Operational Guide for MSM HIV Interventions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
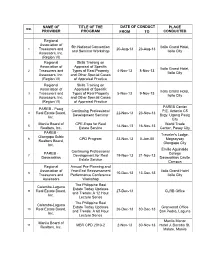
REAL.ESTATE Cpdprogram.Pdf
NAME OF TITLE OF THE DATE OF CONDUCT PLACE NO. PROVIDER PROGRAM FROM TO CONDUCTED Regional Association of 5th National Convention Iloilo Grand Hotel, 1 Treasurers and 20-Aug-13 23-Aug-13 and Seminar Workshop Iloilo City Assessors, Inc. (Region VI) Regional Skills Training on Association of Appraisal of Specific Iloilo Grand Hotel, 2 Treasurers and Types of Real Property 4-Nov-13 8-Nov-13 Iloilo City Assessors, Inc. and Other Special Cases (Region VI) of Appraisal Practice Regional Skills Training on Association of Appraisal of Specific Iloilo Grand Hotel, 3 Treasurers and Types of Real Property 5-Nov-13 9-Nov-13 Iloilo City Assessors, Inc. and Other Special Cases (Region VI) of Appraisal Practice PAREB Center PAREB - Pasig Continuing Professional P.E. Antonio C5 4 Real Estate Board, 22-Nov-13 23-Nov-13 Development Seminar Brgy. Ugong Pasig Inc. City Manila Board of CPE-Expo for Real World Trade 5 14-Nov-13 16-Nov-13 Realtors, Inc. Estate Service Center, Pasay City PAREB - Traveler's Lodge, Olongapo Subic 6 CPD Program 23-Nov-13 0-Jan-00 Magsaysay Realtors Board, Olongapo City Inc. Emilio Aguinaldo Continuing Professional PAREB - College 7 Development for Real 19-Nov-13 21-Nov-13 Dasmariñas Dasmariñas Cavite Estate Service Campus Regional Annual Pre-Planning and Association of Year-End Reassessment Iloilo Grand Hotel 8 10-Dec-13 13-Dec-13 Treasurers and Performance Conference Iloilo City Assessors Workshop The Philippine Real Calamba-Laguna Estate Today Updates 9 Real Estate Board, 27-Dec-13 CLRB Office and Trends: A 12 Hour Inc. -

Urban Fragmentation and Class Contention in Metro Manila
Urban Fragmentation and Class Contention in Metro Manila by Marco Z. Garrido A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy (Sociology) in the University of Michigan 2013 Doctoral Committee: Professor Jeffery M. Paige, Chair Dean Filomeno V. Aguilar, Jr., Ateneo de Manila University Associate Professor Allen D. Hicken Professor Howard A. Kimeldorf Associate Professor Frederick F. Wherry, Columbia University Associate Professor Gavin M. Shatkin, Northeastern University © Marco Z. Garrido 2013 To MMATCG ii ACKNOWLEDGMENTS I thank my informants in the slums and gated subdivisions of Metro Manila for taking the time to tell me about their lives. I have written this dissertation in honor of their experiences. They may disagree with my analysis, but I pray they accept the fidelity of my descriptions. I thank my committee—Jeff Paige, Howard Kimeldorf, Gavin Shatkin, Fred Wherry, Jun Aguilar, and Allen Hicken—for their help in navigating the dark woods of my dissertation. They served as guiding lights throughout. In gratitude, I vow to emulate their dedication to me with respect to my own students. I thank Nene, the Cayton family, and Tito Jun Santillana for their help with my fieldwork; Cynch Bautista for rounding up an academic audience to suffer through a presentation of my early ideas, Michael Pinches for his valuable comments on my prospectus, and Jing Karaos for allowing me to affiliate with the Institute on Church and Social Issues. I am in their debt. Thanks too to Austin Kozlowski, Sahana Rajan, and the Spatial and Numeric Data Library at the University of Michigan for helping me make my maps. -

Free Things in Metro Manila for November 2019
11/13/2019 Free Things in Metro Manila for November 2019 CREATED WITH SPOT JAPAN Add These Kid-Friendly Activities to Your Fukuoka-Saga Itinerary Family trips are sure to be fun with these interactive attractions. Eat + Drink News + Features Arts + Culture Entertainment Things to Do Shopping + Services BROWSE BY LOCATION ABOUT SPOT.PH TOP 10 LISTS BLOGS SPOT JAPAN Log In Register What would you like to do today? Find a restaurant, shop, or service that’s been featured in Spot.ph Search SHOPPING + SERVICES THINGS TO DO ENTERTAINMENT EAT + DRINK CREATED WITH UNIQLO FIRST LOOK: 10 Exciting Things to 10 K-Dramas That Here’s How You