National Fatality Review Case Reporting System Data Dictionary
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Oregon Kids: Healthy and Safe Vol. 3
OREGON KIDS: HEALTHY AND SAFE Volume 3 E-Reference A health and safety guide for early care and education providers PUBLIC HEALTH DIVISION Office of Family Health ACCESSING VOLUME 3 AND VOLUME 4 OKHS Volume 3: E-Reference gives you detailed information about the health and safety subjects introduced in OKHS volumes 1 and 2. OKHS Volume 4 is an appendix to volume 3 that contains documents and forms to download and print. TO ACCESS ONE OR BOTH OF THESE DOCUMENTS Scan this quick response (QR) code with your smartphone, tablet or other handheld device to download the Volume 3, E-Reference, and Volume 4, Appendix to the E-Reference as either an interactive PDF or E-book OR Go to the following website: http://public.health.oregon.gov/HealthyPeopleFamilies/Babies/ HealthChildcare/Pages/OKHS.aspx Sign up for the OKHS Training Session — You will learn up-to-date information about: • Promoting children’s health; • Preventing common childhood illnesses and injuries. For trainings in your area, contact your local Child Care Resource & Referral office or visit the training calendar at http://www.oregonchildcaretraining.org. Oregon Kids, Healthy and Safe is a joint project among the following partners: State of Oregon Employment Department CHI LD C ARE PUBLIC HEALTH DIVISION DIVISIO N Office of Family Health ACKNOWLEDGMENTS The Oregon Kids: Healthy and Safe volumes 1, 2, 3 and 4 are the result of a collaborative effort among many early care and education and health care partners. We wish to thank the following individuals and organizations for guiding -
Euro-Nmd Patient Representatives Booklet
EURO-NMD PATIENT REPRESENTATIVES BOOKLET JUNE 2020 EURO-NMD Patient Representatives – 11/06/2020 1 EURO-NMD Meeting, Freiburg, 29-30 November 2017 INTRODUCTION The Patient Advisory Board (PAB) aims to ensure true and equitable representation of the voice of patients within the EURO-NMD network so that EURO-NMD services can answer to the needs and expectations of rare neuromuscular disease patients and improve access to high quality diagnosis, care and treatment. The PAB creates a bridGe between the ERN and the rare neuromuscular patient community, by coordinatinG the participation of all patient representatives in the Network, and liaisinG with its affiliated patient orGanisations. The Patient Advisory Board also endorses additional patient representatives to join Specialist Groups based on their expertise. The PAB has established its own Constitution and Rules of Procedure. Membership: Members of the PAB include those elected via EURORDIS who constitute the European Patient Advocacy Group for EURO-NMD. Members from umbrella orGanisations (e.g. Spierziekten Nederland) have also been invited to join the Patients Advisory Board to ensure a proper representation of the neuromuscular patient community amonG the PAB. ePAG representatives: ‹ François Lamy (AFM-Téléthon, France), ‹ Dimitrios Athanasiou (MDA-Hellas), ‹ Massimo Marra and Patrizia Garzena (alternate) (CIDP Italia ONLUS), ‹ Marisol Montolio (Duchenne Parent Project Spain), ‹ Michela Onali (Gli Equilibristi HIBM, Italy) ‹ Jean-Philippe Plançon (French Association against Peripheral Neuropathies, France - European Patient OrGanisation for Dysimmune and Inflammatory Neuropathies, EU), ‹ Evy Reviers (ALS LiGa Belgium), ‹ Judit Varadine Csapo (Angyalszarnyak HunGarian Muscle Dystrophy Association). Other NMD patient representatives: ‹ Madelon Kroneman (Spierziekten Nederland, Dutch Patient Society of Neuromuscular Diseases), The members of the PAB will commit to assist in the following: ‹ Governance of the ERN: The ERN Board will include the patient representatives that are part of the Patient Advisory Board. -

Placement of Children with Relatives
STATE STATUTES Current Through January 2018 WHAT’S INSIDE Placement of Children With Giving preference to relatives for out-of-home Relatives placements When a child is removed from the home and placed Approving relative in out-of-home care, relatives are the preferred placements resource because this placement type maintains the child’s connections with his or her family. In fact, in Placement of siblings order for states to receive federal payments for foster care and adoption assistance, federal law under title Adoption by relatives IV-E of the Social Security Act requires that they Summaries of state laws “consider giving preference to an adult relative over a nonrelated caregiver when determining a placement for a child, provided that the relative caregiver meets all relevant state child protection standards.”1 Title To find statute information for a IV-E further requires all states2 operating a title particular state, IV-E program to exercise due diligence to identify go to and provide notice to all grandparents, all parents of a sibling of the child, where such parent has legal https://www.childwelfare. gov/topics/systemwide/ custody of the sibling, and other adult relatives of the laws-policies/state/. child (including any other adult relatives suggested by the parents) that (1) the child has been or is being removed from the custody of his or her parents, (2) the options the relative has to participate in the care and placement of the child, and (3) the requirements to become a foster parent to the child.3 1 42 U.S.C. -

