Restoring Neurological Function: Putting the Neurosciences to Work in Neurorehabilitation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Brain Research UK Annual Review 2018/20
Brain Research UK Annual review 2018/20 Brain Research UK Welcome to our annual review Our vision is a world where everyone with a neurological One in six of us has a neurological condition. condition lives better, longer Brain Research UK is the leading dedicated funder of neurological research in the UK. We fund the best science to achieve the The brain is the most complex organ in our body. It weighs just 3lb, yet it controls our greatest impact for people affected by neurological conditions, emotions, senses and actions, every single one of them. It is how we process the to help them live better, longer. world around us. So when it breaks down, we break down. Due to a change in our reporting year, this review covers an It doesn’t have to be this way. exceptional, and busy, eighteen month period from October 2018 to March 2020 during which time we awarded grants totalling There are hundreds of neurological conditions. We fund research to discover almost £2.1 million. the causes, develop new treatments and improve the lives of all those affected. We continued our commitment to PhD and project grant funding within our three priority areas of neuro-oncology, acquired brain and spinal cord injury, and headache and facial pain. In addition, we Let’s unite to accelerate the progress of brain research. Today. awarded key funding of over £600,000 from the Graeme Watts Endowment to support Professor Linda Greensmith’s continued research into motor neurone disease at UCL Institute of Neurology. In the following pages, we feature a few stories from our many inspiring supporters. -

Female Fellows of the Royal Society
Female Fellows of the Royal Society Professor Jan Anderson FRS [1996] Professor Ruth Lynden-Bell FRS [2006] Professor Judith Armitage FRS [2013] Dr Mary Lyon FRS [1973] Professor Frances Ashcroft FMedSci FRS [1999] Professor Georgina Mace CBE FRS [2002] Professor Gillian Bates FMedSci FRS [2007] Professor Trudy Mackay FRS [2006] Professor Jean Beggs CBE FRS [1998] Professor Enid MacRobbie FRS [1991] Dame Jocelyn Bell Burnell DBE FRS [2003] Dr Philippa Marrack FMedSci FRS [1997] Dame Valerie Beral DBE FMedSci FRS [2006] Professor Dusa McDuff FRS [1994] Dr Mariann Bienz FMedSci FRS [2003] Professor Angela McLean FRS [2009] Professor Elizabeth Blackburn AC FRS [1992] Professor Anne Mills FMedSci FRS [2013] Professor Andrea Brand FMedSci FRS [2010] Professor Brenda Milner CC FRS [1979] Professor Eleanor Burbidge FRS [1964] Dr Anne O'Garra FMedSci FRS [2008] Professor Eleanor Campbell FRS [2010] Dame Bridget Ogilvie AC DBE FMedSci FRS [2003] Professor Doreen Cantrell FMedSci FRS [2011] Baroness Onora O'Neill * CBE FBA FMedSci FRS [2007] Professor Lorna Casselton CBE FRS [1999] Dame Linda Partridge DBE FMedSci FRS [1996] Professor Deborah Charlesworth FRS [2005] Dr Barbara Pearse FRS [1988] Professor Jennifer Clack FRS [2009] Professor Fiona Powrie FRS [2011] Professor Nicola Clayton FRS [2010] Professor Susan Rees FRS [2002] Professor Suzanne Cory AC FRS [1992] Professor Daniela Rhodes FRS [2007] Dame Kay Davies DBE FMedSci FRS [2003] Professor Elizabeth Robertson FRS [2003] Professor Caroline Dean OBE FRS [2004] Dame Carol Robinson DBE FMedSci -
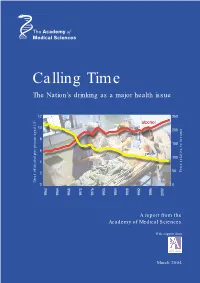
Calling Time the Nation’S Drinking As a Major Health Issue
Calling Time The Nation’s drinking as a major health issue 12 250 10 200 8 150 6 100 4 50 to income Price relative 2 Litres of alcohol per person aged 15+Litres 0 0 1960 1964 1968 1970 1976 1980 1984 1988 1992 1996 2000 A report from the Academy of Medical Sciences With support from March 2004 The independent Academy of Medical Sciences promotes advances in medical science and public health and campaigns to ensure these are translated as quickly as possible into benefits for society. The Academy’s 750 Fellows are the United Kingdom’s leading medical scientists from hospitals, academia, industry and the public service. The aims of the Academy are to: • give national and international leadership in the medical sciences; • promote the application of research to the practice of medicine and