Development of Cardiovascular System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Embryology and Anatomy of Fetal Heart
Prof. Saeed Abuel Makarem Dr. Jamila El Medany Objectives • By the end of this lecture the student should be able to: • Describe the formation, sit, union divisions of the of the heart tubes. • Describe the formation and fate of the sinus venosus. • Describe the partitioning of the common atrium and common ventricle. • Describe the partitioning of the truncus arteriosus. • List the most common cardiac anomalies. • The CVS is the first major system to function in the embryo. • The heart begins to beat at (22nd – 23rd ) days. • Blood flow begins during the beginning of the fourth week and can be visualized by Ultrasound Doppler Notochord: stimulates neural tube formation Somatic mesoderm Splanchnic mesoderm FORMATION OF THE HEART TUBE • The heart is the first functional organ to develop. • It develops from Splanchnic Mesoderm in the wall of the yolk sac (Cardiogenic Area): Cranial to the developing Mouth & Nervous system and Ventral to the developing Pericardial sac. • The heart primordium is first evident at day 18 (as an Angioplastic cords which soon canalize to form the 2 heart tubes). • As the Head Fold completed, the developing heart tubes change their position and become in the Ventral aspect of the embryo, Dorsal to the developing Pericardial sac. • . Development of the Heart tube • After Lateral Folding of the embryo, the 2 heart tubes approach each other and fuse to form a single Endocardial Heart tube within the pericardial sac. • Fusion of the two tubes occurs in a Craniocaudal direction. What is the • The heart tube grows faster than shape of the the pericardial sac, so it shows 5 alternate dilations separated by Heart Tube? constrictions. -

Te2, Part Iii
TERMINOLOGIA EMBRYOLOGICA Second Edition International Embryological Terminology FIPAT The Federative International Programme for Anatomical Terminology A programme of the International Federation of Associations of Anatomists (IFAA) TE2, PART III Contents Caput V: Organogenesis Chapter 5: Organogenesis (continued) Systema respiratorium Respiratory system Systema urinarium Urinary system Systemata genitalia Genital systems Coeloma Coelom Glandulae endocrinae Endocrine glands Systema cardiovasculare Cardiovascular system Systema lymphoideum Lymphoid system Bibliographic Reference Citation: FIPAT. Terminologia Embryologica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology, February 2017 Published pending approval by the General Assembly at the next Congress of IFAA (2019) Creative Commons License: The publication of Terminologia Embryologica is under a Creative Commons Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0) license The individual terms in this terminology are within the public domain. Statements about terms being part of this international standard terminology should use the above bibliographic reference to cite this terminology. The unaltered PDF files of this terminology may be freely copied and distributed by users. IFAA member societies are authorized to publish translations of this terminology. Authors of other works that might be considered derivative should write to the Chair of FIPAT for permission to publish a derivative work. Caput V: ORGANOGENESIS Chapter 5: ORGANOGENESIS -

MDCT of Interatrial Septum
Diagnostic and Interventional Imaging (2015) 96, 891—899 PICTORIAL REVIEW /Cardiovascular imaging MDCT of interatrial septum ∗ D. Yasunaga , M. Hamon Service de radiologie, pôle d’imagerie, CHU de Caen, avenue de la Côte-de-Nacre, 14033 Caen Cedex 9, France KEYWORDS Abstract ECG-gated cardiac multidetector row computed tomography (MDCT) allows precise Cardiac CT; analysis of the interatrial septum (IAS). This pictorial review provides a detailed description of Interatrial septum; the normal anatomy, variants and abnormalities of the IAS such as patent foramen ovale, con- Patent foramen genital abnormalities such as atrial septal defects as well as tumors and tumoral-like processes ovale; that develop on the IAS. Secundum ASD © 2015 Published by Elsevier Masson SAS on behalf of the Éditions françaises de radiologie. Introduction Major technical advances in computed tomography (CT) in recent years have made it pos- sible to use multidetector row CT (MDCT) in the field of cardiac imaging. Besides coronary arteries, ECG-gated cardiac MDCT provides high-resolution images of all cardiac structures. It is therefore important for radiologists to understand and be able to analyze the normal anatomical structures, variants and diseases of these different structures. This article provides an analysis of the interatrial septum (IAS) based on a pictorial review. After a short embryological and anatomical description, we will illustrate the nor- mal anatomy and variants of the IAS, anomalies such as patent foramen ovale (PFO), congenital diseases such as atrial septal defects (ASD) as well as tumors and tumoral-like processes that develop on the IAS. Abbreviations: ASA, atrial septal aneurysm; ASD, atrial septal defect; ECG, electrocardiogram; IAS, interatrial septum; IVC, inferior vena cava; IVS, interventricular septum; LV, left ventricle; M, myxoma; PFO, patent foramen ovale; RSPV, right superior pulmonary vein; RV, right ventricle; SVC, superior vena cava; MIP, maximal intensity projection; TEE, transesophageal echocardiography; TV, tricuspid valve. -

