Gaston County Community Health Assessment March 2019
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gaston County
LINCO LN COUNTY Gaston County C H E R ER RD R NG Y LI V L SR 1 D IL Hughs Pond E B U D R L D 637 T D To Piedmont O VFD R E T 1638 L T H S Spur R A O R T C R B SR S N 155 E H O 1 R L D B R D RD W 6 T SR 1649 SR 16 E U EL SR 1 E 1 A R Y P X Y E A T 1 H L W 9 H A R C 0 C C R L 3 R H 38 61 B E 6 D N D I 0 S 4 S R K 6 S Q N S 2 K 1 o N S S U L R SR G O R B L D B u R L SR A T E I I R 1 A N E 16 N SR W 18 R HIGH H 50 R t 0 1 L M C R E C h 321 D IS SR 1617 0 20 63 O B K G N F To Piedmont D O H T O H 1 R C ILL AST SH IRON STATION RD D o A R S W O 274 8 N IB L D I Z A A r SR 1637 H H A H P R SR 1002 5 k SHOALS Spur X E SR 1649 L H 2 IG 1 m N L T L RD P o H a T RCH SR 16 S L IN N O C U d C E O H I E 22 r HIGH SHOALS y LN R S L O R 16 L e k 27 COU F R S H v e NTY H T Bicycle D 150 2 a S re COMMUNITY l S E e I C e L C P B P X S PARK R 2 A D H E H R S H A O D 9 R A SR 1 D O IG H Fire Dept L 1 LE K Z O Town Hall I A X A D H A IS L A I H RA L L 820 L C B S H D D E 61 S S SCHOOL ST A 1 I E R Y N H SR G O A Police Station D R 18 H X IA 02 09 R R R R C D SR 1620 8 I T D W H 6 1607 E S U R S 19 D L S S HO L H SR 161 H H CHE P ALS RD About the Routes RR A R G Y ST H R H D L D O O R D IN I A SR E K T 20 L N L A 18 O LV N D S SR L I N S O 2 Alexis VFD R C SR 1 E R C O C S O 20 O W SR W D 16 SR 18 T L C A H Briarcreek 1812 2 H P SR Y N I MAP N T 1 1 D E L U A 165 R L 2 L D A D R 190 1 SR 1622 r L R R S B O Golf Course C O R E The Gaston County bicycle routes were R A S C D C G e L CHERRYVILLE 2 C H X V BLA N H M W O BENJA 7 R SR 1638 I R I N U I e S I L S L -

Career and Technical Education Offerings
Career and Technical Education Offerings Gaston County Schools is dedicated to providing students with a number of CTE programs where students can pursue their interests. Below is a listing of programs available in Gaston County. Ashbrook High School ● Career Management ● Carpentry I ● Carpentry II ● Carpentry III ● Core ● CTE Advanced Studies ● CTE Internship ● Drafting ● Drafting Architectural II ● Drafting Engineering II ● ECommerce ● Electrical I ● Electrical II ● Electrical III ● Entrepreneurship I ● Entrepreneurship II ● Foods ● Foods II ● Health Team Relations ● Health Science I ● Health Science II ● Microsoft Word ● Microsoft Excel ● Multimedia and Web Design ● Nursing Fundamentals ● Personal Finance ● Principles of Business ● Sports Marketing I ● Sports Marketing II ● Teen Living Bessemer City High School ● Career Management ● Carpentry I ● Carpentry II ● Carpentry III ● Core ● CTE Internship ● Early Childhood Ed. I ● Early Childhood Ed. II ● Entrepreneurship ● Health Science ● Health Science II ● Health Team Relations ● Masonry I ● Masonry II ● Masonry III ● Microsoft Word ● Microsoft Excel ● Multimedia and Web Design ● Nursing Fundamentals ● Personal Finance ● Parenting & Child Development ● Principles of Business & Finance Cherryville High School ● Accounting I ● Accounting II ● Career Management ● Carpentry I ● Carpentry II ● Carpentry III ● Core ● CTE Advanced Studies ● CTE Internship ● Entrepreneurship I ● Foods ● Foods II ● Game Art Design ● Health Science I ● Health Science II ● Health Team Relations ● Microsoft Word, -

