Diffa Region, Niger Health Assessment 21-26 November 2013
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

NIGER - DIFFA : Les Incidents Liés Au Groupe Boko Haram* (1 Janvier Au 31 Août 2018)
NIGER - DIFFA : Les incidents liés au groupe Boko Haram* (1 janvier au 31 août 2018) De janvier à août 2018, la situation sécuritaire dans la région de Diffa a été marquée par une augmentation des exactions des éléments du groupe armé non étatique Boko Haram (BH) et une baisse des victimes civiles liées à ces incidents comparativement à la même période l’année dernière (2017). Les mois de janvier et août 2018 ont enregistré le plus d’incidents (47/94 soit 50%). Les communes de Gueskerou, Bosso, Maine Soroa et Chetimari sont les plus touchées par les attaques du groupe BH (73/94 incidents soit 78%). Des attaques terroristes majeures ont été rapportées dans les localités bordant les berges de la Komadougou et les localités proches des îles du Lac Tchad. Le 4 juin, 3 kamikazes ont fait exploser leurs charges dans un quartier de la ville de Diffa tuant 6 civils. Trois (3) bases militaires ont été attaquées par les éléments du groupe BH respectivement les 17 janvier, 23 janvier et 1 juillet dans les localités de Toumour, Chétima Wangou (Chetimari) et Bilabrin (N’Guigmi) faisant des victimes dans les deux camps. Ces incidents et d’autres de nature criminelle (enlèvements, extorsions et menaces) sont à l’origine de mouvements de populations entre les différents sites et/ou villages. Bilan des incidents Les incidents par commune en 2018 Les incidents par mois 94 incidents de janv. à août 2018 Pertes en vies 38 humaines 60 incidents de janv. à août 2017 (janv. à août 2018) 30 24 23 Pertes en vies 25 56 humaines 20 15 15 (2017) 10 0 5 0 1-5 Enlèvements Ngourti Jui Jul Avr Oct Déc. -
UNHCR Niger Operation UNHCR Database
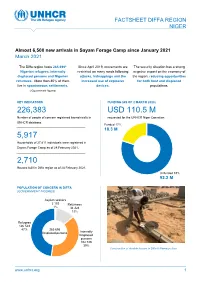
FACTSHEET DIFFA REGION NIGER Almost 6,500 new arrivals in Sayam Forage Camp since January 2021 March 2021 NNNovember The Diffa region hosts 265,696* Since April 2019, movements are The security situation has a strong Nigerian refugees, internally restricted on many roads following negative impact on the economy of displaced persons and Nigerien attacks, kidnappings and the the region, reducing opportunities returnees. More than 80% of them increased use of explosive for both host and displaced live in spontaneous settlements. devices. populations. (*Government figures) KEY INDICATORS FUNDING (AS OF 2 MARCH 2020) 226,383 USD 110.5 M Number of people of concern registered biometrically in requested for the UNHCR Niger Operation UNHCR database. Funded 17% 18.3 M 5,917 Households of 27,811 individuals were registered in Sayam Forage Camp as of 28 February 2021. 2,710 Houses built in Diffa region as of 28 February 2021. Unfunded 83% 92.2 M the UNHCR Niger Operation POPULATION OF CONCERN IN DIFFA (GOVERNMENT FIGURES) Asylum seekers 2 103 Returnees 1% 34 324 13% Refugees 126 543 47% 265 696 Displaced persons Internally Displaced persons 102 726 39% Construction of durable houses in Diffa © Ramatou Issa www.unhcr.org 1 OPERATIONAL UPDATE > Niger - Diffa / March 2021 Operation Strategy The key pillars of the UNHCR strategy for the Diffa region are: ■ Ensure institutional resilience through capacity development and support to the authorities (locally elected and administrative authorities) in the framework of the Niger decentralisation process. ■ Strengthen the out of camp policy around the urbanisation program through sustainable interventions and dynamic partnerships including with the World Bank. -

NIGER: Carte Administrative NIGER - Carte Administrative