Transcriptomic Analysis and Developmental Neural Transcript Identification in the Brittle Star Ophioplocus Esmarki
Rochester Institute of Technology RIT Scholar Works Theses 4-27-2020 Transcriptomic Analysis and Developmental Neural Transcript Identification in the Brittle Star Ophioplocus esmarki Alexandria Shumway [email protected] Follow this and additional works at: https://scholarworks.rit.edu/theses Recommended Citation Shumway, Alexandria, "Transcriptomic Analysis and Developmental Neural Transcript Identification in the Brittle Star Ophioplocus esmarki" (2020). Thesis. Rochester Institute of Technology. Accessed from This Thesis is brought to you for free and open access by RIT Scholar Works. It has been accepted for inclusion in Theses by an authorized administrator of RIT Scholar Works. For more information, please contact [email protected]. 1 Transcriptomic Analysis and Developmental Neural Transcript Identification in the Brittle Star Ophioplocus esmarki By Alexandria Shumway A Thesis Submitted in Partial Fulfillment of the Requirements for the Degree of Master of Science in Bioinformatics Thomas H. Gosnell School of Life Sciences College of Science Rochester Institute of Technology Rochester, NY April 27, 2020 Rochester Institute of Technology Thomas H. Gosnell School of Life Sciences Bioinformatics Program 2 To: Head, Thomas H. Gosnell School of Life Sciences The undersigned state that Alexandria Juliana Shumway, a candidate for the Master of Science degree in Bioinformatics, has submitted her thesis and has satisfactorily defended it. This completes the requirements for the Master of Science degree in Bioinformatics at Rochester Institute of Technology. Name Date ____________________________ _______________________________ Dr. Hyla Sweet, Ph.D. Thesis Advisor ____________________________ _______________________________ Dr. Michael Osier, Ph.D. Committee Member ____________________________ _______________________________ Dr. Andre Hudson, Ph.D. Committee Member 3 1 ABSTRACT Ophioplocus esmarki is one species within a family of brittle stars that includes an abbreviated mode of development with a non-feeding, vitellaria larva. -

A 29-Year-Old Man with Acute Onset Blurry Vision, Weakness, and Gait Abnormality
Journal of the Louisiana State Medical Society CLINICAL CASE OF THE MONTH A 29-Year-Old Man With Acute Onset Blurry Vision, Weakness, and Gait Abnormality Deepu Thoppil, MD; Murtuza J. Ali, MD; Neeraj Jain, MD; Sanjay Kamboj, MD; Pramilla Subramaniam, MD; and Fred A. Lopez, MD (Section Editor) A 29-year-old man, with no significant past medical history, was in his usual state of health until the afternoon of admission. The patient was seated at work eating lunch when he suddenly noticed that his vision became blurry. He covered his right eye and had no visual difficulty but noted blurry vision upon covering his left eye. At this point, the patient tried to stand up, but had difficulty walking and noticed he was “falling toward his left.” Facial asymmetry when smiling was also appreciated. The patient denied any alteration in mental status, confusion, antecedent or current headaches, aura, chest pains, or shortness of breath. He was not taking any prescribed medications and had no known allergies. The patient denied any prior hospitalization or surgery. He denied use of tobacco, alcohol, or illicit drugs, and worked as a maintenance worker in a hotel. His family history is remarkable for his father who died of pancreatic cancer in his 50s and his mother who died of an unknown heart condition in her late 40s. Vital signs on presentation to the emergency department included temperature of 97.6oF; respiratory rate of 18 per minute; pulse of 68 per minute; blood pressure of 124/84 mmHg; pulse oximetry of 99% on ambient air. -

