Health Information Technology Platform
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

121012 Tech Legend Sees Soma Oakland SFBT
Tech legend sees SoMa - in Oakland October 12, 2012 By Blanca Torres Mitch Kapor and Freada Kapor Klein are investing in Oakland’s future. When famed technology titan and philanthropist Mitch Kapor looks at Oakland, he remembers South of Market in San Francisco the way it was in the late 1990s. Former industrial properties were being transformed into inexpensive spaces for both startup tech companies and residents. There was a buzz of innovation in the air. SoMa today is not the same place Kapor remembers, but Oakland could be. “Oakland in particular is the next great South of Market,” Kapor said. “It will be to this decade what South of Market was to the previous one. There’s lots of space, both to work and to live, lots of energy and lots of opportunity. People just sense potential.” With that belief in mind, Kapor and his wife, Freada Kapor Klein, moved the operations of Kapor Capital, Kapor Enterprises Inc., the Kapor Foundation and Level Playing Field Institute, a nonprofit, to Oakland’s Uptown neighborhood from a previous location in SoMa. Kapor made his name and fortune from Lotus Development Corp., maker of the Lotus 1-2-3 spreadsheet and Lotus Notes software applications. The Kapors, along with Oakland business and community leaders, see the move as much more than just physical. It could serve as a major endorsement for Oakland’s technology sector, which so far features a handful of big names — Pandora Media, Ask.com and Sungevity — but has yet to detonate. “Oakland is a welcoming environment for innovators and for people who cross boundaries because we’re not just doing tech, we’re doing tech with social impact,” Kapor said. -

Cyberspace and the "Devil's Hatband"
ARTICLE Cyberspace and the "Devil's Hatband" JonathanJ. Rusch* INTRODUCTION "I cannot remember a time," the novelist Robertson Davies wrote, "when I did not take it as understood that everybody has at least two, if not twenty-two, sides to him."' Davies' comment gives us a convenient point of departure to explore the relationship between law and cyberspace. Anyone who spends a significant amount of time on the Internet knows that the Net has at least two, if not twenty-two, sides to it. Auction sites, chat rooms, instant messaging, knowledge networks, and Net radio are but a few of the Internet's constantly expanding capabilities for communication, commerce, and social interaction. It seems remarkable, then, that at a time when we are seeking to understand and enhance a medium of such Protean charac- ter, so much of our thinking about the Internet has remained bound to-and bounded by-the same few metaphors that have dominated Internet culture over the past decade. No metaphor has been more pervasive in this regard than the concept of cyberspace as the "Wild West." Early visionaries of the Internet characterized it as an "electronic frontier, "2' comparing its * Special Counsel for Fraud Prevention, Fraud Section, Criminal Division, U.S. Depart- ment of Justice; Adjunct Professor, Georgetown University Law Center. This Article is a substantial revision and expansion of a presentation I gave on April 1, 2000, at the Seattle University School of Law's Internet Law Institute. The views in this Article are solely those of the author and not necessarily those of the Department of Justice or any officer or component thereof. -
Computing the Cost of Copyright */ Programmers Fight 4Look and Feel' Lawsuits
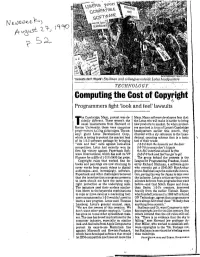
l<L^r^- RICK FRIEDMAN-BLACK STAR Innovate don't litigate': Stallman and colleagues outside Lotus headquarters :••' •• ' .' TECHNOLOGY/' ;.:::'; : ' Computing the Cost of Copyright */ Programmers fight 4look and feel' lawsuits he Cambridge, Mass., protest was de-" Macs. Many software developers fear that cidedly different. These weren't the the Lotus win will make it harder to bring Tusual malcontents from Harvard or new products to market. So when protest Boston University; these were computer ers marched in front of Lotus's Cambridge programmers hewing picket signs. The en headquarters earlier this month, they emy: giant Lotus Development Corp., chanted with a sly reference to the hexa which is trying to protect the market lead decimal counting scheme that is a basic of its 1-2-3 software package by bringing tool of their trade: "look and feel" suits against look-alike 1-2-3A kick the lawsuits out the door competitors. Lotus had recently won its 5-6'7-8 innovate don't litigate first big victory against Paperback Soft 9-A-B-C interfaces should be free ware International, which has sold its VP D-E-F-0 look and feel has got to gol Planner for a fifth of 1-2-3's $495 list price. The group behind the protests is the. Copyright rules that worked fine for League for Programming Freedom, found books and paintings are now straining to ed by Richard Stallman, a software gum cover works from music videos to digital who recently got a $240,000 MacArthur audiotapes—and, increasingly, software. grant. Stallman says the suits stifle innova Paperback and other challengers believed tion, paving the way for Japan to take over that the interface that a program presents the industry. -