NIGER - Carte Administrative NIGER: Carte administrative Awbari (Ubari) Madrusah Légende DJANET Tajarhi /" Capital Illizi Murzuq L I B Y E !. Chef lieu de région ! Chef lieu de département Frontières Route Principale Adrar Route secondaire A L G É R I E Fleuve Niger Tamanghasset Lit du lac Tchad Régions Agadez Timbuktu Borkou-Ennedi-Tibesti Diffa BARDAI-ZOUGRA(MIL) Dosso Maradi Niamey ZOUAR TESSALIT Tahoua Assamaka Tillabery Zinder IN GUEZZAM Kidal IFEROUANE DIRKOU ARLIT ! BILMA ! Timbuktu KIDAL GOUGARAM FACHI DANNAT TIMIA M A L I 0 100 200 300 kms TABELOT TCHIROZERINE N I G E R ! Map Doc Name: AGADEZ OCHA_SitMap_Niger !. GLIDE Number: 16032013 TASSARA INGALL Creation Date: 31 Août 2013 Projection/Datum: GCS/WGS 84 Gao Web Resources: www.unocha..org/niger GAO Nominal Scale at A3 paper size: 1: 5 000 000 TILLIA TCHINTABARADEN MENAKA ! Map data source(s): Timbuktu TAMAYA RENACOM, ARC, OCHA Niger ADARBISNAT ABALAK Disclaimers: KAOU ! TENIHIYA The designations employed and the presentation of material AKOUBOUNOU N'GOURTI I T C H A D on this map do not imply the expression of any opinion BERMO INATES TAKANAMATAFFALABARMOU TASKER whatsoever on the part of the Secretariat of the United Nations BANIBANGOU AZEY GADABEDJI TANOUT concerning the legal status of any country, territory, city or area ABALA MAIDAGI TAHOUA Mopti ! or of its authorities, or concerning the delimitation of its YATAKALA SANAM TEBARAM !. Kanem WANZERBE AYOROU BAMBAYE KEITA MANGAIZE KALFO!U AZAGORGOULA TAMBAO DOLBEL BAGAROUA TABOTAKI TARKA BANKILARE DESSA DAKORO TAGRISS OLLELEWA -
Resident / Humanitarian Coordinator Report on the Use of Cerf Funds Niger Rapid Response Conflict-Related Displacement
RESIDENT / HUMANITARIAN COORDINATOR REPORT ON THE USE OF CERF FUNDS NIGER RAPID RESPONSE CONFLICT-RELATED DISPLACEMENT RESIDENT/HUMANITARIAN COORDINATOR Mr. Fodé Ndiaye REPORTING PROCESS AND CONSULTATION SUMMARY a. Please indicate when the After Action Review (AAR) was conducted and who participated. Since the implementation of the response started, OCHA has regularly asked partners to update a matrix related to the state of implementation of activities, as well as geographical location of activities. On February 26, CERF-focal points from all agencies concerned met to kick off the reporting process and establish a framework. This was followed up by submission of individual projects and input in the following weeks, as well as consolidation and consultation in terms of the draft for the report. b. Please confirm that the Resident Coordinator and/or Humanitarian Coordinator (RC/HC) Report was discussed in the Humanitarian and/or UN Country Team and by cluster/sector coordinators as outlined in the guidelines. YES NO c. Was the final version of the RC/HC Report shared for review with in-country stakeholders as recommended in the guidelines (i.e. the CERF recipient agencies and their implementing partners, cluster/sector coordinators and members and relevant government counterparts)? YES NO The CERF Report has been shared with Cluster Coordinator and recipient agencies. 2 I. HUMANITARIAN CONTEXT TABLE 1: EMERGENCY ALLOCATION OVERVIEW (US$) Total amount required for the humanitarian response: 53,047,888 Source Amount CERF 5,181,281 Breakdown -

5,500 New Arrivals in Sayam Forage Camp 225,118 5,538 1,972 USD 32
FACTSHEET DIFFA REGION 5,500 new arrivals in Sayam Forage Camp October 2020 The Diffa region hosts 265,696* Since April 2019, movements are The security situation has a strong Nigerian refugees, internally restricted on many roads following negative impact on the economy of displaced persons and Nigerien attacks, kidnappings and the the region, reducing opportunities returnees. More than 80% of them increased use of explosive for both host and displaced live in spontaneous settlements. devices. populations. (*Government figures) KEY INDICATORS FUNDING (AS OF 7 OCTOBER) 225,118 USD 32,14 million Number of people of concern registered biometrically in requested for the Nigeria situation in Niger UNHCR database. (Diffa and Maradi regions) Funded 5,538 38% 12,12 million Individuals were registered in Sayam Forage Camp these past three months following a secondary displacement 1,972 As of 31 September 2020, houses have been built in Unfunded Diffa region, 55% of the final target. 62% 20,01 million POPULATION OF CONCERN IN DIFFA (GOVERNMENT FIGURES) Asylum seekers 2 103 Returnees 1% 34 324 13% Refugees 126 543 47% Internally Displaced persons 102 726 39% www.unhcr.org 1 OPERATIONAL UPDATE > Niger - Diffa / October 2020 Update on Achievements Operational Context Population movements and security situation The Diffa region has been hosting Nigerian refugees fleeing terrorist violence in the northern states of Nigeria since 2013. In the wake of the first attacks on Niger soil in 2015, the situation has dramatically deteriorated. In May 2015, the authorities decided to evacuate the population living in the Niger region of the Lake Chad Islands. -