Cardiovascular System Heart Development Cardiovascular System Heart Development
Cardiovascular System Heart Development Cardiovascular System Heart Development In human embryos, the heart begins to beat at approximately 22-23 days, with blood flow beginning in the 4th week. The heart is one of the earliest differentiating and functioning organs. • This emphasizes the critical nature of the heart in distributing blood through the vessels and the vital exchange of nutrients, oxygen, and wastes between the developing baby and the mother. • Therefore, the first system that completes its development in the embryo is called cardiovascular system. https://www.slideshare.net/DrSherifFahmy/intraembryonic-mesoderm-general-embryology Mesoderm is one of the three • Connective tissue primary germ layers that • Smooth and striated muscle • Cardiovascular System differentiates early in • Kidneys development that collectively • Spleen • Genital organs, ducts gives rise to all subsequent • Adrenal gland cortex tissues and organs. The cardiovascular system begins to develop in the third week of gestation. Blood islands develop in the newly formed mesoderm, and consist of (a) a central group of haemoblasts, the embryonic precursors of blood cells; (b) endothelial cells. Development of the heart and vascular system is often described together as the cardiovascular system. Development begins very early in mesoderm both within (embryonic) and outside (extra embryonic, vitelline, umblical and placental) the embryo. Vascular development occurs in many places. • Blood islands coalesce to form a vascular plexus. Preferential channels form arteries and veins. • Day 17 - Blood islands form first in the extra-embryonic mesoderm • Day 18 - Blood islands form next in the intra-embryonic mesoderm • Day 19 - Blood islands form in the cardiogenic mesoderm and coalesce to form a pair of endothelial heart tubes Development of a circulation • A circulation is established during the 4th week after the myocardium is differentiated. -

Development of Right Ventricle
DEVELOPMENT OF THE HEART II. David Lendvai M.D., Ph.D. Mark Kozsurek, M.D., Ph.D. • Septation of the common atrioventricular (AV) orifice. • Formation of the interatrial septum. • Formation of the muscular interventricular septum. • Appearance of the membranous interventricular septum and the spiral aorticopulmonary septum. right left septum primum septum primum septum primum septum primum septum primum septum primum foramen primum foramen primum septum primum septum primum foramen primum foramen primum septum primum septum primum foramen secundum foramen secundum foramen primum foramen primum septum primum foramen secundum septum primum foramen secundum foramen primum foramen primum septum primum septum primum foramen secundum foramen secundum septum secundum septum secundum foramen secundum foramen ovale foramen ovale septum primum septum primum septum secundum septum secundum foramen secundum foramen ovale foramen ovale septum primum septum primum septum secundum septum secundum foramen secundum septum primum foramen ovale foramen ovale septum primum SUMMARY • The septation of the common atrium starts with the appearance of the crescent-shaped septum primum. The opening of this septum, the foramen primum, becomes progressively smaller. • Before the foramen primum completly closes, postero-superiorly several small openings appear on the septum primum. These perforations coalesce later and form the foramen secundum. • On the right side of the septum primum a new septum, the septum secundum, starts to grow. The orifice of the septum secundum is the foramen ovale. • Finally two crescent-like, incomplete, partially overlapping septa exist with one hole on each. Septum secundum is more rigid and the septum primum on its left side acts as a valve letting the blood flow exclusively from the right to the left. -
Echocardiographic Follow-Up of Patent Foramen Ovale and the Factors Affecting Spontaneous Closure
Acta Cardiol Sin 2016;32:731-737 Brief Report doi: 10.6515/ACS20160205A Echocardiographic Follow-Up of Patent Foramen Ovale and the Factors Affecting Spontaneous Closure Ali Yildirim,1 Alperen Aydin,2 Tevfik Demir,1 Fatma Aydin,2 Birsen Ucar1 and Zubeyir Kilic1 Background: The aim of the present study was to evaluate the echocardiographic follow-up of patent foramen ovale, which is considered a potential etiological factor in various diseases, and to determine the factors affecting spontaneous closure. Methods: Between January 2000 and June 2012, records of 918 patients with patent foramen ovale were retrospectively reviewed. Patency of less than 3 mm around the fossa ovalis is called patent foramen ovale. Patients with cyanotic congenital heart diseases, severe heart valve disorders and severe hemodynamic left to right shunts were excluded from the study. The patients were divided into three groups based on age; 1 day-1 monthingroup1,1month-12monthsingroup2,andmorethan12monthsingroup3. Results: Of the 918 patients, 564 (61.4%) had spontaneous closure, 328 (35.8%) had patent foramen ovale continued, 15 (1.6%) patients had patent foramen ovale enlarged to 3-5 mm, 6 patients were enlarged to 5-8 mm, and in one patient patent foramen ovale reached to more than 8 mm size. Defect was spontaneously closed in 65.9% of the patients in group 1, 66.7% of the patients in group 2, and 52.3% of the patients in group 3. There was a negative correlation between the age of diagnosis and spontaneous closure (p < 0.05). Gender, prematurity and coexisting malformations such as patent ductus arteriosus and atrial septal aneurysm did not have any effect on spontaneous closure of patent foramen ovale (p > 0.05). -