Excel 2010: Where It Came From
1 Excel 2010: Where It Came From In This Chapter ● Exploring the history of spreadsheets ● Discussing Excel’s evolution ● Analyzing why Excel is a good tool for developers A Brief History of Spreadsheets Most people tend to take spreadsheet software for granted. In fact, it may be hard to fathom, but there really was a time when electronic spreadsheets weren’t available. Back then, people relied instead on clumsy mainframes or calculators and spent hours doing what now takes minutes. It all started with VisiCalc The world’s first electronic spreadsheet, VisiCalc, was conjured up by Dan Bricklin and Bob Frankston back in 1978, when personal computers were pretty much unheard of in the office environment. VisiCalc was written for the Apple II computer, which was an interesting little machine that is something of a toy by today’s standards. (But in its day, the Apple II kept me mesmerized for days at aCOPYRIGHTED time.) VisiCalc essentially laid theMATERIAL foundation for future spreadsheets, and you can still find its row-and-column-based layout and formula syntax in modern spread- sheet products. VisiCalc caught on quickly, and many forward-looking companies purchased the Apple II for the sole purpose of developing their budgets with VisiCalc. Consequently, VisiCalc is often credited for much of the Apple II’s initial success. In the meantime, another class of personal computers was evolving; these PCs ran the CP/M operating system. A company called Sorcim developed SuperCalc, which was a spreadsheet that also attracted a legion of followers. 11 005_475355-ch01.indd5_475355-ch01.indd 1111 33/31/10/31/10 77:30:30 PMPM 12 Part I: Some Essential Background When the IBM PC arrived on the scene in 1981, legitimizing personal computers, VisiCorp wasted no time porting VisiCalc to this new hardware environment, and Sorcim soon followed with a PC version of SuperCalc. -

Antonio Tajani MEP President of the European Parliament [email protected]
Antonio Tajani MEP President of the European Parliament [email protected] 12 June 2018 Mr President, Article 13 of the EU Copyright Directive Threatens the Internet As a group of the Internet’s original architects and pioneers and their successors, we write to you as a matter of urgency about an imminent threat to the future of this global network. The European Commission’s proposal for Article 13 of the proposed Directive for Copyright in the Digital Single Market Directive was well-intended. As creators ourselves, we share the concern that there should be a fair distribution of revenues from the online use of copyright works, that benefits creators, publishers, and platforms alike. But Article 13 is not the right way to achieve this. By requiring Internet platforms to perform automatic filtering all of the content that their users upload, Article 13 takes an unprecedented step towards the transformation of the Internet from an open platform for sharing and innovation, into a tool for the automated surveillance and control of its users. Europe has been served well by the balanced liability model established under the Ecommerce Directive, under which those who upload content to the Internet bear the principal responsibility for its legality, while platforms are responsible to take action to remove such content once its illegality has been brought to their attention. By inverting this liability model and essentially making platforms directly responsible for ensuring the legality of content in the first instance, the business models and investments of platforms large and small will be impacted. The damage that this may do to the free and open Internet as we know it is hard to predict, but in our opinions could be substantial. -

Digital Media & Learning Conference
