Hearing Loss
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Underwater Acoustics: Webinar Series for the International Regulatory Community
Underwater Acoustics: Webinar Series for the International Regulatory Community Webinar Outline: Marine Animal Sound Production and Reception Thursday, December 3, 2015 at 12:00pm (US East Coast Time) Sound production and reception in teleost fish (M. Clara P. Amorim, Ispa – Instituto Universitário) • Teleost fish are likely the largest vocal vertebrate group. Sounds made by fish can be an important part of marine soundscapes. • Fish possess the most diversified sonic mechanisms among vertebrates, which include the vibration of the swim bladder through intrinsic or extrinsic sonic muscles, as well as the rubbing of bony elements. • Fish sounds are usually pulsed (each sonic muscle contraction corresponds to a sound pulse), short (typically shorter than 1 s) and broadband (with most energy below 1 kHz), although some fish produce tonal sounds. Sounds generated by bony elements are often higher frequency (up to a few kHz). • In contrast with terrestrial vertebrates, fish have no external or middle ear. Fish detect sounds with the inner ear, which comprises three semicircular canals and three otolithic end organs, the utricle, the saccule and the lagena. Fish mostly detect particle motion and hear up to 1 kHz. Some species have evolved accessory auditory structures that serve as pressures transducers and present enhanced hearing sensitivity and increased frequency detection up to several kHz. Fish hearing seems to have evolved independently of sound production and is important to detect the ‘auditory scene’. • Acoustic signals are produced during social interactions or during distress situations as in insects or other vertebrates. Sounds are important in mate attraction, courtship and spawning or to defend a territory and gain access to food. -

Advance and Unedited Reporting Material (English Only)
13 March 2018 (corr.) Advance and unedited reporting material (English only) Seventy-third session Oceans and the law of the sea Report of the Secretary-General Summary In paragraph 339 of its resolution 71/257, as reiterated in paragraph 354 of resolution 72/73, the General Assembly decided that the United Nations Open-ended Informal Consultative Process on Oceans and the Law of the Sea would focus its discussions at its nineteenth meeting on the topic “Anthropogenic underwater noise”. The present report was prepared pursuant to paragraph 366 of General Assembly resolution 72/73 with a view to facilitating discussions on the topic of focus. It is being submitted for consideration by the General Assembly and also to the States parties to the United Nations Convention on the Law of the Sea, pursuant to article 319 of the Convention. Contents Page I. Introduction ............................................................... II. Nature and sources of anthropogenic underwater noise III. Environmental and socioeconomic aspects IV. Current activities and further needs with regard to cooperation and coordination in addressing anthropogenic underwater noise V. Conclusions ............................................................... 2 I. Introduction 1. The marine environment is subject to a wide array of human-made noise. Many human activities with socioeconomic significance introduce sound into the marine environment either intentionally for a specific purpose (e.g., seismic surveys) or unintentionally as a by-product of their activities (e.g., shipping). In addition, there is a range of natural sound sources from physical and biological origins such as wind, waves, swell patterns, currents, earthquakes, precipitation and ice, as well as the sounds produced by marine animals for communication, orientation, navigation and foraging. -

Large Scale Sound Installation Design: Psychoacoustic Stimulation
LARGE SCALE SOUND INSTALLATION DESIGN: PSYCHOACOUSTIC STIMULATION An Interactive Qualifying Project Report submitted to the Faculty of the WORCESTER POLYTECHNIC INSTITUTE in partial fulfillment of the requirements for the Degree of Bachelor of Science by Taylor H. Andrews, CS 2012 Mark E. Hayden, ECE 2012 Date: 16 December 2010 Professor Frederick W. Bianchi, Advisor Abstract The brain performs a vast amount of processing to translate the raw frequency content of incoming acoustic stimuli into the perceptual equivalent. Psychoacoustic processing can result in pitches and beats being “heard” that do not physically exist in the medium. These psychoac- oustic effects were researched and then applied in a large scale sound design. The constructed installations and acoustic stimuli were designed specifically to combat sensory atrophy by exer- cising and reinforcing the listeners’ perceptual skills. i Table of Contents Abstract ............................................................................................................................................ i Table of Contents ............................................................................................................................ ii Table of Figures ............................................................................................................................. iii Table of Tables .............................................................................................................................. iv Chapter 1: Introduction ................................................................................................................. -

