Management of Iatrogenic Nerve Injuries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Schwann Cell Supplementation in Neurosurgical Procedures After Neurotrauma Santiago R
ll Scienc Ce e f & o T l h a e Unda, J Cell Sci Ther 2018, 9:2 n r a r a p p u u DOI: 10.4172/2157-7013.1000281 y y o o J J Journal of Cell Science & Therapy ISSN: 2157-7013 Review Open Access Schwann Cell Supplementation in Neurosurgical Procedures after Neurotrauma Santiago R. Unda* Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina *Corresponding author: Santiago R. Unda, Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina, Tel: 3804277348; E-mail: [email protected] Rec Date: January 12, 2018, Acc Date: March 13, 2018, Pub Date: March 16, 2018 Copyright: © 2018 Santiago R. Unda. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Nerve trauma is a common cause of quality of life decline, especially in young people. Causing a high impact in personal, psychological and economic issues. The Peripheral Nerve Injury (PNI) with a several grade of axonotmesis and neurotmesis represents a real challenge for neurosurgeons. However, the basic science has greatly contribute to axonal degeneration and regeneration knowledge, making possible to implement in new protocols with molecular and cellular techniques for improve nerve re-growth and to restore motor and sensitive function. The Schwann cell transplantation from different stem cells origins is one of the potential tools for new therapies. In this briefly review is included the recent results of animal and human neurosurgery protocols of Schwann cells transplantation for nerve recovery after a PNI. -

Types and Classification of Nerve Injury: a Review
Indian Journal of Clinical Practice, Vol. 31, No. 5, October 2020 REVIEW ARTICLE Types and Classification of Nerve Injury: A Review R JAYASRI KRUPAA*, KMK MASTHAN†, ARAVINTHA BABU N‡, SONA B# ABSTRACT Nerve injuries are the most common conditions with varying symptoms, depending on the severity, intensity and nerves involved. Though much information is available on the mechanisms of injury and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve injuries and their classification. Keywords: Axonotmesis, neurotmesis, neurapraxia, Wallerian degeneration erve injuries are the most common conditions bundles of fibers called fascicles, which are covered with varying symptoms depending on the by perineurium. severity, intensity and nerves involved. N Â Epineurium: Finally, groups of fascicles are bundled Recovery after any nerve injury is variable. Though together to form the peripheral nerve (such as the much information exists on the mechanisms of injury median nerve), which is covered by epineurium. and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve CLASSIFICATION injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve Classification by Type of Nerve Injury injuries and classification of nerve injuries, which is There are three types of nerve injuries: useful in understanding their pathological basis, and to evaluate the prognosis for recovery. Nerve section Understanding the basic nerve anatomy is important Nerve section can be partial or complete, sharp or for the classification and also essential to evaluate blunt. -
Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography
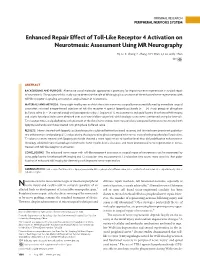
ORIGINAL RESEARCH PERIPHERAL NERVOUS SYSTEM Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography H.J. Li, X. Zhang, F. Zhang, X.H. Wen, L.J. Lu, and J. Shen ABSTRACT BACKGROUND AND PURPOSE: Alternative use of molecular approaches is promising for improving nerve regeneration in surgical repair of neurotmesis. The purpose of this study was to determine the role of MR imaging in assessment of the enhanced nerve regeneration with toll-like receptor 4 signaling activation in surgical repair of neurotmesis. MATERIALS AND METHODS: Forty-eight healthy rats in which the sciatic nerve was surgically transected followed by immediate surgical coaptation received intraperitoneal injection of toll-like receptor 4 agonist lipopolysaccharide (n ϭ 24, study group) or phosphate buffered saline (n ϭ 24, control group) until postoperative day 7. Sequential T2 measurements and gadofluorine M-enhanced MR imaging and sciatic functional index were obtained over an 8-week follow-up period, with histologic assessments performed at regular intervals. T2 relaxation times and gadofluorine enhancement of the distal nerve stumps were measured and compared between nerves treated with lipopolysaccharide and those treated with phosphate buffered saline. RESULTS: Nerves treated with lipopolysaccharide injection achieved better functional recovery and showed more prominent gadofluo- rine enhancement and prolonged T2 values during the degenerative phase compared with nerves treated with phosphate buffered saline. T2 values in nerves treated with lipopolysaccharide showed a more rapid return to baseline level than did gadofluorine enhancement. Histology exhibited more macrophage recruitment, faster myelin debris clearance, and more pronounced nerve regeneration in nerves treated with toll-like receptor 4 activation. -