to the advancement of human health and welfare; • promote the aims and ethos of medical sciences with particular emphasis on excellence in research and training; • enhance public understanding of the medical sciences and their impact on society; • assess and advise on issues of medical science of public concern. The Academy of Medical Sciences was established in 1998 following the recommendations of a working group chaired by Sir Michael Atiyah, Past President of the Royal Society. There is an elected Council of 22 Fellows that includes the five Officers of the Academy: President Sir Keith Peters, FRS, PMedSci Vice-President (Clinical) Lord Turnberg, FMedSci Vice-President (Non-clinical) Sir John Skehel, FRS, FMedSci Treasurer Sir Colin Dollery, FMedSci Registrar Professor Patrick Vallance, FMedSci The Academy is a registered charity and a company limited by guarantee. -
Neuro Informatics 2015
Neuro NeuroInformatics 2015 Informatics 2015 August 20-22 Cairns,August Australia 20-22 Cairns, Australia ABSTRACT BOOK ABSTRACT BOOK Neuroinformatics 2015 8th INCF Congress Program & abstracts August 20 - 22, 2015 Cairns, Australia Neuroinformatics 2015 3 What is INCF? What is INCF? The International Neuroinformatics Coordinating Facility (INCF), together with its 18 member countries, coordinates collaborative informatics infrastructure for neuroscience and manages scientific programs to develop standards for data sharing, analysis, modeling, and simulation in order to catalyze insights into brain function in health and disease. INCF is an international organization launched in 2005, following a proposal from the Global Science Forum of the OECD to establish international coordination and collaborative informatics infrastructure for neuroscience. INCF is hosted by Karolinska Institutet and the Royal Institute of Technology, and the Secretariat is located on the Karolinska Institute Campus in Solna. INCF currently has 18 member countries across North America, Europe, Australia, and Asia. Each member country establishes an INCF National Node to further the development of Neuroinformatics and to interface with the INCF Secretariat. The mission of INCF is to share and integrate neuroscience data and knowledge worldwide, with the aim to catalyze insights into brain function in health and disease. Learn more: incf.org software.incf.org neuroinformatics2015.org INCF Member Countries as of August 2015 Victoria Node (blue), Australia Node from 1 Jan 2016 (hatched blue) 2 4 Neuroinformatics 2015 Welcome Welcome Welcome to the 8th INCF Congress in Cairns, Australia! The 8th INCF Congress on Neuroinformatics meets this year in sunny Cairns, Australia, home to the Great Barrier Reef. -

Clinical Molecular Genetics in the Uk C.1975–C.2000
CLINICAL MOLECULAR GENETICS IN THE UK c.1975–c.2000 The transcript of a Witness Seminar held by the History of Modern Biomedicine Research Group, Queen Mary, University of London, on 5 February 2013 Edited by E M Jones and E M Tansey Volume 48 2014 ©The Trustee of the Wellcome Trust, London, 2014 First published by Queen Mary, University of London, 2014 The History of Modern Biomedicine Research Group is funded by the Wellcome Trust, which is a registered charity, no. 210183. ISBN 978 0 90223 888 6 All volumes are freely available online at www.history.qmul.ac.uk/research/modbiomed/ wellcome_witnesses/ Please cite as: Jones E M, Tansey E M. (eds) (2014) Clinical Molecular Genetics in the UK c.1975–c.2000. Wellcome Witnesses to Contemporary Medicine, vol. 48. London: Queen Mary, University of London. CONTENTS What is a Witness Seminar? v Acknowledgements E M Tansey and E M Jones vii Illustrations and credits ix Abbreviations xi Ancillary guides xiii Introduction Professor Bob Williamson xv Transcript Edited by E M Jones and E M Tansey 1 Appendix 1 Photograph, with key, of delegates attending The Molecular Biology of Thalassaemia conference in Kolimbari, Crete, 1978 88 Appendix 2 Extracts from the University of Leiden postgraduate course Restriction Fragment Length Polymorphisms and Human Genetics, 1982 91 Appendix 3 Archival material of the Clinical Molecular Genetics Society 95 Biographical notes 101 References 113 Index 131 Witness Seminars: Meetings and Publications 143 WHAT IS A WITNESS SEMINAR? The Witness Seminar is a specialized form of oral history, where several individuals associated with a particular set of circumstances or events are invited to meet together to discuss, debate, and agree or disagree about their memories. -