The Audiogram
Recently,Recently, I’veI’ve been trying to orga- evaluations, and they are truly im- nize some of the columns and articles pressive, the information and insights RI’veI’ve written overover the past ten years.years. provided by the simple audiogram As I was looking through them, it be- can still provide the most pertinent came apparent that I’ve neglected to information to explain the behavioral discuss what is perhaps the implications of a hearing loss. most important hearing di- Perhaps the most important in- mension of all, the simple sight of all is an appreciation of how The audiogram. specifi c audiograms impact upon the In reality, however, perception of certain speech sounds. the “simple” audiogram, Without including speech in the Audiogram: and particularly its im- equation, it is simply not possible to Audiogram: plications, is not quite so intelligibly discuss the audiogram. simple. Even though just This, after all, is the signal we are about everybody who re- most interested in hearing (not to Explanation ceives a hearing aid has his minimize the specifi c needs of certain or her hearing tested with groups of people for other types of a pure-tone audiometer, sounds, such as musicians). and not everybody receives a comprehensive explanation Figure One Audiogram — of exactly what the results The “Speech Banana” Signifi cance mean and what the impli- cations are for them. The audiogram of a fairly typical And even for those who audiogram can be seen in Figure 1. do, at a time when prospec- (My thanks to Brad Ingrao for creat- By Mark Ross tive hearing aid purchasers ing these fi gures for me.) Let’s fi rst go are being inundated with through the fundamentals. -

Appendix J Fish Hearing and Sensitivity to Acoustic
APPENDIX J FISH HEARING AND SENSITIVITY TO ACOUSTIC IMPACTS Fish Hearing and Sensitivity to Acoustic Impacts J-iii TABLE OF CONTENTS Page 1. INTRODUCTION ............................................................................................................................ J-1 1.1. What is Injury for Fishes?........................................................................................................ J-1 1.2. Fish........................................................................................................................................... J-1 1.3. Fish Bioacoustics – Overview.................................................................................................. J-2 1.4. Metrics of Sound Exposure...................................................................................................... J-2 2. BACKGROUND ON FISH HEARING........................................................................................... J-3 2.1. Sound in Water ........................................................................................................................ J-3 2.2. Hearing Sensitivity................................................................................................................... J-3 2.3. Other Aspects of Fish Hearing................................................................................................. J-7 3. EFFECTS OF HUMAN-GENERATED SOUND ON FISHES – OVERVIEW ............................. J-8 4. EFFECTS OF ANTHROPOGENIC SOUNDS ON HEARING ..................................................... -
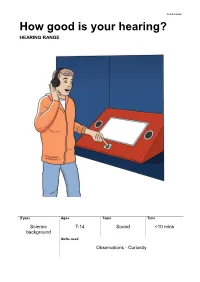
How Good Is Your Hearing? HEARING RANGE
Exhibit Sheet How good is your hearing? HEARING RANGE (Type) Ages Topic Time Science 7-14 Sound <10 mins background Skills used Observations - Curiosity Overview for adults Hearing Range lets you test your hearing. As you listen through headphones, sounds of different frequencies are played, starting quietly and getting louder. You press a button when you hear the sound and at the end get an estimate of your “hearing age”. What’s the science? Frequency is the number of sound waves per second. It’s measured in hertz (Hz). Humans can hear sounds at frequencies between 20 hertz (a cat purring) and 20,000 hertz (a bat squeaking). The sounds you can hear are linked to your age. An 8-year-old hears the widest range of sounds. Then, as you get older, it becomes harder to hear high-frequency sounds. Science in your world Different animals have different hearing ranges. Dogs and cats can hear much higher sounds than we can – up to 50,000hz. That’s why dog whistles work. They produce really high frequency sounds that we can’t hear but dogs can hear them loud and clear. Things to think and talk about … Why do you think hearing gets worse as you get older? What could make your hearing better or worse? Things to investigate … How good is your hearing? Who the best hearing in your group? Are they the youngest? Museum links When microphones were invented, they could only pick up small ranges of frequencies. To record people speaking, you needed lots of different microphones of different sizes – from tiny ones to pick up high frequency sounds to big ones to pick up the low frequency sounds. -
Audiology 101: an Introduction to Audiology for Nonaudiologists Terry Foust, Aud, FAAA, CC-SLP/A; & Jeff Hoffman, MS, CCC-A
NATIONALA RESOURCE CENTER GUIDE FOR FOR EARLY HEARING HEARING ASSESSMENT DETECTION & & MANAGEMENT INTERVENTION Chapter 5 Audiology 101: An Introduction to Audiology for Nonaudiologists Terry Foust, AuD, FAAA, CC-SLP/A; & Jeff Hoffman, MS, CCC-A Parents of young Introduction What is an audiologist? children who are arents of young children who are An audiologist is a specialist in hearing identified as deaf or hard identified as deaf or hard of hearing and balance who typically works in of hearing (DHH) are P(DHH) are suddenly thrust into a either a medical, private practice, or an suddenly thrust into a world of new concepts and a bewildering educational setting. The primary roles of world of new concepts array of terms. What’s a decibel or hertz? an audiologist include the identification and a bewildering array What does sensorineural mean? Is a and assessment of hearing and balance moderate hearing loss one to be concerned problems, the habilitation or rehabilitation of terms. about, since it’s only moderate? What’s of hearing and balance problems, and the a tympanogram or a cochlear implant? prevention of hearing loss. When working These are just a few of the many questions with infants and young children, the that a parent whose child has been primary focus of audiology is hearing. identified as DHH may have. In addition to parents, questions also arise from Audiologists are licensed by the state in professionals and paraprofessionals who which they practice and may be members work in the field of early hearing detection of the American Speech-Language- and intervention (EHDI) and are not Hearing Association (ASHA), American audiologists. -