Wallerian Degeneration and Inflammation in Rat Peripheral Nerve Detected by in Vivo MR Imaging
741 Wallerian Degeneration and Inflammation in Rat Peripheral Nerve Detected by in Vivo MR Imaging DavidS. Titelbaum 1 To investigate the role of MR imaging in wallerian degeneration, a series of animal Joel L. Frazier 2 models of increasingly complex peripheral nerve injury were studied by in vivo MR. Robert I. Grossman 1 Proximal tibial nerves in brown Norway rats were either crushed, transected (neurotomy), Peter M. Joseph 1 or transected and grafted with Lewis rat (allograft) or brown Norway (isograft) donor Leonard T. Yu 2 nerves. The nerves distal to the site of injury were imaged at intervals of 0-54 days after surgery. Subsequent histologic analysis was obtained and correlated with MR Eleanor A. Kassab 1 3 findings. Crush injury, neurotomy, and nerve grafting all resulted in high signal intensity William F. Hickey along the course of the nerve observed on long TR/TE sequences, corresponding to 2 Don LaRossa edema and myelin breakdown from wallerian degeneration. The abnormal signal inten 4 Mark J. Brown sity resolved by 30 days after crush injury and by 45-54 days after neurotomy, when the active changes of wallerian degeneration had subsided. These changes were not seen in sham-operated rats. Our findings suggest that MR is capable of identifying traumatic neuropathy in a peripheral nerve undergoing active wallerian degeneration. The severity of injury may be reflected by the corresponding duration of signal abnormality. With the present methods, MR did not distinguish inflammatory from simple posttraumatic neuropathy. Wallerian degeneration is the axonal degeneration and loss of myelin that occurs when an axon is separated from its cell body. -

Nerve Injury After Peripheral Nerve Block: Allbest Rights Practices Reserved
PRINTER-FRIENDLY VERSION AVAILABLE AT ANESTHESIOLOGYNEWS.COM Nerve Injury After Peripheral Nerve Block: AllBest rights Practices reserved. Reproduction and Medical-Legal in whole or in part without Protection permission isStrategies prohibited. Copyright © 2015 McMahon Publishing Group unless otherwise noted. DAVID HARDMAN, MD, MBA Professor of Anesthesiology Vice Chair for Professional Affairs Department of Anesthesiology University of North Carolina at Chapel Hill Chapel Hill, North Carolina Dr. Hardman reports no relevant financial conflicts of interest. he risk for permanent or severe nerve injury after peripheral nerve blocks (PNBs) is Textremely low, irrespective of its etiology (ie, related to anesthesia, surgery or the patient). The risk inherent in a procedure should always be explicitly discussed with the patient (sidebar, page 4). In fact, it may be better to define this phenomenon ultrasound-guided axillary blocks were used, demon- as postoperative neurologic symptoms (PONS) or peri- strated a very low nerve injury rate of 0.0037% at hos- operative nerve injuries (PNI) in order to help stan- pital discharge.1-7 dardize terminology. Permanent injury rates, as defined A 2009 prospective case series involving more than by a neurologic abnormality present at or beyond 12 7,000 PNBs, conducted in Australia and New Zealand, months after the procedure, have consistently ranged demonstrated that when a postoperative neurologic from 0.029% to 0.2%, although the results of a recent symptom was diagnosed, it was 9 times more likely to multicenter Web-based survey in France, in which be due to a non–anesthesia-related cause than a nerve ANESTHESIOLOGY NEWS • JULY 2015 1 block–related cause.6 On the other hand, it is well doc- PNI rate of 1.7% in patients who received a single-injec- umented in the orthopedic and anesthesia literature tion interscalene block (ISB). -

Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know
Anaesthesia & Critical Care Medicine Journal ISSN: 2577-4301 Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know Kamel I* and Huck E Review Article Lewis Katz School of Medicine at Temple University, USA Volume 4 Issue 3 Received Date: June 20, 2019 *Corresponding author: Ihab Kamel, Lewis Katz School of Medicine at Temple Published Date: August 01, 2019 University, MEHP 3401 N. Broad street, 3rd floor outpatient building ( Zone-B), DOI: 10.23880/accmj-16000155 Philadelphia, United States, Tel: 2158066599; Email: [email protected] Abstract Peripheral nerve injury is a rare but significant perioperative complication. Despite a variety of investigations that include observational, experimental, human cadaveric and animal studies, we have an incomplete understanding of the etiology of PPNI and the means to prevent it. In this article we reviewed current knowledge pertinent to perioperative upper extremity peripheral nerve injury and optimal intraoperative patient positioning. Keywords: Nerve Fibers; Proprioception; Perineurium; Epineurium; Endoneurium; Neurapraxia; Ulnar Neuropathy Abbreviations: PPNI: Perioperative Peripheral Nerve 2018.The most common perioperative peripheral nerve Injury; MAP: Mean Arterial Pressure; ASA CCP: American injuries involve the upper extremity with ulnar Society of Anesthesiology Closed Claims Project; SSEP: neuropathy and brachial plexus injury being the most Somato Sensory Evoked Potentials frequent [3,4]. In this article we review upper extremity PPNI with regards to anatomy and physiology, Introduction mechanisms of injury, risk factors, and prevention of upper extremity PPNI. Perioperative peripheral nerve injury (PPNI) is a rare complication with a reported incidence of 0.03-0.1% [1,2]. Anatomy and Physiology of Peripheral PPNI is a significant source of patient disability and is the Nerves second most common cause of anesthesia malpractice claims [3,4]. -
Development of a Z-Stack Projection Imaging Protocol for a Nerve Allograft
DEVELOPMENT OF A Z-STACK PROJECTION IMAGING PROTOCOL FOR A NERVE ALLOGRAFT by SELVAANISH SELVAM Submitted in partial fulfillment of the requirements for the degree of Master of Science Dissertation Advisor: Dr. George F. Muschler Department of Biomedical Engineering CASE WESTERN RESERVE UNIVERSITY August 2018 CASE WESTERN RESERVE UNIVERSITY SCHOOL OF GRADUATE STUDIES We hereby approve the thesis of Selvaanish Selvam candidate for the degree of (Master of Science) *. Committee Chair Dr. George F. Muschler Committee Member Dr. Eben Alsberg Committee Member Dr. Robert Kirsch Committee Member Cynthia Boehm Date of Defense May 4th 2018 *we also certify that written approval has been obtained For any proprietary material contained therein 2 Table of Contents List of Tables……………………………………………………………………..4 Figures List……………………………………………………………………….5 Acknowledgments………………………………………………………………..6 List of Abbreviations………………………………………………………….....7 Abstract…………………………………………………………………………...8 Introduction……………………………………………………………………..10 Methods………………………………………………………………………….21 Data and Analysis………………………………………………………………31 Conclusions and Future Directions……………………………………………51 References……………………………………………………………………….53 3 List of Tables Table 1: Overall summary of ratios and retention rates……………………..31 Table 2: Selection Ratio for grafts (3X – 10-minute rinse) ………………….35 Table 3: Selection Ratio for grafts (15-minute soak) ………………………...35 4 List of Figures: Figure 1: 2D 10X DAPI stained image using current techniques…….……….9 Figure 2: Peripheral Nerve Anatomy………………………………………….10 -