Part I Officers in Institutions Placed Under the Supervision of the General Board
2 OFFICERS NUMBER–MICHAELMAS TERM 2009 [SPECIAL NO.7 PART I Chancellor: H.R.H. The Prince PHILIP, Duke of Edinburgh, T Vice-Chancellor: 2003, Prof. ALISON FETTES RICHARD, N, 2010 Deputy Vice-Chancellors for 2009–2010: Dame SANDRA DAWSON, SID,ATHENE DONALD, R,GORDON JOHNSON, W,STUART LAING, CC,DAVID DUNCAN ROBINSON, M,JEREMY KEITH MORRIS SANDERS, SE, SARAH LAETITIA SQUIRE, HH, the Pro-Vice-Chancellors Pro-Vice-Chancellors: 2004, ANDREW DAVID CLIFF, CHR, 31 Dec. 2009 2004, IAN MALCOLM LESLIE, CHR, 31 Dec. 2009 2008, JOHN MARTIN RALLISON, T, 30 Sept. 2011 2004, KATHARINE BRIDGET PRETTY, HO, 31 Dec. 2009 2009, STEPHEN JOHN YOUNG, EM, 31 July 2012 High Steward: 2001, Dame BRIDGET OGILVIE, G Deputy High Steward: 2009, ANNE MARY LONSDALE, NH Commissary: 2002, The Rt Hon. Lord MACKAY OF CLASHFERN, T Proctors for 2009–2010: JEREMY LLOYD CADDICK, EM LINDSAY ANNE YATES, JN Deputy Proctors for MARGARET ANN GUITE, G 2009–2010: PAUL DUNCAN BEATTIE, CC Orator: 2008, RUPERT THOMPSON, SE Registrary: 2007, JONATHAN WILLIAM NICHOLLS, EM Librarian: 2009, ANNE JARVIS, W Acting Deputy Librarian: 2009, SUSANNE MEHRER Director of the Fitzwilliam Museum and Marlay Curator: 2008, TIMOTHY FAULKNER POTTS, CL Director of Development and Alumni Relations: 2002, PETER LAWSON AGAR, SE Esquire Bedells: 2003, NICOLA HARDY, JE 2009, ROGER DERRICK GREEVES, CL University Advocate: 2004, PHILIPPA JANE ROGERSON, CAI, 2010 Deputy University Advocates: 2007, ROSAMUND ELLEN THORNTON, EM, 2010 2006, CHRISTOPHER FORBES FORSYTH, R, 2010 OFFICERS IN INSTITUTIONS PLACED UNDER THE SUPERVISION OF THE GENERAL BOARD PROFESSORS Accounting 2003 GEOFFREY MEEKS, DAR Active Tectonics 2002 JAMES ANTHONY JACKSON, Q Aeronautical Engineering, Francis Mond 1996 WILLIAM NICHOLAS DAWES, CHU Aerothermal Technology 2000 HOWARD PETER HODSON, G Algebra 2003 JAN SAXL, CAI Algebraic Geometry (2000) 2000 NICHOLAS IAN SHEPHERD-BARRON, T Algebraic Geometry (2001) 2001 PELHAM MARK HEDLEY WILSON, T American History, Paul Mellon 1992 ANTHONY JOHN BADGER, CL American History and Institutions, Pitt 2009 NANCY A. -

HUMAN GENE MAPPING WORKSHOPS C.1973–C.1991
HUMAN GENE MAPPING WORKSHOPS c.1973–c.1991 The transcript of a Witness Seminar held by the History of Modern Biomedicine Research Group, Queen Mary University of London, on 25 March 2014 Edited by E M Jones and E M Tansey Volume 54 2015 ©The Trustee of the Wellcome Trust, London, 2015 First published by Queen Mary University of London, 2015 The History of Modern Biomedicine Research Group is funded by the Wellcome Trust, which is a registered charity, no. 210183. ISBN 978 1 91019 5031 All volumes are freely available online at www.histmodbiomed.org Please cite as: Jones E M, Tansey E M. (eds) (2015) Human Gene Mapping Workshops c.1973–c.1991. Wellcome Witnesses to Contemporary Medicine, vol. 54. London: Queen Mary University of London. CONTENTS What is a Witness Seminar? v Acknowledgements E M Tansey and E M Jones vii Illustrations and credits ix Abbreviations and ancillary guides xi Introduction Professor Peter Goodfellow xiii Transcript Edited by E M Jones and E M Tansey 1 Appendix 1 Photographs of participants at HGM1, Yale; ‘New Haven Conference 1973: First International Workshop on Human Gene Mapping’ 90 Appendix 2 Photograph of (EMBO) workshop on ‘Cell Hybridization and Somatic Cell Genetics’, 1973 96 Biographical notes 99 References 109 Index 129 Witness Seminars: Meetings and publications 141 WHAT IS A WITNESS SEMINAR? The Witness Seminar is a specialized form of oral history, where several individuals associated with a particular set of circumstances or events are invited to meet together to discuss, debate, and agree or disagree about their memories. The meeting is recorded, transcribed, and edited for publication. -

Science & Policy Meeting Jennifer Lippincott-Schwartz Science in The