A Comparison of Behavioral and Auditory Brainstem Response
A Dissertation entitled A Comparison of Behavioral and Auditory Brainstem Response Measures of Hearing in the Laboratory Rat (Rattus norvegicus) By Evan M. Hill Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Doctor of Philosophy Degree in Psychology ________________________________________ ______________ Dr. Henry Heffner, Committee Chair ______________________________________ ________________ Dr. Harvard Armus, Committee Member ______________________________________________________ Dr. Stephen Christman, Committee Member ______________________________________________________ Dr. Kamala London, Committee Member ______________________________________________________ Dr. Lori Pakulski, Committee Member ______________________________________________________ Dr. Patricia R. Komuniecki, Dean College of Graduate Studies The University of Toledo December 2011 i ii An Abstract of A Comparison of Behavioral and Auditory Brainstem Response Measures of Hearing in the Laboratory Rat (Rattus norvegicus) by Evan M. Hill Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Doctor of Philosophy Degree in Psychology The University of Toledo December 2011 The basic measure of an animal‘s hearing is the behavioral, pure-tone audiogram, which shows an animal‘s sensitivity to pure tones throughout its hearing range. Because obtaining a behavioral audiogram on an animal can take months, the tone-evoked auditory brainstem response (ABR) is often used instead to obtain thresholds. Although the tone-evoked ABR is obtained quickly and with relative ease, it does not accurately reflect an animal‘s behavioral sensitivity to pure tones. Because several lines of evidence suggested that using narrow-band noise to evoke the ABR might give a more accurate measure, ABR thresholds evoked by one-octave noise bands and short-duration tones (tone pips) were compared in rats to determine which most closely estimated the animals‘ behavioral, pure-tone thresholds. -

Audiology Staff At
3rd Edition contributions from and compilation by the VA Audiology staff at Mountain Home, Tennessee with contributions from the VA Audiology staffs at Long Beach, California and Nashville, Tennessee Department of Veterans Affairs Spring, 2009 TABLE OF CONTENTS Preface ...................................................................................................................... iii INTRODUCTION ..............................................................................................................1 TYPES OF HEARING LOSS ...........................................................................................1 DIAGNOSTIC AUDIOLOGY ............................................................................................3 Case History ...............................................................................................................3 Otoscopic Examination ..............................................................................................3 Pure-Tone Audiometry ...............................................................................................3 Masking ......................................................................................................................6 Audiometric Tuning Fork Tests ..................................................................................6 Examples of Pure-Tone Audiograms ........................................................................7 Speech Audiometry ....................................................................................................8 -