Persistent Patent Foramen Ovale in Adult Male
Internatiional Journal of Biioassays ISSN: 2278-778X www.ijbio.com Case Report PERSISTENT PATENT FORAMEN OVALE IN ADULT MALE Santhoshkumar N, Kunjumon PC and Anju Balaji More* Department of Anatomy, Sree Mookambika Institute of Medical Sciences, Kulasekharam, Tamilnadu, 629161, India Received for publication: February 17, 2014; Accepted: March 13, 2014 Abstract: In this case report, we want to present a persistent foramen ovale with length of 1.4 cm in an adult male cadaver approximately 60 years of age. The person had a heavy built up and appeared well nourished. The foramen ovale is a normal interatrial communication during fetal life. The persistence of this opening in the later life may go unnoticed if asymptomatic. But symptoms can begin in adult life due to pulmonary hypertension. It will become an added complication to any cardio-vascular disorder developing in later life. With no other anomalous findings in the heart, it appears that the foramen ovale was probe patent. There are five types of foramen ovale according to its location. The present finding belongs to type I that is patent foramen ovale of ostium secundum type. Echocardiogram, Electrocardiogram, Doppler image, Cardiac catheterization, Chest x-ray and MRI of the heart are the various imaging techniques which can detect this variance. Keywords: Atrium, Foramen ovale (Patent oval foramen), Fossa ovalis (Oval fossa). INTRODUCTION An atrial septal defect (ASD) is an opening in made available for the purpose of dissection under the interatrial septum. It allows oxygen rich blood in Anatomy Act. left atrium to mix with oxygen-poor blood in right atrium. -
Primitive Blood Circulation. • Heart Development (Dev. of Heart Tube, Septa and Valves) • Aortal Arches and Their Derivatives
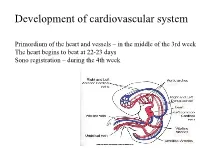
Development of cardiovascular system Primordium of the heart and vessels – in the middle of the 3rd week The heart begins to beat at 22-23 days Sono registration – during the 4th week • Primitive blood circulation. • Heart development (dev. of heart tube, septa and valves) • Aortal arches and their derivatives. • Fetal blood circulation. • Cardiovascular system malformations. Vessels development: (from week 3) hemangiogenesis - blood islands (insulae sanguinae) DAY 15 – 16 in extraembryonic mesoderm of - yolk sac (vasa omphalomesenterica /vitellina/), - connecting stalk and placenta (vasa umbilicalia) DAY 17 – 18 in mesenchyme of embryo Groups of angiogenic cells in mesenchyma ectoderm Blood islet mesenchyme angioblasts endoderm hemoblasts primitive erythrocytes primitive endothelium Differentiation of mesenchymal cells angiogenic cells: - angioblasts endothelium (at the periphery of blood islets) - hemoblasts primitive erythrocytes (in the center of blood islets) angiogenic cells form a "horseshoe-shaped" space between somatic and splanchnic layer of mesoderm = pericardial cavity. Two endothelial tubes arrise in splanchnic mesoderm. The ventral portion with tubes forms the cardiogenic area two heart tubes, while the lateral portions form the dorsal aortae. Cardiogenic region just cranial to the prechordal plate. Fusion of heart tubes mesocardium dorsale diferentiation of heart wall: endocardium ● heart jelly epimyocardium Vitelline, umbilical and intraembryonic vessels fuse together and form the primitive blood circulation ( fetal blood circulation!) Pericardial cavity Cor tubulare simplex Septum transversum branchial arteries 1-6 Right Leftt Desc.aorta Ventral wiew Truncus arteriosus Asc.aorta Sinus venosus right horn degenerate Saccus aorticus Vessels v. cardinalis ant. sin. + v. cardinalis com.sin. cor tubulare Yolk sac v. cardinalis post. sin. aa.omphalomesentericae a. mesenterica sin. -