DIGITAL MEDIA & LEARNING CONFERENCE MARCH 1-3, 2012 // SAN FRANCISCO, CALIFORNIA DML2012 TABLE OF CONTENTS COMMITTEE & SPONSORS...............................5 OVERVIEW............................................................ 6 ABOUT THE THEME: BEYOND EDUCATIONAL TECHNOLOGY.......6 CONFERENCE CHAIR & COMMITTEE ...................................7 KEYNOTES AND PLENARY PANELISTS ...............................9 CONFERENCE INFORMATION ..........................................12 CONFERENCE SCHEDULES & ABSTRACTS MARCH 1 ..................................................................13 MARCH 1 MOZILLA SCIENCE FAIR EXHIBITORS ...................24 MARCH 2 .................................................................27 MARCH 3 .................................................................39 CONFERENCE TRAVEL GUIDE & MAPS........55 3 BEYOND EDUCATIONAL TECHNOLOGY 2012 DIGITAL MEDIA & LEARNING CONFERENCE Parc 55 Wyndham // San Francisco, California // March 1-3, 2012 CONFERENCE CHAIR Diana Rhoten CONFERENCE COMMITTEE Tracy Fullerton Re-imagining Media for Learning Chair Antero Garcia Innovations for Public Education Chair Jess Klein Democratizing Learning Innovation Co-Chair Mitch Resnick Making, Tinkering and Remixing Chair Mark Surman Democratizing Learning Innovation Chair KEYNOTE PRESENTERS John Seely Brown PLENARY PANELISTS Elizabeth Corcoran Mitch Kapor Ronaldo Lemos Vicki Phillips Leslie Redd Carina Wong Constance M. Yowell HOSTED BY THANKS TO OUR SPONSORS 5 CONFERENCE OVERVIEW The Digital Media and Learning Conference is an -
Future of Leadership Corporate Hindsight Ofers Insights
Future of Leadership Corporate hindsight ofers insights. However, often too late, and often only after being dissected by every, invited and uninvited, self-acclaimed expert. It is too easy to pass judgement on past events, from the airport executive lounge a few years after mayhem, as a tech-savvy columnist, or as a case study writer decades after. Having corporate extinctions, a moonshot, or some other outlier spelled out in retrospect, while being interesting, only serves as a small tool in the real-time leadership toolbox. Quite often, these insights are transformed in to platitudes that might sound fantastic on social media, or in a key note, but represents little to no strategic value. Platitudes do not belong in a toolbox. Still, future leaders should seek insights from others; but it should be as “insights through conversation”. The art of it is to identify who should be part of that conversation. By conversation is not meant board meeting – but actual conversation. Many board meetings are still reserved for what could be phrased as “the boardroom boogie”. Every move is anticipated, rehearsed and pre-approved. What better way to spark an insightful and exploratory conversation than with a little help from a few questions? With the support from +100 leadership experts in Denmark and the United States, the key deliverable of this publication is a subset of 12 questions, for the board and C-suite to explore. The objective of the conversation, should not be to come up with immediate answers to the questions, it is more a “talk about the meaning of the question to us” type of conversation. -
Ww2010-Programs-Web-Pdf.Pdf
1 Program Design by Jake Mix, KEI Creative Mitchell Kapor Foundation presents November 8, 2010, 8:30 AM–6:30 PM November 9, 2010, 9 AM–4 PM David Brower Center 2150 Allston Way, Berkeley, CA 94704 Mitchell Kapor Foundation 543 Howard Street, 5th Floor www.mkf.org San Francisco, CA 94105 3 8:30-9:30 AM Registration 'SRXMRIRXEP&VIEOJEWX Mingling 9:30-10:00 AM Welcome & Convening Launch Mitch Kapor & Freada Kapor Klein Cedric Brown Carmen Rojas 10:00 AM-12:00 PM 7IXXMRKXLI'SRXI\X'VMQMREPM^EXMSRSJ6EGI Moderator Kung Li, Southern Center for Human Rights Melanie Cervantes Zachary Norris, Justice for Families James Rucker, Citizen Engagement Laboratory Saket Soni, New Orleans Workers’ Center for Racial Justice 12:00 -1:30 PM Lunch 1:30-3:00 PM 3RXLI+VSYRHMR Moderator Danielle Mahones, Center for Third World Organizing Nicole Lee Carlos Garcia, Movimiento Puente AZ Hamid Khan, South Asian Network Juan Rodriguez, Florida Immigration Coalition/Trail of Dreams 3:00-3:30 PM Break %+)2(%(%=23:)1&)6 3:30-5:00 PM Uniting Across Sectors & Communities Moderator Manuel Criollo, Labor Community Strategy Center Joshua Arce Maria Poblet, Causa Justa::Just Cause Alicia Garza, People Organized to Win Employment Rights Max Rameaux, Take Back the Land 3:30-5:00 PM Resourcing the Movement Moderator Melanie Cervantes, Akonadi Foundation Jakada Imami Mario Lugay, Mitchell Kapor Foundation Guillermo Quinteros, Solidago Foundation 5:00-6:30 PM Reception & Keynote Angela Davis, Critical Resistance $ Criminalization 3RXLI+VSYRH Uniting Across Resourcing SJ6EGI 1:30-3:00 -
Can Visicorp Come Back?