North-Carolina Ctsos
Career and Technical Student Organizations Serving Career and Technical Education Students in North Carolina 1 As a career educator for more than 30 years in North Carolina and a Career and Technical Student Organization (CTSO) adviser for the majority of these years, I value the impact of CTSOs. DECA, FBLA, FCCLA, FFA, HOSA, Skills USA and TSA provide our students multiple opportunities to network in their field. In high school I developed and excelled in the business skills that led me to choose my career path in college and career. As our students prepare themselves for their future in education or the job market, equipping them to find their career path and to be competitive in the marketplace are two of the many benefits to belonging to a CTSO. I have seen directly how CTSOs have impacted students’ lives in multiple ways. By attending local, regional, state and national events hosted by their CTSOs, our students learn to network socially and professionally and develop leadership skills necessary to succeed in their career field and life. Our goal is for each of our students to be able to compete globally in the 21st century and find gainful employment in their field. CTSOs provide positive opportunities for our students to meet these goals by building leadership, public speaking skills, technical competencies and self-confidence. In North Carolina over 104,000 work-place credentials have been earned by students enrolled in business, health science, marketing, family and consumer science, technology, agriculture, and trade and industry -
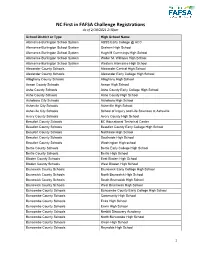
NC First in FAFSA Challenge Registrations As of 2/18/2021 2:30Pm
NC First in FAFSA Challenge Registrations As of 2/18/2021 2:30pm School District or Type High School Name Alamance-Burlington School System ABSS Early College @ ACC Alamance-Burlington School System Graham High School Alamance-Burlington School System Hugh M Cummings High School Alamance-Burlington School System Walter M. Williams High School Alamance-Burlington School System Western Alamance High School Alexander County Schools Alexander Central High School Alexander County Schools Alexander Early College High School Alleghany County Schools Alleghany High School Anson County Schools Anson High School Ashe County Schools Ashe County Early College High School Ashe County Schools Ashe County High School Asheboro City Schools Asheboro High School Asheville City Schools Asheville High School Asheville City Schools School of Inquiry and Life Sciences at Asheville Avery County Schools Avery County High School Beaufort County Schools BC Educational Technical Center Beaufort County Schools Beaufort County Early College High School Beaufort County Schools Northside High School Beaufort County Schools Southside High School Beaufort County Schools Washington High school Bertie County Schools Bertie Early College High School Bertie County Schools Bertie High School Bladen County Schools East Bladen High School Bladen County Schools West Bladen High School Brunswick County Schools Brunswick Early College High School Brunswick County Schools North Brunswick High School Brunswick County Schools South Brunswick High School Brunswick County Schools West -

2020-2021 AIC CIC Certification for North Carolina Page 1 of 15 Run Date
2020-2021 AIC CIC Certification for North Carolina First Name Last Name School AIC CIC steve abernathy No School Affiliation Listed in NFHS Learning Center X Alex Adams Ashbrook High School X Dustin Adams Millbrook High School X X Kaitlyn Adams Ashley High School X Patricia Adolph No School Affiliation Listed in NFHS Learning Center X Kellie AlDriDge Gray's Creek High School X Louis Amigo Emsley A Laney High X X Julee Mae AnDerson No School Affiliation Listed in NFHS Learning Center X Will AnDerson Carolina FrienDs School X X Brian AnDrews South Point HS X Job Armenta West Craven MiDDle X Hunter Armstrong South Point High, Belmont X X Michael ArnolD GolDsboro High X BranDon Arrington Rocky Mount High School X X jeff arthurs Carrboro High X jerry auten North Gaston High School X Joey Autry West BlaDen High School X Kyle Bain Nash Central High School X Christopher Baity East Gaston High X Steven Barbour Terry SanforD High X ToDD Barbour River BenD MiDDle School X Jason Barker Jones Senior High School X X JaDa BarksDale No School Affiliation Listed in NFHS Learning Center X X Burnetta Barnes GolDsboro High X Peter Barney No School Affiliation Listed in NFHS Learning Center X Earl Bates Southeast GuilforD High, Greensboro X BroDie BauDers Christ the King X X Sophie Bauers East Chapel Hill High X Carl Beam HighlanD School Of Technology X Lauren Belch Gates County Senior High X X GLENWOOD BELL WARSAW ELEMENTARY SCHOOL (DUPLIN COUNTY SCHOOLS) X Jonathan Bell RiversiDe High school X William Bell Forbush High, East BenD X X AunDra Belle Durham School of the Arts, Durham X X Alison Bennett Pamlico County High X Jeffrey Berger Panther Creek High School X X Allison Bernauer East Carteret High X William Bethea Rocky Mount High X X Matt Biggy Gates County high school X X Courtney Birch State University of Oswego X Dr. -