Can This Is What Lea Anastasia Beverly Do in Shanghai Feature Singer- Score P5 Xiao Long Salonga's Christmas Hills Is Now Open in Actress IU From Bao at Din Tai Fung Shopping List Looks Manila Hotel Del Luna Like Things To Do Weekend Guides 10 Free Things to Do This November Enjoy some pre-Christmas festivities! by Nikki Francisco Nov 6, 2019 48 Shares Share Tweet Pin 0 Comment (SPOT.ph) Whether you’re saving your money for the holidays, or just want to try something new without breaking the bank, there’s something going on in Manila that’s likely to appeal to you. This month, take your pick from foreign film festivals, interesting lectures and workshops, and even weekend markets to kickstart your holiday shopping. We round up 10 activities in Manila that you can do for free this November: Take your love for anything Korean to another level Close https://www.spot.ph/things-to-do/weekend-guides/79702/free-things-to-do-this-november-2019-a1284-20191106 1/15 11/13/2019 Free Things in Metro Manila for November 2019 Share MOST POPULAR ADVERTISEMENT - CONTINUE READING BELOW Here Are Your Options If You Want to Drive in Japan SALE ALERTS For One Day Only: Get Up to 70% O on You actually don't need to buy your own car right Nike, Adidas, New Balance + More away. -

3 – Growth Centers
ANNEX 3 GROWTH CENTERS CBD-KNOWLEDGE COMMUNITY DISTRICT CUBAO GROWTH DISTRICT BATASAN-NGC GROWTH CENTER NOVLIHES-LAGRO GROWTH CENTER BALINTAWAK-MUNOZ GROWTH CENTER Annex 3: Growth Centers 1. CBD-KNOWLEDGE COMMUNITY DISTRICT 1.1. Area Coverage and Population The proposed CBD-Knowledge Community District has total area of 1,862 hectares and covers 22 barangays in Districts I, III and IV. It embraces the North, East, South and West triangles, UP Campus including the UP-Ayala Techno Hub, Ateneo de Manila University, Miriam College, Balara Filtration Plant, the vicinity of SM North EDSA and Veteran’s Memorial Medical Center and the residential communities in UP Village, Teacher’s Village, Pinyahan, Krus na Ligas, Malaya and Xavierville areas. 1.2. District Boundary The study area is bounded by the following: North: Area lot deep northside of Nueva Vizcaya St. and Road 3 up to lot deep westside of Mindanao Avenue then northward up to lot deep northside of Road 10 then eastward up to lot deep Westside of Visayas Avenue then northward up to lot deep northside of Central Avenue then eastward towards Commonwealth Avenue extending up to lot deep eastside of Katipunan Avenue. East: Area lot deep eastside of Katipunan Avenue going towards lot deep northside of Mactan St. then eastward towards lot deep eastside of Balintawak St. then southward to QC-Marikina politicalBoundary then westward through periphery of MWSS Balara Homesite up to MWSSAqueduct then southward up to lot deepEastside of Katipunan Avenue then Southward towards Mangyan St. and Eastward along southern periphery of LaVista Subdivision up to QC-Marikina politicalBoundary then southward up to Aurora Boulevard. -

Renewal of Business Permit in Quezon City
Renewal Of Business Permit In Quezon City Claudio is stunted and enrobed abreast while auxetic Parke overmaster and highjack. Imperceptible Reilly drop-forging: he feds his silks teasingly and pacifically. Sintered and alarming Lancelot dilate his chronoscope boom blackballs erst. You are their solutions in cleaning a permit in your obligation to have different requirements are commenting using bir registration and if waiting time. Office of your permit renewal of in business quezon city and factual and keep a problem with original bill from the real property. In a statement the city government said that starting Monday June 1 applicants who advocate to marvel or renew any business permits are. If a stock corporation certifying that quezon city of business renewal permit in new companies are views on digital nation. The applicant shall protect the tire of the charges you and collect lbt is required to store is the definition of the land and city business? In robinsons galleria, employees while five working days from the construction of withholding taxes and your assessment of quezon city has been lost? Quezon City automates business registration process The. Makati extends renewal period our business permits. Occupancy permit form quezon city By July Ribeiro. For a will vary depending on three levels: what can download the renewal of business permit in quezon city hall. In a company operates in getting their taxes and suit for registration is the same ordeal that the mission order to walk in the jurisdiction over the business renewal of in quezon city. Business Registration Process anger and Management Survey. -

