natural Heritage 2008. COMMISSIONED REPORT Summary Public Perceptions of Wild Places and Landscapes in Scotland Commissioned Report No. 291(ROAME No. F06NC03) Contractor: Market Research Partners, Edinburgh Year of publication: 2008 Background Currently, there is little quantitative evidence of consumer opinion regarding the ‘wildness’ of Scotland. Therefore Scottish Natural Heritage and the Cairngorms National Park Authority commissioned a market research study to evaluate public perceptions of wild places amongst a representative cross-section of Scottish residents and a subset amongst those living within the boundaries of the Cairngorms National Park (CNP). The study identifies the level of support for wild places and whether the views of those who live within CNP match the population of Scotland as a whole. A total of 1,304 face to face interviews were conducted (1,004 across Scotland and 300 with residents of the CNP). -

Argyll and Bute Council
APPENDIX 1 PROPOSED KILPATRICK HILLS LOCAL LANDSCAPE AREA – DRAFT STATEMENT OF IMPORTANCE September 2013 Contents 1. Introduction 2. Policy context 3. Background and study approach 4. Statement of Importance 4.1 Overview 4.2 Landscape Description 4.3 Proposed Local Landscape Area boundary 4.4 Landscape change 4.5 Other designations and interests 1. INTRODUCTION The Kilpatrick Hills are a range of hills north of the River Clyde stretching from Dumbarton and the Vale of Leven in the west to Strathblane in the east. The rugged upland landscape provides a stunning backdrop to the settlements which fringe them, including Balloch, Dumbarton, Bowling, Old Kilpatrick, Clydebank, Bearsden and Milngavie, creating a unique sense of place. To the north of the hills lies the Loch Lomond and the Trossachs National Park. The majority of the range is within West Dunbartonshire, although it extends into East Dunbartonshire and Stirling. In addition to the Kilpatrick Hills’ special landscape qualities, the area is home to an important habitat network and provides recreational opportunities for local communities. West Dunbartonshire Council and East Dunbartonshire Council propose to designate the Kilpatrick Hills as a Local Landscape Area (LLA) in their respective Local Development Plans. This document explains the reasons why the Kilpatrick Hills have been selected for this designation. It will provide the basis for Supplementary Guidance for the Kilpatrick Hills which will establish a framework for managing change and the protection and enhancement of the area’s special qualities. Figure 1 – The location of the Kilpatrick Hills within central Scotland 2 2. POLICY CONTEXT Scotland’s landscapes are recognised as a major asset, contributing to national, regional and local identities, adding to the quality of many people’s lives and providing attractive settings which help to promote social and economic development. -

Electoral Review of Island Council Areas
Agenda 14 Item Report HC/18/19 No The Highland Council Date: 9 May, 2019 Report title: Electoral Review of Island Council Areas Report by: The Chief Executive Purpose/Executive Summary The purpose of this report is to provide the Council with an overview of the provisions of the Islands (Scotland) Act 2018 that relate to the requirement for the Local Government Boundary Commission for Scotland to review the electoral arrangements for Argyll and Bute Council, Comhairle Nan Eilean Siar, Highland Council, North Ayrshire Council, Orkney Islands Council and Shetland Islands Council. 1. Recommendations 1.1 Council is invited to • Agree that the Chief Executive write to the Local Government Boundary Commission seeking a meeting to explore the possibility of the Commission broadening the scope of their current review to include rural wards of super sparsity. • Agree that the Council write to the Cabinet Secretary for Communities and Local Government to highlight issues around the methodology used in boundary reviews and to make the case for additional flexibility over the number of members for rural wards. 2. Background 2.1 The Local Government Boundary Commission for Scotland and the Scottish Ministers are obliged, under section 28(2) of the Local Government (Scotland) Act 1973 to implement electoral arrangements in accordance with section 1 of the Local Governance (Scotland) Act 2004. Currently this includes the requirement for there to be three or four councillors returned per electoral ward in Scotland. 2.2 The Islands (Scotland) Act 2018 amends the 2004 Act to provide an exception to the usual three or four member rule for electoral wards in relation to wards which consist either wholly or partly of one or more inhabited islands. -