Gastonia City Council Meeting May 19, 2015 – 6:00 P.M
Page 169 Page 169 GASTONIA CITY COUNCIL MEETING MAY 19, 2015 – 6:00 P.M. GASTON COUNTY COURTHOUSE PUBLIC FORUM ROOM – GASTONIA, NC Mayor Bridgeman called the meeting to order at 6:00 p.m. on Tuesday, May 19, 2015, in the Gaston County Courthouse Public Forum Room, Gastonia, North Carolina. Councilman Gallagher opened the meeting with prayer and Mayor Bridgeman led the audience in the pledge of allegiance to the flag. Ms. Virginia L. Creighton, City Clerk, recorded the minutes. PRESENT: Mayor John D. Bridgeman Mayor Pro Tem Brenda B. Craig Council Members: David R. Kirlin Walter A. Kimble James Gallagher Todd Pierceall Porter L. McAteer City Manager Edward C. Munn City Attorney L. Ashley Smith ABSENT: None ADOPTION OF THE AGENDA Councilman McAteer made a motion to adopt the agenda as printed. Councilman Pierceall seconded the motion and Council approved it unanimously. AWARDS, CEREMONIES, AND PROMOTIONS COMMITTEE (1) 2015 Student Achievement Awards Councilman Kimble recognized the following recipients of the 2015 Student Achievement Award, and yielded to school personnel for the purpose of introducing and highlighting the accomplishments of each recipient: Mr. Atondi Graham, Southwest Middle School – Introduced by Ms. Rebecca Huffstetler, Principal. Mr. Samuel Boyles – Ashbrook High School – Introduced by Mr. Joey Clinton, Principal. (Reference as contained in Exhibit Book 7 to Minute Book 104 at Page 1.) Mr. Scyler Hanif, Grier Middle School – Introduced by Ms. Loretta Reed, Principal. (Reference as contained in Exhibit Book 7 to Minute Book 104 at Page 2.) Ms. Ashlyn Sawyer, Highland School of Technology – Introduced by Mr. Justin Beam, Assistant Principal. -

Appendix Health Databook
Appendix Health Databook Peer Counties: The table below includes selected health data for Gaston and compares them to person counties and North Carolina. The peer counties were grouped by the University of North Carolina at Charlottes Urban Institute since they have similar-sized populations, economic and social history As former mill communities, are geographically near with four of them in the same region, have similar rural and urban population and similar health status measures. The Urban Institute selected them as a region-wide collaboration and has high credibility and comparing Gaston County with it peers helps to assess improvement in the county’s health. Overall Life Expectancy is slightly lower in Gaston County, Poverty in the past 12 months is slightly higher compared to peer counties but similar to NC and Teen pregnancy is slightly high in Gaston County. Selected Health Indicators, Gaston County, Peer Counties North Carolina Gaston Cabarrus Catawba Davidso Iredell N.C. n Population (2017 Estimates) 220182 206872 157974 165466 175711 10273419 North Carolina (2017) and 75.6 78.0 76.2 76.2 77.3 77.0 County (2015-2017) Life Expectancy at Birth Percent Below Poverty in the 16.5% 11.5% 14.2% 15.8% 12.7 % 16.1% past 12 months (2013-2017) Percent Uninsured (2013- 12.3% 8.9% 11.3% 11.5% 12.3% 12.1% 2017) Teen Pregnancy Rate per 14.0 10.7 11.7 14.1 9.0 14.1 1,000 15-17 Year Olds (2013- 2017) Teen Pregnancy Rate per 33.5 26.5 29.9 31.8 27.1 30.5 1,000 15-19 Year Olds (2013- 2017) Infant (< 1 Year) Mortality 7.1 5.6 7.1 6.2 8.7 7.1 per -