Restoration of Neurological Function Following Peripheral Nerve Trauma
International Journal of Molecular Sciences Review Restoration of Neurological Function Following Peripheral Nerve Trauma Damien P. Kuffler 1,* and Christian Foy 2 1 Institute of Neurobiology, Medical Sciences Campus, University of Puerto Rico, 201 Blvd. del Valle, San Juan, PR 00901, USA 2 Section of Orthopedic Surgery, Medical Sciences Campus, University of Puerto Rico, San Juan, PR 00901, USA; [email protected] * Correspondence: dkuffl[email protected] Received: 12 January 2020; Accepted: 3 March 2020; Published: 6 March 2020 Abstract: Following peripheral nerve trauma that damages a length of the nerve, recovery of function is generally limited. This is because no material tested for bridging nerve gaps promotes good axon regeneration across the gap under conditions associated with common nerve traumas. While many materials have been tested, sensory nerve grafts remain the clinical “gold standard” technique. This is despite the significant limitations in the conditions under which they restore function. Thus, they induce reliable and good recovery only for patients < 25 years old, when gaps are <2 cm in length, and when repairs are performed <2–3 months post trauma. Repairs performed when these values are larger result in a precipitous decrease in neurological recovery. Further, when patients have more than one parameter larger than these values, there is normally no functional recovery. Clinically, there has been little progress in developing new techniques that increase the level of functional recovery following peripheral nerve injury. This paper examines the efficacies and limitations of sensory nerve grafts and various other techniques used to induce functional neurological recovery, and how these might be improved to induce more extensive functional recovery. -

Painful Abdominal Wall Nerves
CASE REPORT Reconstructive Treatment of Painful Nerves in the Abdominal Wall Using Processed Nerve Allografts Andrew Bi, BS Eugene Park, MD Summary: Neuromas can be a debilitating cause of pain and often negatively af- Gregory A. Dumanian, MD fect patients’ quality of life. One effective method of treatment involves surgical resection of the painful neuroma and use of a processed nerve allograft to repair the injured nerve segment. Giving the nerve “somewhere to go and something to do” has been shown to effectively alleviate pain in upper and lower extremities. We present the first report of this concept to treat a painful neuroma of the ab- dominal wall that developed following a laparoscopic gastric bypass. The neuroma was excised, and the affected nerve was reconstructed using a processed nerve allograft as an interposition graft, with resolution of pain and gradual return of normal sensation. Patient-reported outcomes were measured using the Patient Reported Outcomes Measurement Information System. Neuroma excision with concurrent interposition grafting using processed nerve allografts may be a promising method of treatment for postsurgical painful neuromas of the trunk. Bi et al. (Plast Reconstr Surg Glob Open 2018;6:e1670; doi: 10.1097/GOX.0000000000001670; Published online 6 March 2018.) INTRODUCTION and unacceptable repeat surgical rates.2 And while wrap- Painful neuromas can form following any surgery when ping the distal point of a painful nerve postneuroma exci- nerves are injured due to cautery or traction. Nerve injury sion -

Delayed Facial Palsy After Head Injury
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.40.4.342 on 1 April 1977. Downloaded from Journal ofNeurology, Neurosurgery, andPsychiatry, 1977, 40, 342-350 Delayed facial palsy after head injury K. PUVANENDRAN, M. VITHARANA, AND P. K. WONG From the University Department ofMedicine, and the Department ofOtorhinolaryngology, Singapore General Hospital, Singapore SUMMARY Where facial palsy follows head injury after many days, the mechanism is not clear, and there has been no detailed study on this condition. In this prospective study, an attempt is made to estimate this complication of head injury, and to study its pathogenesis, natural history, prognosis, and sequelae which differ markedly from Bell's palsy. It has a much worse prognosis and so surgical decompression should be considered early in this condition. The facial nerve is the motor cranial nerve which is studies, for prediction of prognosis at a time when most commonly affected in closed head injuries surgical intervention seems most advantageous. (Turner, 1943). In facial palsy which immediately follows a head injury, the mechanism is obvious, but Patients and methods Protected by copyright. it is not clear when the facial palsy follows the head injury after many days (Potter and Braakman, 1976). During the period May 1974-April 1975, there were Traumatic facial palsy has received much attention 6304 cases of head injury admitted to government but few authors distinguish between immediate and hospitals in Singapore. The chief criterion for delayed palsy. admission to hospital was the occurrence of traumatic Turner (1944) studied a selected group of war-time amnesia or unconsciousness, indicating concussion head injuries from a military hospital for head of the brain. -