NIGER Community Action Program and Community-Based Integrated Ecosystem Management Project Phase I and II
NIGER Community Action Program and Community-Based Integrated Ecosystem Management Project Phase I and II Report No. 155367 DECEMBER 31, 2020 © 2021 International Bank for Reconstruction and Development / The World Bank 1818 H Street NW Washington DC 20433 Telephone: 202-473-1000 Internet: www.worldbank.org Attribution—Please cite the work as follows: World Bank. 2021. Niger—Community Action Program and Community-Based Integrated Ecosystem Management Project. Independent Evaluation Group, Project Performance Assessment Report 155367. Washington, DC: World Bank. This work is a product of the staff of The World Bank with external contributions. The findings, interpretations, and conclusions expressed in this work do not necessarily reflect the views of The World Bank, its Board of Executive Directors, or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. RIGHTS AND PERMISSIONS The material in this work is subject to copyright. Because The World Bank encourages dissemination of its knowledge, this work may be reproduced, in whole or in part, for noncommercial purposes as long as full attribution to this work is given. Any queries on rights and licenses, including subsidiary rights, should be addressed to World Bank Publications, The World Bank Group, 1818 H Street NW, Washington, DC 20433, USA; fax: 202-522-2625; e-mail: [email protected]. -
Monitoring De Protection
REPUBLIQUE DU NIGER REGION DE DIFFA Cluster Protec�on Niger Agadez GROUPE DE TRAVAIL PROTECTION DIFFA Tahoua Zinder Tillabéri Maradi Niamey Dosso JANVIER 2021 MONITORING DE PROTECTION Communes de Dia, Chétimari, N’guigmi, Gueskerou, © ANDDH, Distribution de Kits NFI par l’UNHCR au profit de 300 ménages victimes de l’incursion Maine-Soroa, Toumour, Kabléwa, Foulatary des GANE à Toumour, 27 janvier 2021 I. APERCU DE L’ENVIRONNEMENT SECURITAIRE ET DE PROTECTION Chiffres globaux - Région de Diffa Janvier 2021 La situation sécuritaire de la région de Diffa est demeurée calme, mais imprévisible en janvier 2021. La tendance au maintien de la pression des éléments des GANE sur les populations 74,621 269,589 civiles et les cibles et objectifs militaires observés déjà en fin d’année 2020, restent d’actualité. ménages individus C’est ainsi que l’après-midi du 13 janvier 2021, entre Djaboulam et Maniram, dans la commune Répartition spatiale des déplacés de Bosso, de violents affrontements ont opposé deux (02) factions rivales des GANE, avec plusieurs morts. Les rescapés se seraient cachés non loin de Garin Wanzam, dans la commune de Gueskerou. Ce même jour, un (01) piroguier et deux (02) techniciens de la Compagnie de téléphonie mobile Airtel ont été enlevés à Gueskerou, de retour d’une mission d’entretien. La problématique des engins explosifs improvisés (EEI) se pose avec autant d’acuité que les N’Gourti 709 mois précédents. En témoigne les deux (02) incidents d’envergure survenus au cours du mois de rapportage. En effet, alors qu’ils s’étaient lancés à la poursuite des auteurs d’une incursion Foulatari contre le poste militaire de Chetima Wangou dans la commune de Chétimari, des éléments des 348 N’Guel Beyli Nguigmi forces de défense et de sécurité (FDS) sont tombés sur un engin explosif improvisé (EEI) dans 893 Kablewa 33,446 15,432 l’après- midi du 18 janvier 2021. -

Niger Food Security Brief