NC First in FAFSA Challenge Registrations 4.1.2021
NC First in FAFSA Challenge Registrations As of 4/1/2021 11apm District (if applicable) High School Name Alamance-Burlington School System ABSS Early College @ ACC Alamance-Burlington School System Graham High School Alamance-Burlington School System Hugh M Cummings High School Alamance-Burlington School System Walter M. Williams High School Alamance-Burlington School System Western Alamance High School Alexander County Schools Alexander Central High School Alexander County Schools Alexander Early College High School Alleghany County Schools Alleghany High School Anson County Schools Anson High School Ashe County Schools Ashe County Early College High School Ashe County Schools Ashe County High School Asheboro City Schools Asheboro High School Asheville City Schools Asheville High School Asheville City Schools School of Inquiry and Life Sciences at Asheville Avery County Schools Avery County High School Beaufort County Schools BC Educational Technical Center Beaufort County Schools Beaufort County Early College High School Beaufort County Schools Northside High School Beaufort County Schools Southside High School Beaufort County Schools Washington High school Bertie County Schools Bertie Early College High School Bertie County Schools Bertie High School Bladen County Schools East Bladen High School Bladen County Schools West Bladen High School Brunswick County Schools Brunswick Early College High School Brunswick County Schools North Brunswick High School Brunswick County Schools South Brunswick High School Brunswick County Schools West -

Laws & Safety Tips Gaston County Detail Maps
Gaston County Detail Maps Laws & Safety Tips Gaston County Gastonia Bessemer City Bicycle Bessemer Bike = Vehicle Basic Traffic Riding Techniques Share the Road Rhyne SIMS EAST Highland Technology Woodhill T BRADLEY WALKING City Elementary 274N MAP S PARK LEGION Elementary PARK Primary Magnet School 85 N TRACK Cars and bicycles frequently must Share BESSEMER In North Carolina, your bicycle is a vehicle and you are A Elementary PARK O Destination and position 1 Riding confidently and skillfully in traffic takes practice M The Road. On roadways with high levels N A Rhynes OR MARSHALL 4 its driver. You share the rights and the duties with all T K Gastonia A E T W Airfield and an understanding of some basic ideas. One of the of bicycle traffic, but relatively demanding D H R Bessemer SENA T O Fire Station D CITY other drivers as you use the State's roadway network. Near intersections, it’s a good idea to let your road position R O S I D O City High most important ideas is road position. Just where you E A ARTHUR RAUCH HWY D V conditions for bicyclists, Share The Road #2 O L M A R tell others where you’re going. T L I S O S A D ride on the roadway depends on several important things: T D signs have been installed. These signs are T R T O R A R T DA SON ST H VID K S E S your speed, the width and condition of the road, and C ERWIN R intended to increase motorists’ awareness IN S H S T S K N A N To turn right, move towards the right edge of the E 1 85 T Z N PARK 9 T S T your destination. -