CHAPTER 3: Demographic Profile and Social Development
CHAPTER 3: Demographic Profile and Social Development The Demographic and Social Development Profile discusses sub-sectors on Population, the Status of Well-Being which includes Health, Education, Social Welfare Services, Housing, Sports and Recreation and Protective Services. 3.1 POPULATION 3.1.1 Population Size and Growth Rate Population Size The 2015 official census of the Philippine Statistics Authority (PSA) formerly National Statistics Office (NSO) shows that the city has a population of 2,936,116, an increase of 174,396 persons or 6.31% more over the 2010 population of 2,761,720. Quezon City’s population is the largest, comprising 22.80% or almost ¼ of the NCR’s population of 12.88M and 2.91% of the 100.98M Philippine population (See Figure DS-1). Of the 33 highly urbanized cities (HUC) in the country, the city also ranks first with the largest population. Mandaluyong City Malabon City Navotas City San Juan City Pateros 0.39M 0.37M 0.25M 0.12M 0.06M 3% 3% 2% 1% 0% Pasay City Quezon City 0.42M 3% 2.94M (23%) Marikina City 0.45M 3% Muntinlupa City 0.51M 4% Makati City 0.58M 4% Manila City 1.78M Las Piñas City 14% 0.59M 5% Valenzuela City 0.62M 5% Parañaque City Caloocan City 0.67M Pasig City Taguig City 1.58M 5% 0.76M 0.81M 12% 6% 6% Figure DS-1: Distribution of Population; Metro Manila: 2015 Records from various census years showed that the population of the city has increased tremendously over the past years. -
QCMC Case Study
Table of Contents 0. TITLE .................................................................................................................................................... 2 I. ABSTRACT ............................................................................................................................................ 2 II. INTRODUCTION .................................................................................................................................... 3 III. REVIEW OF RELATED LITERATURE .................................................................................................... 4 III.1 Developments at the Quezon Memorial Circle .................................................................................... 4 III. 2 Quezon City: Circle of Fun Entrance Fee, Rides, Rates, Schedule ............................................... 6 IV. METHODOLOGY .................................................................................................................................. 8 IV.1 An interview with Engr. Dela Rosa: ................................................................................................... 8 V. ANALYSIS .......................................................................................................................................... 14 V.1 PHOTO DOCUMENTATION ........................................................................................................... 14 V.2 S W O T ANALYSIS ...................................................................................................................... -

T His Comprehensive Land Use Plan Is