The Sinus Venosus Typeof Interatrial Septal Defect*
Thorax: first published as 10.1136/thx.13.1.12 on 1 March 1958. Downloaded from Thorax (I9%8), 13, 12. THE SINUS VENOSUS TYPE OF INTERATRIAL SEPTAL DEFECT* BY H. R. S. HARLEY Cardiff (RECEIVED FOR PUBLICATION DECEMBER 30, 1957) Defects of the interatrial septum, other than namely, (1) it lies above and independent of valvular patency of the foramen ovale, are often the fossa ovalis; (2) its margin is incomplete, classified into ostium primum and ostium secun- being absent superiorly and incomplete pos- dum varieties. The relationship of the former type teriorly; and (3) it is associated with anomalous to abnormal development of the atrioventricular drainage of the right superior, and sometimes of canal has been stressed by several workers, includ- the right middle or inferior, pulmonary vein. This ing Rogers and Edwards (1948), Wakai and type of defect is illustrated in Fig. 1 (after Lewis Edwards (1956), Wakai, Swan, and Wood (1956), et al., 1955) and Fig. 2 (after Geddes, 1912). In Brandenburg and DuShane (1956), Toscano- the case reported by Ross (1956), who kindly per- Barbosa, Brandenburg, and Burchell (1956), and mitted me to see the heart, the interatrial Cooley and Kirklin (1956). These workers prefer communication was described as ". lying the term "persistent common within the orifice of atrioventricular the superior vena cava in itscopyright. canal " to "persistent ostium primum." medial wall opposite the mouths of the anomalous In addition to the above types of interatrial pulmonary veins." Ross goes on to say: "On septal defect there is a third variety, which was casual inspection of the interior of the left atrium, described as long ago as 1868 by Wagstaffe, but the defect was not visible unless a search was made which has come into prominence only since the within the superior caval orifice." The relation- http://thorax.bmj.com/ introduction of surgical repair of interatrial ship of the defect to the orifice of the superior communications under direct vision. -

THE CARDIOVASCULAR SYSTEM the Picture Shows the Tranverse Section of the Embryo Demonstrating the Formation of the Angioblastic Cords
EMBRYOLOGY: THE CARDIOVASCULAR SYSTEM The picture shows the tranverse section of the embryo demonstrating the formation of the angioblastic cords . In which region do these cords develop? The picture shows the lateral folding of the embryo and the fusion of the endocardial heart tubes . What is the significance of this folding? This picture shows the formation of cardiac loop . What are the five dilatations which form on the primordial heart tube? . What results in the bending of the heart tube? The picture shows the structure of a primordial heart . Give the three pairs of veins which are received by the sinus nenosus. The picture shows blood circulation through a primordial heart . Describe the circulation of blood through the primordial heart. The picture shows the formation of endocardial cushions . What are endocardial cushions and what is their significance? The picture shows the septation of the atrium in the primordial heart . Give the two septa which are responsible for the formation of the interatrial septa. What results in the perforations denoted by the red arrows? . What results in the formation of foramen primum and foramen secundum? . What is its significance? . What result in the formation of foramen ovale? What is the significance of this foramen? . What structure does formen ovale forms in the adult? The diagram shows the division of the sinus venosus into the left and right horns . Which structure is responsible for this division? . What are the derivatives/remnants of the left horn of the sinus venosus? . What is the fate of the right horn of the sinus venosus? The picture shows the absorption of the pulmonary vein into the left atrium .