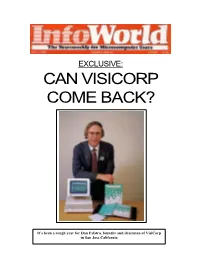
EXCLUSIVE: CAN VISICORP COME BACK? It’s been a rough year for Dan Fylstra, founder and chairman of VisiCorp in San Jose California CAN VISICORP COME BACK? Company regroups after corporate version of the Civil War BY DENISE CARUSO Reporter Dan Fylstra, cofounder and chairman of VisiCorp, sits waiting for his chicken teriyaki at Theo's, a quiet and elegant restaurant in Palo Alto, California. Theo's is frequented by the more well-to-do of the Silicon Valley set. Passing by, someone says with a chuckle, "Hey Dan, how ya doin' ? Been reading about you in the papers!" Fylstra grimaces. "I wouldn't wish these past six months on anyone," he says. "It's been really difficult on me, personally, as well as the company. People stop and say things like that all the time." VisiCorp, the San Jose, California, company credited with starting the micro-computer software industry in 1978 with its introduction of a spreadsheet program called VisiCalc, has been suffering for more than a year. Sales of VisiCalc began to drop sharply in June 1983, putting the company in the red by year's end, for the first time since 1979. A nasty legal imbroglio with Software Arts, the company that developed VisiCalc, slowed sales even more and has preoccupied Fylstra and other company managers, diverting their time from management of the company. And buyer acceptance of Visi On, the company's groundbreaking integrated applications environment, has been slower than the company had hoped. When, in late May, the company had a "reduction in force" (the oft-used euphemism for laying off employees a company can no longer afford to keep), rumors that began circulating months earlier — of bankruptcy, acquisition, raiding by headhunt- ers, even money funneled to Swiss bank accounts — increased exponentially in intensity. -

List of Programmers 1 List of Programmers
List of programmers 1 List of programmers This list is incomplete. This is a list of programmers notable for their contributions to software, either as original author or architect, or for later additions. A • Michael Abrash - Popularized Mode X for DOS. This allows for faster video refresh and square pixels. • Scott Adams - one of earliest developers of CP/M and DOS games • Leonard Adleman - co-creator of RSA algorithm (the A in the name stands for Adleman), coined the term computer virus • Alfred Aho - co-creator of AWK (the A in the name stands for Aho), and main author of famous Dragon book • JJ Allaire - creator of ColdFusion Application Server, ColdFusion Markup Language • Paul Allen - Altair BASIC, Applesoft BASIC, co-founded Microsoft • Eric Allman - sendmail, syslog • Marc Andreessen - co-creator of Mosaic, co-founder of Netscape • Bill Atkinson - QuickDraw, HyperCard B • John Backus - FORTRAN, BNF • Richard Bartle - MUD, with Roy Trubshaw, creator of MUDs • Brian Behlendorf - Apache • Kent Beck - Created Extreme Programming and co-creator of JUnit • Donald Becker - Linux Ethernet drivers, Beowulf clustering • Doug Bell - Dungeon Master series of computer games • Fabrice Bellard - Creator of FFMPEG open codec library, QEMU virtualization tools • Tim Berners-Lee - inventor of World Wide Web • Daniel J. Bernstein - djbdns, qmail • Eric Bina - co-creator of Mosaic web browser • Marc Blank - co-creator of Zork • Joshua Bloch - core Java language designer, lead the Java collections framework project • Bert Bos - author of Argo web browser, co-author of Cascading Style Sheets • David Bradley - coder on the IBM PC project team who wrote the Control-Alt-Delete keyboard handler, embedded in all PC-compatible BIOSes • Andrew Braybrook - video games Paradroid and Uridium • Larry Breed - co-developer of APL\360 • Jack E. -