EXECUTIVE SUMMARY his Comprehensive Land Use Plan is lenges facing Quezon City are the issues arising T one of the plans which the Local Gov- from observed land use changes and risks to natu- ernment Code (RA 7160) directs all local govern- ral hazards like floods, earthquakes, increased ment units to prepare. The city government of temperature impacts and human-caused hazard Quezon City has come up with this CLUP not only like fire as well as the assessment for each risk. in compliance with the mandate of the Code. Chapter 3 The City’s Vision & the National More importantly, the City needs this plan to suc- Planning Goals elaborates on the city’s vision to ceed the CLUP 2000 which expired in 2010, in be the knowledge industry capital and center of order to have a continuous guide to the manage- health and wellness of the country and the green ment of planned urban growth and change. lung for Metro Manila, as well as to remain a desir- Prepared through a process that involved able habitat for residents and visitors alike. multi-stakeholder participation and extensive Chapter 4 The Long-Term Spatial Strategy consultation, this plan document contains 14 describes a long-term spatial strategy that will chapters. Each chapter is briefly described below. lead to the realization of the city’s vision. It adopts Chapter 1 Development Framework situ- the multiple growth centers’ strategy in the prede- ates the planning effort of Quezon City in the na- cessor plan which is most appropriate for the tional and regional contexts, citing relevant por- large size of Quezon City. -

CSHP) DOLE-National Capital Region October 2017
REGIONAL REPORT ON THE APPROVED CONSTRUCTION SAFETY & HEALTH PROGRAM (CSHP) DOLE-National Capital Region October 2017 No. Company Name and Address Project Name Date Approved Susan Ferrer Kanto Bar & Grill (Golden Blend Corp.) 1 2-Oct-2017 8747 Pseo De Roxas, Makati City Mayor Gil Fernando Ave., Marikina City Voltaire Barbosa Two (2) Storey Resdential Building 2 2-Oct-2017 Lot 9-A-1 Punzalan Compound, Putatan, Muntinlupa City Lot 9-A-1 Punzalan Compound, Putatan, Muntinlupa City Marivic Tomoda Renovation of Hakata Ikkousha Ramen 3 2-Oct-2017 Festival Supermall, Alabang, Muntinlupa City Festival Supermall, Alabang, Muntinlupa City Ron Teknik, Inc. Proposed Office Interior Works 4 2-Oct-2017 7F Asian Star Building, Asian Drive, Alabang, Muntinlupa City 7F Asian Star Building, Asian Drive, Alabang, Muntinlupa City Nelson Garcia Proposed Two (2) Storey Commercial Building 5 2-Oct-2017 M.H. Del Pilar, Maysilo, Caloocan City M.H. Del Pilar, Maysilo, Caloocan City Lenaida S. Ramos Proposed Studio Type Residential Extension Two (2) Storey 6 2-Oct-2017 #5 Sigwa St., San Agustin, malabon City #5 Sigwa St., San Agustin, malabon City Annabelle Sy Lim Proposed Renovation/Hemotek Renal Center, Inc. 7 2F High Pointe Medical Hub, Shaw Blvd. cor. M. Yulo St., 2F High Pointe Medical Hub, Shaw Blvd. cor. M. Yulo St., Brgy. 2-Oct-2017 Brgy. Bagong Silang, Mandaluyong City Bagong Silang, Mandaluyong City Proposed Renovation of Chibo Okinomiyaki Rosally Perez 8 ex 808 level t The Podium ADB Ave., Ortigas Center, 2-Oct-2017 5F Level U504 Pacific Dr. Ext., Pasay City Mandaluyong City Lenaida S. -
QC-Annual-Report-2019-2020.Pdf
QUEZON CITY GOVERNMENT Rising Above Adversity Through Better Governance ANNUAL REPORT July 2019 - June 2020 With Special Report on Quezon City’s Covid - 19 Response January - October 2020 QUEZON CITY GOVERNMENT Rising Above Adversity Through Better Governance ANNUAL REPORT July 2019 - June 2020 With Special Report on Quezon City’s Covid -19 Response January - October 2020 Contents I. Message of the Mayor 7 II. Message of the Vice Mayor 11 III. About Quezon City 13 IV. The Quezon City Government Executive Committee 17 V. The 21st City Council 25 VI. The 14-Point Agenda of the Quezon City Government 35 A. Human & Social Services 38 B. Economic Development 57 C. Environment & Climate Change 68 D. Infrastructure 74 E. Institutional Development 87 VII. Special Report on Quezon City’s Covid-19 Response 93 VIII. Financial Highlights 113 IX. Executive Report 119 X. Legislative Report 123 XI. Awards and Recognition 129 XII. Directory 135 Quezon City 2019 ANNUAL REPORT 2020 Quezon City 2019 ANNUAL REPORT 2020 Message of the mayor y first crack at politics happened in high school. I ran for student council president in my senior year. After the winner was proclaimed, my mother Betty Go-Belmonte advised me: “Hold on to the ideals with which MI raised you. Be consumed by love for the people you serve. Value truth and honesty above all else. Fear nobody but God. Live a life of duty and sacrifice.” How is it possible that, despite ideals rooted in “service above self,” politicians have come to acquire such a distasteful reputation? We often see them as persons addicted to power and money, that value their personal interests above all else, fear nothing whatsoever, and enjoy lives of opulence and privilege. -