Short- and Long-Term Monitoring of Underwater Sound Levels in the Hudson River (New York, USA)
Short- and long-term monitoring of underwater sound levels in the Hudson River (New York, USA) S. Bruce Martina) JASCO Applied Sciences, 32 Troop Avenue, Suite 202, Dartmouth, Nova Scotia B3B 1Z1, Canada Arthur N. Popper Department of Biology, University of Maryland, College Park, Maryland 20742, USA (Received 20 June 2015; revised 22 January 2016; accepted 15 March 2016; published online 18 April 2016) There is a growing body of research on natural and man-made sounds that create aquatic soundscapes. Less is known about the soundscapes of shallow waters, such as in harbors, rivers, and lakes. Knowledge of soundscapes is needed as a baseline against which to determine the changes in noise levels resulting from human activities. To provide baseline data for the Hudson River at the site of the Tappan Zee Bridge, 12 acoustic data loggers were deployed for a 24-h period at ranges of 0–3000 m from the bridge, and four of the data loggers were re-deployed for three months of continu- ous recording. Results demonstrate that this region of the river is relatively quiet compared to open ocean conditions and other large river systems. Moreover, the soundscape had temporal and spatial diversity. The temporal patterns of underwater noise from the bridge change with the cadence of human activity. Bridge noise (e.g., road traffic) was only detected within 300 m; farther from the bridge, boating activity increased sound levels during the day, and especially on the weekend. Results also suggest that recording near the river bottom produced lower pseudo-noise levels than previous studies that recorded in the river water column. -

THE AUDITORY RANGE of a HAIRY WOODPECKER by WARRENK
Mar., 1965 183 THE AUDITORY RANGE OF A HAIRY WOODPECKER By WARRENK. RAMP An experiment was conducted to determine the auditory range of a Hairy Wood- pecker (Dendrocopos vdlosus) through means of a conditioned response. The bird used had been taught to respond to sounds emitted from a pure tone audiometer by flying to an artificial feeding hole in a spruce log. This response then served to indicate whether or not the bird was hearing a given frequency. A survey of the literature shows that no determination of the hearing range of the Hairy Woodpecker has been made previously. Similar studies utilizing condi- tioned response have been made on other birds. Brand and Kellogg (Wilson Bull., 51, 1939 : 38-41) have reported the range in the English Sparrow (Passer domesticus) as 675-11,500 cycles per second (c.P.s.) and in the Domestic Pigeon (CoZ~mba Zivia) as 200-7500 c.p.s. The upper limit of hearing of the Starling (Sturnus v&g&s) has been shown to be 16,000 c.p.s. (Frings and Cook, Condor, 66, 1964:56-60). These and other studies have failed to indicate an accurate measurement of the sound pressure level used. It is felt that, unless the sound level is measured in air at a constant distance from the sound source, the validity of the results is questionable. In terms of amplitude, a speaker system has a frequency range through which it responds best. Hence, even if the output to the speakers is calibrated, a true evalua- tion of sound levels received by the bird cannot be obtained unless a sound level meter is used. -

Evaluation of Malingering Characteristics and Strategies During Hearing Assessment Sarah Michelle Thompson
University of Northern Colorado Scholarship & Creative Works @ Digital UNC Capstones Student Research 5-2017 Evaluation of Malingering Characteristics and Strategies During Hearing Assessment Sarah Michelle Thompson Follow this and additional works at: http://digscholarship.unco.edu/capstones Recommended Citation Thompson, Sarah Michelle, "Evaluation of Malingering Characteristics and Strategies During Hearing Assessment" (2017). Capstones. 19. http://digscholarship.unco.edu/capstones/19 This Text is brought to you for free and open access by the Student Research at Scholarship & Creative Works @ Digital UNC. It has been accepted for inclusion in Capstones by an authorized administrator of Scholarship & Creative Works @ Digital UNC. For more information, please contact [email protected]. ©2017 SARAH MICHELLE THOMPSON ALL RIGHTS RESERVED UNIVERSITY OF NORTHERN COLORADO Greeley, Colorado The Graduate School EVALUATION OF MALINGERING CHARACTERISTICS AND STRATEGIES DURING HEARING ASSESSMENT A Capstone Research Project Submitted in Partial Fulfillment of the Requirements for the Degree of Doctor of Audiology Sarah Michelle Thompson College of Natural and Health Sciences School of Human Sciences Audiology & Speech-Language Sciences May 2017 This Capstone Project by: Sarah Michelle Thompson Entitled: Evaluation of Malingering Characteristics and Strategies During Hearing Assessment Has been approved as meeting the requirement for the Degree of Doctor of Audiology in the College of Natural and Health Sciences in the School of Human Sciences, Program of Audiology and Speech-Language Sciences Accepted by the Capstone Research Committee Kathryn Bright, Ph.D., Co-Research Advisor Tina M. Stoody, Ph.D., Co-Research Advisor Kathleen Fahey, Ph.D., Committee Member Accepted by the Graduate School Linda L. Black, Ed.D. Associate Provost and Dean Graduate School and International Admission ABSTRACT Thompson, Sarah Michelle.