SUMMER 2014 ISSUE 27 encounters page 9 Science in the desert EMBO | EMBL Anniversary Science & Policy Meeting pageS 2 – 3 ANNIVERSARY TH page 8 Interview Jennifer E M B O 50 Lippincott-Schwartz H ©NI Membership expansion EMBO News New funding for senior postdoctoral In perspective Georgina Ferry’s enlarges its membership into evolution, researchers. EMBO Advanced Fellowships book tells the story of the growth and ecology and neurosciences on the offer an additional two years of financial expansion of EMBO since 1964. occasion of its 50th anniversary. support to former and current EMBO Fellows. PAGES 4 – 6 PAGE 11 PAGES 16 www.embo.org HIGHLIGHTS FROM THE EMBO|EMBL ANNIVERSARY SCIENCE AND POLICY MEETING transmissible cancer: the Tasmanian devil facial Science meets policy and politics tumour disease and the canine transmissible venereal tumour. After a ceremony to unveil the 2014 marks the 50th anniversary of EMBO, the 45th anniversary of the ScienceTree (see box), an oak tree planted in soil European Molecular Biology Conference (EMBC), the organization of obtained from countries throughout the European member states who fund EMBO, and the 40th anniversary of the European Union to symbolize the importance of European integration, representatives from the govern- Molecular Biology Laboratory (EMBL). EMBO, EMBC, and EMBL recently ments of France, Luxembourg, Malta, Spain combined their efforts to put together a joint event at the EMBL Advanced and Switzerland took part in a panel discussion Training Centre in Heidelberg, Germany, on 2 and 3 July 2014. The moderated by Marja Makarow, Vice President for Research of the Academy of Finland. -

Michaelmas Term 2002 Special No.6 Part I
2 OFFICERS NUMBER–MICHAELMAS TERM 2002 SPECIAL NO.6 PART I Chancellor: H.R.H. The Prince PHILIP, Duke of Edinburgh, T Vice-Chancellor: 1996, Prof. Sir Alec BROERS, CHU, 2003 Deputy Vice-Chancellors: for 2002–2003: A. M. LONSDALE, NH,M.J.GRANT, CL,O.S.O’NEILL, N, Sir ROGER TOMKYS, PEM,D.E.NEWLAND, SE,S.G.FLEET, DOW,G.JOHNSON, W Pro-Vice-Chancellors: 1998, A. M. LONSDALE, NH, 30 June 2004 2001, M. GRANT, CL, 31 Dec. 2004 High Steward: 2001, Dame BRIDGET OGILVIE, G Deputy High Steward: 1983, The Rt Hon. Lord RICHARDSON, CAI Commissary: 2002, Lord MACKAY, T Proctors for 2002–2003: J. D. M ACDONALD, CAI Deputy: D. J. CHIVERS, SE T. N. M ILNER, PET Deputy: V.E. IZZET, CHR Orator: 1993, A. J. BOWEN, JE Registrary: 1997, T. J. MEAD, W Deputy Registrary: 1993, N. J. B. A. BRANSON, DAR Secretary General of the Faculties: 1992, D. A. LIVESEY, EM Treasurer: 1993, J. M. WOMACK, TH Librarian: 1994, P.K. FOX, SE Deputy Librarians: 1996, D. J. HALL, W 2000, A. MURRAY, W Director of the Fitzwilliam Museum and Marlay Curator: 1995, D. D. ROBINSON, M Development Director: 2002, P.AGAR, SE Esquire Bedells: 1996, J. P.EMMINES, PET 1997, J. H. WILLIAMS, HH University Advocate: 1999, N. M. PADFIELD, F, 2003 Deputy University Advocate: 1999, P.J. ROGERSON, CAI, 2003 OFFICERS IN INSTITUTIONS PLACED UNDER THE SUPERVISION OF THE GENERAL BOARD PROFESSORS Accounting Vacant Aeronautical Engineering, Francis Mond 1996 W.N. DAWES, CHU Aerothermal Technology 2000 H. P.HODSON, G African Archaeology 2001 D. -
Restoring Neurological Function: Putting the Neurosciences to Work in Neurorehabilitation
Restoring Neurological Function: Putting the neurosciences to work in neurorehabilitation A report from the Academy of Medical Sciences March 2004 The independent Academy of Medical Sciences promotes advances in medical science and campaigns to ensure these are translated as quickly as possible into benefits for patients. The Academy’s Fellows are the United Kingdom’s leading medical scientists from hospitals, academia, industry and the public service. The aims of the Academy are: • to give national and international leadership in the medical sciences; • to promote the application of research to the practice of medicine and to the advancement of human health and welfare; • to promote the aims and ethos of medical sciences with particular emphasis on excellence in research and training; • to enhance public understanding of the medical sciences and their impact on society; • to assess and advise on issues of medical science of public concern. The Academy of Medical Sciences was established in 1998 following the recommendations of a working group chaired by Sir Michael Atiyah, Past President of the Royal Society. There is an elected Council of 22 Fellows that includes the five Officers of the Academy: President Sir Keith Peters, FRS, PMedSci Vice-President (Clinical) Lord Turnberg, FMedSci Vice-President (Non-clinical) Sir John Skehel, FRS, FMedSci Treasurer Sir Colin Dollery, FMedSci Registrar Professor Patrick Vallance, FMedSci The Academy’s Executive Director is Mrs Mary Manning. For more information about the work of the Academy please see -