NIGER FOOD SECURITY BRIEF MAY 2014 Niger Food Security Brief This publication was prepared by Meredith Sisa under the United States Agency for International Development Famine Early Warning Systems Network (FEWS NET) Indefinite Quantity Contract, AID-OAA-I-12-00006. The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government. Photo credit: Peter Thomas, FEWS NET Page 2 Niger Food Security Brief Introduction Over the last three decades, FEWS NET has steadily built a core set of integrated materials on livelihoods, household vulnerability, nutrition, trade, and agro- climatology through fieldwork and secondary data collection and research. FEWS NET also looks beyond the immediate context to understand the broader context and the underlying causes of food insecurity. This Food Security Brief draws on FEWS NET research and an array of other sources to provide an overview of the food security context and the main determinants of chronic and acute food insecurity, and highlight areas or livelihood zones at most risk of food insecurity. It is a starting ABOUT point for anyone seeking a deep understanding of the range of factors influencing food security in Niger. F E W S N E T The brief is organized around the FEWS NET Household Livelihoods Analytical Created in response to Framework (Figure 1), which looks at underlying and proximate causes of food the 1984 famines in insecurity as a means to inform outcomes at the regional and household levels. At East and West Africa, the core of this analysis is an understanding of hazards and their magnitude and the Famine Early extent, household vulnerability to hazards, and coping capacity in response. -

Multi-Sectoral Support to Vulnerable Households in Diffa, Niger (Agreement No: 720FDA18GR00280)
Multi-sectoral support to vulnerable households in Diffa, Niger (Agreement No: 720FDA18GR00280) INTERNATIONAL RESCUE COMMITTEE NIGER SEMI-ANNUAL REPORT Multi-sectoral support to vulnerable households in Diffa, Niger AGREEMENT NO: 720FDA18GR00280 REPORTING PERIOD: AUGUST 1, 2018- MARCH 31, 2019 PRESENTED TO: THE USAID OFFICE OF FOREIGN DISASTER ASSISTANCE Collaborating Partner: Agency Headquarters: International Rescue Committee Niger International Rescue Committee c/o Giorgio Faedo, Country Director c/o Amelia Hays, Program Officer Tel: +227 92 18 74 01 Tel : 212.551.0954 E-mail: [email protected] E-mail: [email protected] SUBMITTED: MAY 1, 2019 Multi-sectoral support to vulnerable households in Diffa, Niger (Agreement No: 720FDA18GR00280) I. Executive Summary PROGRAM TITLE: Multi-sectoral support to vulnerable households in Diffa, Niger AGREEMENT: 720FDA18GR00280 AGENCY: International Rescue Committee in Niger CAUSE: WASH, protection, food security, shelter and NFI PROJECT PERIOD: 12 months (August 1, 2018 – July 31, 2019) OBJECTIVE: Improve the living conditions and build the resilience of vulnerable households in Diffa region, through emergency and early recovery interventions in the WASH, protection, food security, shelter, and NFI sectors BENEFICIARIES: Total number of beneficiaries targeted: 26,280 direct beneficiaries, including 14,580 IDPs Total number of beneficiaries reached to date: 15,359 beneficiaries, including 8,728 IDPs LOCATION: Region of Diffa, Niger WASH: Diffa, Maïné Soroa, and Goudoumaria departments Protection: N’Guigmi, Bosso, Diffa, Maïné Soroa, and Goudoumaria departments Agriculture and Food Security: N’Gourti, Diffa, Maïné Soroa, and Goudoumaria departments Shelter and Settlements: Diffa department 1 Multi-sectoral support to vulnerable households in Diffa, Niger (Agreement No: 720FDA18GR00280) I. -

1 EVALUATION DU 8Ème PROGRAMME DE PAYS UNFPA
REPUBLIQUE DU NIGER Fonds des Nations Unies pour la Population EVALUATION DU 8ème PROGRAMME DE PAYS UNFPA/NIGER 2014-2018 Période évaluée : 1er Janvier 2014 — 30 Juin 2017 RAPPORT FINAL D’EVALUATION Juin 2018 1 Page 1 Equipe d’évaluation Chef de mission, Consultant International, Thématique SSR Tiburce NYIAMA Consultant National, Thématique Population & Harouna HAMIDOU Développement Exception : Le contenu de ce rapport ne reflete pas nécessairement l’opinion de l’UNFPA. Il s’agit de l’appréciation des consultants suite à l’analyse des données et évidences collectées. 