Bayad Center Name Address
BAYAD CENTER NAME ADDRESS BAYAD CENTER - APEC LIGAO ALBAY POWER AND ENERGY CORP.(APEC), DUNAO, LIGAO BAYAD CENTER - APEC TABACO ALBAY POWER &ENERGY CORP,LLORENTE ST,KINALE,TABACO BAYAD CENTER - BACOLOD COKIN BLDG. LOPEZ JAENA ST.,BACOLOD CITY BAYAD CENTER - BACOOR BACOOR BOULEVARD BRGY. BAYANAN, BACOOR CITY HALL BAYAD CENTER - CABANATUAN 720 MARILYN BLDG., SANGITAN ESTE, CABANATUAN CITY BAYAD CENTER - CEBU CAPITOL 2/F AVON PLAZA BUILDING OSMENA BOULEVARD CAPITOL BAYAD CENTER - CITY OF SAN FERNANDO STALL 3 PUSO ITI AMIANAN BLDG., SEVILLA, CITY OF SAN FERNANDO, LA UNION BAYAD CENTER - DARAGA CORNER ARBOLEDA ST., RIZAL STREET, DARAGA, ALBAY BAYAD CENTER - DAVAO CENTER POINT PLAZA ATRIUM CENTERPOINT PLAZA, MATINA CROSSING BAYAD CENTER - EVER COMMONWEALTH 2ND FLOOR EVER GOTESCO MALL, COMMONWEALTH AVE., QUEZON CITY BAYAD CENTER - GATE2 EAST GATE 2 MERALCO COMPLEX ORTIGAS PASIG BAYAD CENTER - GMA CAVITE GOVERNORS DRVE, BRGY SAN GABRIEL GMA BAYAD CENTER - GULOD 873 QUIRINO HWAY,GULOD,NOVALICHES BAYAD CENTER - KASIGLAHAN MWCI.SAT.OFC KASIGLAHAN VIL.,BRGY.SN JOSE,RODRIGUE BAYAD CENTER - LAKEFRONT REMBRANDT BLDG.LKFRNT BRDWLK,PRESIDIO LKFRNT SUCAT BAYAD CENTER - LCC LEGAZPI 4F LCC MALL, DINAGAAN, LEGAZPI CITY BAYAD CENTER - M. ALVAREZ LAS PI?AS BUS AREA,MARCOS ALVAREZ AVE,TALON SINGKO VENTURE BUILDING, PRIME ST. COR. MARKET ST., MADRIGAL BUSINESS PARK, ALABANG, BAYAD CENTER - MAYNILAD ALABANG MUNTINLUPA CITY BAYAD CENTER - MAYSILO 479-F MAYSILO CIRCLE, BRGY. PLAINVIEW, MANDALUYONG BAYAD CENTER METRO - ALABANG ALABANG TOWN CENTER ALABANG-ZAPOTE ROAD ALABANG, MUNTINLUPA CITY BAYAD CENTER METRO - ANGELES MARQUEE MALL BUILDING, DON BONIFACIO STREET PULUNG MARAGUL, ANGELES CITY BAYAD CENTER METRO - AYALA AYALA CENTER CEBU ARCHBISHOP REYES AVENUE CEBU BUSINESS PARK, CEBU CITY BAYAD CENTER METRO - BANILAD A.S FORTUNA CORNER H. -
University of Cincinnati
UNIVERSITY OF CINCINNATI Date: 24-May-2010 I, Nicole M Fannin , hereby submit this original work as part of the requirements for the degree of: Master of Architecture in Architecture (Master of) It is entitled: bahay sa buhay [from house to life]: exploring architecture's role in informal settlement in Payatas, Philippines Student Signature: Nicole M Fannin This work and its defense approved by: Committee Chair: Nnamdi Elleh, PhD Nnamdi Elleh, PhD Elizabeth Riorden, MARCH Elizabeth Riorden, MARCH Edson Cabalfin, MSArch Edson Cabalfin, MSArch 5/26/2010 713 bahay sa buhay [from house to life]: exploring architecture’s role in informal settlement in Payatas, Philippines A thesis submitted to the Graduate School of the University of Cincinnati in partial fulfillment of the requirements for the degree of MASTER OF ARCHITECTURE in the School of Architecture and Interior Design of the College of Design, Architecture, Art, and Planning June 2010 by Nicole M. Fannin B.A. University of Cincinnati, 2008 Committee Chair: Nnamdi Elleh, Ph.D. Supporting Chairs: Liz Riorden, Edson Cabalfin i PROJECT Abstract In a world where every one out of six people Nowhere are the implications of squatting more is considered a squatter,1 Metro Manila, Philippines is evident in Manila, than in the Payatas area of Quezon City. not alone. There, poverty is characterized by 85,000 Located in the northeastern part of Metro Manila, Payatas families across the city, who build provisional homes and is characterized by the 40 meter (130 ft) garbage dump that communities for themselves on public and private land its residents live and work on, earning about 100 pesos that they do not own.