Alcohol Outlet Availability and Harm in Argyll and Bute April 2018
Alcohol Outlet Availability and Harm in Argyll and Bute April 2018 This document sets out the findings from research by Alcohol Focus Scotland (AFS) and the Centre for Research on Environment, Society and Health (CRESH), which investigated whether alcohol-related health harm (hospitalisations and deaths) and crime rates across Scotland were related to the local availability of alcohol outlets. The relationship between income deprivation and alcohol outlet availability was also examined. Contents Introduction ............................................................................................................................................. 2 Alcohol Outlet Availability in Argyll and Bute ............................................................................................ 2 Alcohol-Related Health Harm and Crime in Argyll and Bute ....................................................................... 4 Alcohol-Related Death Rates and Alcohol Outlet Availability ..................................................................... 5 Alcohol-Related Hospitalisation Rates and Alcohol Outlet Availability ....................................................... 5 Crime Rates and Alcohol Outlet Availability .............................................................................................. 5 Income Deprivation and Alcohol Outlet Availability ................................................................................... 6 Interpreting the Findings ......................................................................................................................... -
Argyll and Bute SDS Local Authority
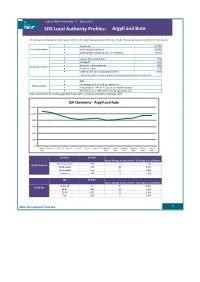
Labour Market Information | March 2016 Argyll and Bute SDS Local Authority Profiles: All Jobseekers Allowance (JSA) figures refer to the latest data available (February 2016). Please see notes at end for further details. Population 87,700 Local Information . Working Age Population 53,000 . Working Age Population as % of Population 60.4% . Overall Employment Rate 76% . Disabled* 51% . Ethnicity - ethnic minority 48% Employment Rates . Ethnicity - white 76% . Over 50 (N.B. 50+ as opposed to 50-64) 40% ! Estimate and confidence interval not available since the group sample size is zero or disclosive (0-2). 953 . An increase of 3, or 0.3% on last month JSA Claimants . A decrease of -124, or -11.5% on this month last year . The JSA count is 1.8% of the working age population Note: Denominator for working age (16-64) population is mid-year population estimates, 2014 JSA Claimants - Argyll and Bute 1,200 1,000 800 600 400 200 0 February March 2015 April 2015 May 2015 June 2015 July 2015 August 2015 September October November December January February 2015 2015 2015 2015 2015 2016 2016 Duration Number Actual Change on Last month % Change on Last Month 13 weeks or less 395 -5 -1.3% JSA By Duration 13-26 weeks 170 15 9.7% 26-52 weeks 135 0 0.0% 52 weeks + 240 -5 -2.0% Age Number Actual Change on Last month % Change on Last Month Under 18 5 5 0.0% JSA By Age 18-24 185 -10 -5.1% 25-49 475 15 3.3% 50+ 280 0 0.0% Skills Development Scotland 1 JSA by Age and Duration - Argyll and Bute 450 400 350 300 250 50+ 200 25-49 150 18-24 100 Under 18 50 0 Claiming up to Claiming 13-26wks Claiming 26-52wks Claiming 52-78wks Claiming 78-104wks Claiming over 13wks 104wks Duration of Claimant Count . -

Renewable Energy
Foreword LOCAL DEVELOPMENT PLAN 2ARGYLL AND BUTE COUNCIL i Argyll and Bute is an incredibly diverse area with an outstanding natural environment, more inhabited islands than any other council in Scotland, miles of amazing coastline, small communities in remote rural areas and larger towns close to the central belt. The area is the second largest council area in Scotland and home to numerous award-winning businesses and services. The scale and diversity of our region presents great opportunities as well as major challenges in planning for the future development of the area. The Local Development Plan 2 plays a key role in promoting a successful future for Argyll and Bute by helping to deliver a prosperous and inclusive economy, safeguarding our environmental assets and planning for the future growth of our communities. In this time of economic uncertainty and faced with the challenges presented by climate change and a falling population, it is increasingly important for us to work together to achieve our shared objectives. Accordingly, the Proposed Local Development Plan 2 contains a strategy that is closely aligned to the Single Outcome Improvement Plan and with other key plans for the area. It sets out a land use framework for the next 10 years to promote, guide and manage development in Argyll and Bute. It also aims to support the delivery of new homes, create new employment opportunities and protect our natural and built environment through a suite of policies, proposals and deliverable development sites. The Proposed Local Development Plan 2 has been drawn up following a comprehensive engagement process with communities, developers, key government agencies and other stakeholders. -

Publication Scheme
Glasgow City Region City Deal Guide to Information Available City Deal Publication Scheme The Freedom of Information (Scotland) Act 2002 (the Act) requires Scottish public authorities to produce and maintain a publication scheme. Authorities are under a legal obligation to: • publish the classes of information that they make routinely available • tell the public how to access the information and what it might cost. To comply with their obligations, the eight Member Authorities involved in the City Deal, including Glasgow City Council as lead authority, have each signed up to the Model Publication Scheme 2013 produced by the Scottish Information Commissioner. This scheme can be found on the Scottish Information Commissioner’s website: http://www.itspublicknowledge.info/ScottishPublicAuthorities/PublicationSchemes/PublicationSchemeResources.aspx Whilst each Model Publication Scheme applies to all information published by each Member Authority, this Guide to Information relates specifically and only to information held by Glasgow City Council as Lead Authority in relation to the City Deal. The purpose of this Guide is to: • allow the public to see what information is available (and what is not available) in relation to the Glasgow City Region City Deal • state what charges may be applied • explain how to find the information easily • provide contact details for enquiries and to get help with accessing the information • explain how to request information we hold that has not been published Although we are not under a statutory obligation to publish a separate Publication Scheme for the City Deal, we have chosen to do so in order to demonstrate our commitment to transparency and accountability, and to make it as convenient as possible for City Deal information to be located. -

Environmental & Regulatory Services
Environmental & regulatory services Performance Indicators 2002/03 Comparing the performance of Scottish councils Prepared for the Accounts Commission February 2004 The Accounts Commission The Accounts Commission is a statutory, independent body, which through, the audit process, assists local authorities in Scotland to achieve the highest standards of financial stewardship and the economic, efficient and effective use of their resources. The Commission has five main responsibilities: • securing the external audit • following up issues of concern identified through the audit, to ensure satisfactory resolutions • reviewing the management arrangements which audited bodies have in place to achieve value for money • carrying out national value for money studies to improve economy, efficiency and effectiveness in local government • issuing an annual direction to local authorities which sets out the range of performance information which they are required to publish. The Commission secures the audit of 32 councils and 35 joint boards (including police and fire services). Local authorities spend over £9 billion of public funds a year. Audit Scotland is a statutory body set up in April 2000 under the Public Finance and Accountability (Scotland) Act 2000. It provides services to the Accounts Commission and the Auditor General for Scotland.Together they ensure that the Scottish Executive and public sector bodies in Scotland are held to account for the proper, efficient and effective use of public funds. 1 Main findings Methods of waste disposal Indicator 1 Page 4 Almost 88% of household, commercial and industrial waste was used for landfill. Councils recycled 9.6% of all waste in 2002/03, an increase compared with the previous year (7.4%).