2 Page 2 REMERCIEMENTS Des acteurs nationaux et internationaux ont contribué à l’évaluation finale du 8ème Programme de coopération entre l’UNFPA et l’Etat du Niger. L’équipe d’évaluation reconnaît au Bureau Pays de l’UNFPA au Niger et aux membres du Groupe de Référence de l’Evaluation l’accompagnement continu apporté. Une appréciation particulière va à l’endroit de M. le Représentant Résident, Dr. Nestor Azandegbe, de l’Assistant Représentant Résident et Coordinateur du Programme, M. Hassane Ali et du Chargé de Programme Suivi et Evaluation, M. Abdoul Razaou Issa pour la qualité de leur investissement en vue du succès de l’évaluation. M. Simon-Pierre Tegang, Conseiller Technique en Suivi et Evaluation au bureau Régional de l’UNFPA pour l’Afrique de l’Ouest et du Centre à Dakar/Sénégal, a apporté l’assistance technique nécessaire. L’obligeance de l’équipe d’évaluation va aussi à l’endroit des 7 Ministères en charge de la Santé, de la Jeunesse, du Genre, de la population, de l’enseignement secondaire, de la formation professionnelle et technique et du Plan, l’ENESP D. -
UNFPA–UNICEF Global Programme to End Child Marriage
NIGER COUNTRY PROFILE UNFPA–UNICEF Global Programme to End Child Marriage Dejongh © UNICEF/UN0317837/Frank NIGER COUNTRY PROFILE 0% Niger is home to 5 10% million child brides. 20% Of these, 1.9 million 30% married before age 15. 40% 50% Source: UNICEF global databases, 2020. Demographic data are 5 million 60% from United Nations, Department Married before age 18 of Economic and Social Affairs, 70% Population Division (2019). World Population Prospects 2019, Online 80% Edition. Rev. 1. 90% Notes: For details on the calculation of girls and women married in 100% childhood, see: United Nations Children’s Fund, Child Marriage: Latest trends and future prospects, Percentage of women aged 20 to 24 years who were first married UNICEF, New York, 2018. Estimates or in union before age 18 refer to population year 2019. Values below 2 million are rounded to 1.9 million Note: This map is stylized and not to scale. It does not reflect a position by UNFPA the nearest hundred thousand; those or UNICEF on the legal status of any country or area or the delimitation of any Married before age 15 above 2 million are rounded to the frontiers. Source for child marriage prevalence data is the Niger Demographic and nearest million. Health Survey 2012. Before age 15 Before age 18 Percentage of women 100 aged 20 to 24 years 90 84 who were first married 80 76 or in union before age 15 and before age 18 70 60 Source: Niger Demographic and Health Survey 2012 50 Note: This trend analysis is based on the prevalence of child marriage 40 across age cohorts, as measured in 34 the latest available survey. -
Niger 2020 Human Rights Report
NIGER 2020 HUMAN RIGHTS REPORT EXECUTIVE SUMMARY Niger is a multiparty republic. In the first round of the presidential elections on December 27, Mohamed Bazoum of the ruling coalition finished first with 39.3 percent of the vote. Opposition candidate Mahamane Ousman finished second with 16.9 percent. A second round between the two candidates was scheduled for February 21, 2021. President Mahamadou Issoufou, who won a second term in 2016, was expected to continue in office until the second round was concluded and the winner sworn into office. International and domestic observers found the first round of the presidential election to be peaceful, free, and fair. In parallel legislative elections also conducted on December 27, the ruling coalition preliminarily won 80 of 171 seats, and various opposition parties divided the rest, with several contests still to be decided. International and local observers found the legislative elections to be equally peaceful, free, and fair. The National Police, under the Ministry of Interior, Public Security, Decentralization, and Customary and Religious Affairs (Ministry of Interior), is responsible for urban law enforcement. The Gendarmerie, under the Ministry of National Defense, has primary responsibility for rural security. The National Guard, also under the Ministry of Interior, is responsible for domestic security and the protection of high-level officials and government buildings. The armed forces, under the Ministry of National Defense, are responsible for external security and, in some parts of the country, for internal security. Every 90 days the parliament reviews the state of emergency declaration in effect in the Diffa Region and in parts of Tahoua and Tillabery Regions.