Indian Surrogacy: Ending Cheap Labor
Santa Clara Journal of International Law Volume 18 Issue 1 Article 1 1-12-2020 Indian Surrogacy: Ending Cheap Labor Jaya Reddy Follow this and additional works at: https://digitalcommons.law.scu.edu/scujil Part of the International Law Commons Recommended Citation Jaya Reddy, Comment, Indian Surrogacy: Ending Cheap Labor, 18 SANTA CLARA J. INT'L L. 92 (2020). Available at: https://digitalcommons.law.scu.edu/scujil/vol18/iss1/1 This Comment is brought to you for free and open access by the Journals at Santa Clara Law Digital Commons. It has been accepted for inclusion in Santa Clara Journal of International Law by an authorized editor of Santa Clara Law Digital Commons. For more information, please contact [email protected], [email protected]. 18 SANTA CLARA JOURNAL OF INTERNATIONAL LAW 92 (2020) Indian Surrogacy: Ending Cheap Labor Jaya Reddy !92 Indian Surrogacy: Ending Cheap Labor Table of Contents I. Introduction ..............................................................................................................................94 II. Background ..............................................................................................................................94 A. 2002: Legalization of Commercial Surrogacy Caused Exploitation but Allowed Impoverished Women to Escape Poverty ............................................................................................................94 B. 2005: Indian Council for Medical Research Issued Extremely Narrow Guidelines Regulating “ART” ............................................................................................................................................98 -
NAEYC Early Learning Program Accreditation Standards and Assessment Items Approved by the NAEYC Council on the Accreditation of Early Learning Programs
NAEYC Early Learning Program Accreditation Standards and Assessment Items Approved by the NAEYC Council on the Accreditation of Early Learning Programs *Applies to all accreditation site visits beginning July 2019 until otherwise informed. NAEYC Early Learning Program Accreditation Standards and Assessment Items Copyright 2019 National Association for the Education of Young Children. All rights reserved. NAEYC Early Learning Program Accreditation Standards and Assessment Item 1 National Association for the Permissions Education of Young Children Readers of NAEYC Early Learning Program Accreditation Standards 1313 L Street NW, Suite 500 and Assessment Items are permitted to photocopy and distribute Washington, DC 20005-4101 up to 25 copies of this publication (including electronic copies 202-232-8777 • 800-424-2460 distributed to more than 25 recipients) for educational or training NAEYC.org purposes only. Photocopies may only be made from an original copy of this publication. NAEYC accepts requests for limited use of our copyrighted NAEYC Accreditation material. For permission to reprint, adapt, translate, or Chief Strategy and otherwise reuse and repurpose content from this publication Innovation Officer, more extensively than outlined above, review our guidelines at Michelle Kang NAEYC.org/resources/permissions. Senior Director, NAEYC Photo Credits Accreditation of All photos copyright © Getty Images Early Learning Programs Kristen Johnson NAEYC Early Learning Program Accreditation Standards Director, Quality Assessment and Assurance and Assessment Items. Copyright © 2019 by the National Susan Hedges Association for the Education of Young Children. All rights reserved. Printed in the United States of America. Senior Reliability Specialist Amanda Batts Director, Quality Improvement and Program Support April D. Kimble Senior Creative Design Manager Henrique J. -
V5 Sectiona-CDR 02-07-18.Xlsx
CDR Report Form National Fatality Review Case Reporting System Version 5.0 Data entry website: https://data.ncfrp.org 1-800-656-2434 [email protected] www.ncfrp.org SAVING LIVES TOGETHER Instructions: This case report is used by Child Death Review (CDR) teams to enter data into the National Fatality Review Case Reporting System (NFR-CRS). The NFR-CRS is available to states and local sites from the National Center for Fatality Review & Prevention (NCFRP) and requires a data use agreement for data entry. The purpose is to collect comprehensive information from multiple agencies participating in a review. The NFR-CRS documents demographics, the circumstances involved in the death, investigative actions, services provided or needed, key risk factors and actions recommended and/or taken by the team to prevent other deaths. While this data collection form is an important part of the CDR process, it should not be the central focus of the review meeting. Experienced users have found that it works best to assign a person to record data while the team discussions are occurring. Persons should not attempt to answer every single question in a step-by-step manner as part of the team discussion. It is not expected that teams will have answers to all of the questions related to a death. However, over time teams begin to understand the importance of data collection and bring the necessary information to the meeting. The percentage of cases marked "unknown" and unanswered questions decreases as the team becomes more familiar with the form. The NFR-CRS Data Dictionary is available. -