Delivering Novel Therapies in the 21St Century Conference Report Held on 24 – 25 October 2018
Part of the conference series Breakthrough science and technologies Transforming our future Delivering novel therapies in the 21st century Conference report Held on 24 – 25 October 2018 Supported by AstraZeneca Delivering novel therapies in the 21st century – Conference report 1 Introduction On 24 – 25 October 2018, the Royal Society and the Academy of Medical Sciences hosted a conference on novel medical therapies. The scientific programme for this meeting was developed by Steve Rees (Vice-President Discovery Biology, AstraZeneca), Professor Molly Stevens FREng (Professor of Biomedical Materials and Regenerative Medicine and Research Director for Biomedical Material Science, Imperial College London), and Sir John Skehel FMedSci FRS (Vice-President and Biological Secretary, the Royal Society). Image: Conference attendees networking. Presentations and discussions outlined recent scientific organised through the Royal Society’s Science and Industry advances in therapeutic modalities and delivery, the programme which demonstrates our commitment to integrate infrastructure required to develop novel treatments, and the science and industry at the Society, promote science and its implications of these advances for policy and healthcare value, build relationships and foster translation. delivery. The conference brought together scientists, technologists and experts from across academia, industry, The Academy’s FORUM programme brings together the NHS and public health, to discuss current challenges in industry, academia and the NHS, and the charity, regulatory human medicine, what future medicines will look like and and wider healthcare sectors. It provides an independent how we can prepare for them. platform for leaders from across the life sciences sector to discuss scientific opportunities, technology trends, This conference, supported by AstraZeneca, forms part of a translational challenges and strategic choices in healthcare. -

80 Stephen Paget Memorial Lecture and Openness Awards Ceremony 5
80th Stephen Paget Memorial Lecture and Openness Awards Ceremony 5th December 2016 Royal College of Physicians, London #ConcordatOpenness Programme 18:00 Arrival and Refreshments 18:30 Welcome Address 18:40 Openness Awards Internal or sector engagement activity Public engagement activity Media engagement or media stories Website or use of new media Individual award 19:00 80th Paget Lecture by Professor Sir Mark Walport Animal Research – Then and Now 20:00 Drinks Reception 21:30 End The Stephen Paget Memorial Lecture The Stephen Paget Memorial Lecture is a scientific lecture to commemorate the life of Dr Stephen Paget. Stephen Paget (1855 – 1926) was the founder of the Research Defence Society, a forerunner of Understanding Animal Research. He believed passionately that better science and understanding of physiology would lead to better medical treatments. After his death in 1926, he was greatly missed by his medical colleagues and the scientific community. The first Stephen Paget memorial lecture was given in 1927 to commemorate his life and allow leading bio-medical scientists of the day to talk about their research. The Openness Awards The Concordat on Openness launched in May 2014 and has to date brought together 109 organisations in a pledge to be more open and transparent about the use of animals in research. This year the Openness Awards celebrate five recipients that have met the Concordat commitments and encouraged the widespread sharing of best practice. Professor Sir Mark Walport, FRS, FMedSci Sir Mark is the Chief Scientific Adviser to HM Government and Head of the Government Office for Science. Previously, Sir Mark was Director of the Wellcome Trust.