The Role of Vagal Nerve Root Injury on Respiration Disturbances In
Original Investigation Original Received: 03.12.2013 / Accepted: 11.02.2014 DOI: 10.5137/1019-5149.JTN.9964-13.1 The Role of Vagal Nerve Root Injury on Respiration Disturbances in Subarachnoid Hemorrhage Subaraknoid Kanamada Solunum Bozuklukları Oluşmasında Vagal Sinir Kökü Hasarının Rolü Murteza CAKıR1, Canan AtALAY 2, Zeynep CAKıR3, Mucahit Emet3, Mehmet Dumlu AYDıN1, Nazan AYDıN4, Arif ONDER5, Muhammed CAlıK6 1Ataturk University, School of Medicine, Department of Neurosurgery, Erzurum, Turkey 2Ataturk University, School of Medicine, Department of Anesthesiology and Reanimation, Erzurum, Turkey 3Ataturk University, School of Medicine, Department of Emergency Medicine, Erzurum, Turkey 4Ataturk University, School of Medicine, Department of Psychiatry, Erzurum, Turkey 5Avrasya Hospital, Department of Neurosurgery, Istanbul, Turkey 6Ataturk University, School of Medicine, Department of Pathology, Erzurum, Turkey Corresponding Author: Murteza CAKır / E-mail: [email protected] ABSTRACT AIM: We examined whether there is a relationship between vagal nerve root injury and the severity of respiration disorders associated with subarachnoid hemorrhage (SAH). MaTERIAL and METHODS: This study was conducted on 20 rabbits. Experimental SAH was induced by injecting homologous blood into the cisterna magna. During the experiment, electrocardiography and respiratory rhythms were measured daily. After the experiment, any axonal injury or changes to the arterial nervorums of the vagal nerves were examined. All respiratory irregularities and vagal nerve degenerations were statistically analyzed. RESULTS: Normal respiration rate, as measured in the control group, was 30±6 bpm. In the SAH-induced group, respiration rates were initially 20±4 bpm, increasing to 40±9/min approximately ten hours later, with severe tachypneic and apneic variation. In histopathological examinations, axon density of vagal nerves was 28500±5500 in both control and sham animals, whereas axon density was 22250±3500 in survivors and 16450±2750 in dead SAH animals. -

Repairing Spinal Cord Nerves
Repairing spinal cord nerves Ronald Schnaar The Johns Hopkins School of Medicine Traumatic spinal cord injury Edwin Smith Papyrus, Egypt, circa 1500 BC Earliest medical text on battlefield trauma, in which spinal cord injury was deemed: “An ailment not to be treated” Axon transection in traumatic nerve injury Modified from Brittis and Flanagan, Neuron (2001) 30, 11 Even after a microcrush injury, nerve axons fail to regenerate after injury optic nerve microcrush: Axon retraction Regeneration failure 24 h post-injury 2 wks post-injury 100100 µm µm Selles-Navarro, et al. (2001) Exp. Neurol. 167, 282-289 • The peripheral nervous system (PNS) is more permissive for axon regeneration than the central nervous system (CNS). • When PNS nerve sheath is grafted into a CNS injury, some CNS axons regenerate through the graft Adult Rat CNS axon regeneration David & Aguayo (1981) Science 214, 931-933 In vitro, superior cervical ganglion neurites extend on a surface coated without myelin (P) or on PNS myelin (PR), but not on a surface coated with CNS myelin (CR) Caroni & Schwab (1988) J Cell Biol 106, 1281-1288 Axon transection in traumatic nerve injury Modified from Brittis and Flanagan, Neuron (2001) 30, 11 Multiple axon regeneration inhibitors (ARI’s) accumulate at the site of a CNS injury • Myelin-associated glycoprotein (MAG) – on residual myelin • Nogo – on residual myelin • OMgp – on residual myelin • Chondroitin sulfate proteoglycan (CSPG) – on residual myelin and the astroglial scar Blocking one or more ARI may enhance axon regeneration after