Infant Safe Haven Laws a Safe Haven
STATE STATUTES Current Through December 2016 WHAT’S INSIDE Who may leave a baby at Infant Safe Haven Laws a safe haven Many State legislatures have enacted legislation to Safe haven providers address infant abandonment and endangerment in Responsibilities of safe response to a reported increase in the abandonment haven providers of infants in unsafe locations, such as public restrooms or trash receptacles. Beginning in Texas Immunity for providers in 1999, “Baby Moses laws” or infant safe haven laws have been enacted as an incentive for mothers in Protections for parents crisis to safely relinquish their babies to designated Consequences of locations where the babies are protected and relinquishment provided with medical care until a permanent home is found. Safe haven laws generally allow the parent, Summaries of State laws or an agent of the parent, to remain anonymous and to be shielded from criminal liability and prosecution for child endangerment, abandonment, or neglect in To find statute exchange for surrendering the baby to a safe haven. information for a particular State, go to https://www.childwelfare. gov/topics/systemwide/ laws-policies/state/. Children’s Bureau/ACYF/ACF/HHS 800.394.3366 | Email: [email protected] | https://www.childwelfare.gov Infant Safe Haven Laws https://www.childwelfare.gov To date, all 50 States, the District of Columbia, and Puerto Safe Haven Providers Rico have enacted safe haven legislation.1 The focus of these laws is protecting newborns from endangerment by The purpose of safe haven laws is to ensure that providing parents an alternative to criminal abandonment, relinquished infants are left with persons who can provide and therefore the laws are generally limited to very the immediate care needed for their safety and well- young children. -
Getting Ready for Baby
Getting Ready for Baby Safety Guide Table of Contents Unintentional Injuries in Babies and Young Children .................................................................4 Suffocation and SIDS (Safe Sleep) ......................................................................................................6 Burns and Scalds .......................................................................................................................................8 Poisoning and Medication Safety ....................................................................................................10 Drowning .................................................................................................................................................13 Choking .....................................................................................................................................................15 Falls .............................................................................................................................................................16 Infant Crying and Shaken Baby Syndrome ..................................................................................17 Motor Vehicle Safety ............................................................................................................................18 Other Safety Tips ...................................................................................................................................20 Additional Resources ...........................................................................................................................21 -

International Surrogacy Arrangements and the Establishment of Legal Parentage
International surrogacy arrangements and the establishment of legal parentage THEMIS-Competition 2015 Semi Final B International Cooperation in Civil Matters – European Family Law Team Austria 2 Mag.a Teresa Schön Mag.a Sabine Tagwerker Mag.a Magdalena Zabl Tutor: Mag.a Christine Miklau Vienna, 16th April 2015 Introduction Due to scientific as well as social developments in the last decade, the number of people wanting to undergo the process of surrogacy has increased enormously. There is on one side the declining fertility rate (the total world fertility rate1 in 2000 was 2.8 while 2014 it decreased to 2.43 children born per woman) which affects especially industrialised countries (e.g. in 2012 European countries had total fertility rates between 1.1 and 1.6 children born/woman2). On the other side there are the growing scientific achievements in the field of in-vitro-fertilisation (hereinafter IVF) which make it possible to circumvent infertility in an increasing number of cases. Furthermore the acceptance within the world population for such methods has risen. As a consequence from the medical point of view it has become fairly easy for couples, who have the desire to have children, to have their “own” baby. From the legal point of view these possibilities lead to various problems. One part of the problem is that in some countries surrogacy is explicitly prohibited and most countries still don’t have any regulations concerning surrogacy. In Europe e.g. Denmark, Greece, Ukraine and the United Kingdom (at least partly, namely only in cases where the surrogate mother is not paid beyond her “reasonable expenses”) allow surrogacy while in other European states surrogacy is either prohibited or not regulated. -