2020-2021 Unified Champion Schools
2020-2021 Unified Champion Schools Alamance County: Beaufort County: Cabarrus County: Caldwell County: E M Holt Elementary School John Small Elementary School AL Brown High School Baton Elementary School Eastern Alamance High School Washington High School AT Allen Elementary School Caldwell Community College & Technical Elon University Brunswick County: C C Griffin Middle School Collettsville School Hawfields Middle School Bolivia Elementary School Cannon School Dudley Shoals Elementary School Highland Elementary School Cedar Grove Middle School Carl A Furr Elementary School Granite Falls Elementary School Marvin B. Smith Elementary School Jessie Mae Monroe Elementary School Carolina International School Granite Falls Middle School South Graham Elementary School Leland Middle School Charles E Boger Elementary School Hudson Middle School Southern Alamance High School North Brunswick High School Cox Mill High School Sawmills Elementary School Southern Alamance Middle School Shallotte Middle School Forest Park Elementary School West Lenoir Elementary School Walter M. Williams High School South Brunswick High School GW Carver Elementary School William Lenoir Middle School Alexander County: South Brunswick Middle School Harold E. Winkler Middle School Carteret County: Alexander Central High School Supply Elementary School Harris Road Middle School Beaufort Elementary School Alleghany County: Town Creek Elementary School Harrisburg Elementary School Beaufort Middle School Gap Civil Head Start West Brunswick High School Hickory Ridge Elementary -

Report to the North Carolina General Assembly
Public Schools of North Carolina State Board of Education Department of Public Instruction Report to the North Carolina General Assembly Broaden Successful Participation in Advanced Courses SL 2013-360 (SB 402, Budget Bill), sec. 8.27 (h) SL 2014-15, sec. 12 as amended by 2014-15, sec. 49.5 G.S. 115C-174.26 Date Due: December 15, 2017 Report # 27 DPI Chronological Schedule, 2017-2018 STATE BOARD OF EDUCATION SBE VISION: Every public school student will graduate ready for post-secondary education and work, prepared to be a globally engaged and productive citizen. SBE MISSION: The State Board of Education will use its constitutional authority to lead and uphold the system of public education in North Carolina. WILLIAM COBEY BECKY TAYLOR TODD CHASTEEN Chair :: Chapel Hill – At-Large Greenville – Northeast Region Blowing Rock – Northwest Region A.L. COLLINS REGINALD KENAN WAYNE MCDEVITT Vice Chair :: Kernersville – Piedmont Triad Region Rose Hill – Southeast Region Asheville – Western Region DAN FOREST AMY WHITE ERIC DAVIS Lieutenant Governor :: Raleigh – Ex Officio Garner – North Central Region Charlotte – At-Large DALE FOLWELL OLIVIA OXENDINE PATRICIA N. WILLOUGHBY State Treasurer :: Raleigh – Ex Officio Lumberton – Sandhills Region Raleigh – At-Large MARK JOHNSON GREG ALCORN Secretary to the Board :: Raleigh Salisbury – Southwest Region NC DEPARTMENT OF PUBLIC INSTRUCTION Mark Johnson, State Superintendent :: 301 N. Wilmington Street :: Raleigh, North Carolina 27601-2825 In compliance with federal law, the NC Department of Public Instruction administers all state-operated educational programs, employment activities and admissions without discrimination because of race, religion, national or ethnic origin, color, age, military service, disability, or gender, except where exemption is appropriate and allowed by law. -

Comprehensive Property Guide
COMPREHENSIVE PROPERTY GUIDE Please note, Home Partners will only consider purchasing homes which are located within our approved communities. Home Partners is focused on resident affordability and increasing the likelihood of our residents’ success in purchasing the home. We target the broadest group of communities where we think both our residents can succeed and Home Partners can efficiently service their needs. We adjust our investment criteria from time to time in response to market conditions including home price appreciation forecasts, mortgage affordability, population density, and more. The following guide lists our approved high school attendance zones* as of 3/22/19 which can also be found at HomePartners.com/communities. Basic Property Criteria: • Single family home or fee-simple townhome • Located in an approved community • List price between $100,000 and metro's maximum purchase price • Minimum of two above-grade bedrooms on a lot of two acres or less • Traditional sale or FSBO Remember: It is not guaranteed that Home Partners will purchase a home that meets the basic property criteria. Please reference the Property Qualification Criteria guide before submitting a home for review. *Important Note: While high school scholastic ranking is not a factor in our analysis, we utilize high school boundaries as our community outlines. Click the metro area in the chart above to jump to the correct page in this guide. Please contact 877.234.5155 with any questions or for more information. ATLANTA METRO ALLATOONA HIGH SCHOOL HILLGROVE