The Untold Story of How Calgary's Garrett Camp
The untold story of how Calgary’s Garrett Camp changed the Internet, blew up the transportation industry and became the third-richest man in Canada—all while remaining virtually anonymous BY STEPHEN M. BALDWIN ILLUSTRATION BY M.ORE 36 MAY 2016 / REPORT ON BUSINESS really just more of an adviser to Uber, he engineering. His thesis was on information retrieval through collaborative interface design insists. “I can talk about it generally,” he and evolutionary algorithms. In other words, combining technology with a tight-knit com- says, “but when you’re on the board of a munity to improve search results. When he and his friend Geoff Smith, along with two company, you don’t have the daily exposure of Smith’s co-workers, began batting around ideas for their own company, the notion of to these sorts of issues. I just don’t think building a community-driven tool to help users find interesting web pages emerged as the it’s your place to comment on something obvious choice. StumbleUpon—the name was Camp’s idea—launched in November, 2001. UBER BRO Uber owes its brash unless you’re well-informed.” Camp summed it up this way: “Google is cool if you know what you want. But what if you and combative Truth be told, Camp has already moved don’t know what you want?” Users would select general categories they were interested style to its CEO. past Uber—let Kalanick deal with the in, then “stumble” through related pages with the click of a button. They could also give THERE’S NOTHING Here are a few classic PARTICULARLY cease-and-desist orders from municipali- pages thumbs-up or thumbs-down reviews, which taught StumbleUpon which content Travis Kalanick ties worldwide, the scores of lawsuits and users wanted. -

Science Trivia Questions Xiv
SCIENCE TRIVIA QUESTIONS XIV ( www.TriviaChamp.com ) 1> Created by Mitch Kapor, what killer app spreadsheet was named for the padmasana yoga position? a. Microsoft Excel b. VisiCalc c. Lotus 1-2-3 d. Quattro Pro 2> When the University of Cambridge was closed due to plague, I retreated to Woolsthorpe, where I did some of my most important work on motion, optics and mathematics. Who am I? a. Isaac Newton b. John Locke c. Michael Faraday d. Thomas Hobbes 3> Proving you can't be a genius all the time, William Shockley shocked folks with shocking racist theories. But he and his crew at Bell Labs also developed what invention, which replaced vacuum tubes and changed the technological world? a. Fiber optics b. Transistor c. Particle accelerator d. Microwave ovens 4> As a boy, Joseph Meister was the first person I saved from rabies. And he in turn became caretaker of the institute named for me. Who am I? a. Joseph Lister b. Jonas Salk c. Louis Pasteur d. Bernard Christian 5> The ceremonial first American AMPS cellular call was made on October 13, 1983, at Soldier's Field in Chicago, when Bob Barnett, Ameritech Mobile's president, called what inventor's grandson in Berlin? a. Werner Von Braun b. Nikola Tesla c. Alexander Graham Bell d. Thomas Edison 6> Possibly because it does less damage when it hits its targets, what less lethal metal does the Lone Ranger have his bullets made from? a. Gold b. Silver c. Lead d. Tin 7> What constellation would you take by the horns if you wanted to see the Crab Nebula and such star clusters as the Hyades and the Pleiades? a.