Child Unintentional Deaths and Injuries in New Zealand, and Prevention Strategies
Child Unintentional Deaths and Injuries in New Zealand, and Prevention Strategies This report outlines New Zealand child injury data and effective or promising injury prevention strategies Executive Summary 1. Introduction 3 Land transport injuries 4 Choking, Suffocation and Strangulation 2 Child unintentional injuries in New Zealand: A snapshot of recent trends 5 Falls 6 Drowning 7 Inanimate mechanical forces 8 Animate mechanical forces 9 Poisoning 10 Burns and scalds Use this colour guide to find the injury topic immediately from the fore edge of this book. Child Unintentional Deaths and Injuries in New Zealand, and Prevention Strategies Safekids Aotearoa Suggested citation: Safekids Aotearoa. (2015). Child Unintentional Deaths and Injuries in New Zealand, and Prevention Strategies. Auckland, NZ: Safekids Aotearoa. You are welcome to use information from this publication as long as you acknowledge Safekids Aotearoa as the source. Safekids Aotearoa 5th Floor, Cornwall Complex, 40 Claude Road, Epsom, Auckland 1023 PO Box 26488, Epsom, Auckland 1344 New Zealand P. +64 9 9955 F. +64 9 630 9961 ISBN: 978-0-9941125-7-6 (Print) ISBN: 978-0-9941125-8-3 (Online) Published December 2015 Disclaimer Safekids Aotearoa has endeavoured to ensure material in this document is technically accurate and reflects legal requirements. However, the document does not override legislation. Safekids Aotearoa does not accept liability for any consequences arising from the use of this document. If the user of this document is unsure whether the material is correct, they should make direct reference to the relevant legislation and contact Safekids Aotearoa. This publication updates information contained in Analysis of unintentional child injury data in New Zealand: Mortality (2001-2005) and Morbidity (2003-2007). -

JOIN the MOVEMENT to PREVENT CHILD ABANDONMENT and CARE for ORPHANS: 1 2 3 RAISE YOUR VOICE SPONSOR a CHILD ADOPT Volunteer with Holt
WWW.HOLTINTERNATIONAL.ORG P.O. BOX 2880, EUGENE, OR, 97402 541-687-2202 PMS 584c PMS 583c PMS 7462c BLACK JOIN THE MOVEMENT TO PREVENT CHILD ABANDONMENT AND CARE FOR ORPHANS: 1 2 3 RAISE YOUR VOICE SPONSOR A CHILD ADOPT Volunteer with Holt. Share stories For $30 per month, you give a For many children, adoption is on social media. Tell your church voice to the voiceless and transform the best route to a permanent, about vulnerable children. Start a a child’s world forever. Visit loving family. Learn more about fundraiser. There are so many ways holtinernational.org/sponsorship to our adoption programs at to advocate for children in need. become a child sponsor. holtinternational.org/adoption. Uplifting children. Strengthening families. At Holt International, we seek a world where every child has the support to reach their full potential — a world where every child has a loving and secure home. Around the world, we work toward our vision by providing individualized, child-focused services in three main program areas: 1 2 PMS 584c PMS 583c3 PMS 7462c BLACK ORPHAN & VULNERABLE ADOPTION SERVICES: FAMILY CHILDREN CARE: When adoption is the best option for a child, our local partners STRENGTHENING: first strive to find a domestic Through our global network of adoptive family — giving the local, on-the-ground experts child the opportunity to grow We believe that children should and in-country partnerships, we up in the country and culture of grow up in the loving care of their ensure that children who have their birth. When international families. -
Spring 2015 Vol
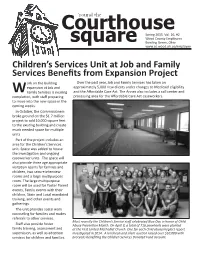
Courthouse‘round the Spring 2015 Vol. 26, #2 Wood County Employees square Bowling Green, Ohio www.co.wood.oh.us/employee Children’s Services Unit at Job and Family Services BeneĮ ts from Expansion Project ork on the building Over the past year, Job and Family Services has taken on expansion at Job and approximately 5,000 new clients under changes to Medicaid eligibility W Family Services is nearing and the Aī ordable Care Act. The Annex also includes a call center and compleƟ on, with staī preparing processing area for the Aī ordable Care Act caseworkers. to move into the new space in the coming weeks. In October, the Commissioners broke ground on the $1.7 million project to add 10,000 square feet to the exisƟ ng building and create much needed space for mulƟ ple units. Part of the project includes an area for the Children’s Services unit. Space was added to house the invesƟ gaƟ on and ongoing caseworker units. The space will also provide three age appropriate visitaƟ on rooms for families and children, two secure interview rooms and a large mulƟ purpose room. The large mulƟ purpose room will be used for Foster Parent events, Family events with their children, State and Local mandated training, and other events and gatherings. The unit provides social work counseling for families and makes referrals to other services. Most recently the Children’s Service staī celebrated Blue Day in honor of Child Staī also provide foster Abuse PrevenƟ on Month. On April 8, a total of 716 pinwheels were planted family training, assessment and at the First United Methodist Church.