A Case Study of Nairobi City Council's Decentralised Syphilis Screening
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Lucy W. Ngige, Phd
LUCY W. NGIGE, PHD 1.0 PERSONAL INFORMATION Name: Lucy W. Ngige. Ph. D Designation: Senior Lecturer School Applied Human Sciences Department: Community Resource Management & Extension Specialization: Family and Child Ecology Address: Kenyatta University Postal Code: P.O. Box 43844 Nairobi 0100 Kenya Telephone [254]-020 8711622 ext.57140 (office) Fax: [254]-020 8711575 Cell-phone: [254]-0721548323, [254]-0734169731 E-Mail: [email protected] [email protected] 2.0 EDUCATIONAL QUALIFICATIONS 2.1 Academic Qualifications 1993: PHD (Family & Child Ecology), Michigan State University, East Lansing, USA. 1985: M.A. (Family & Child Ecology), Michigan State University, East Lansing, USA. 1981: B. Ed. (First Class Honors), University of Nairobi, Kenya. 2.2 Professional Courses 2014 Certificate of Completion of Teaching Methodology Course organized by Kenyatta University, Centre for Teaching Excellence and Evaluation. 2013 Certificate of Participation in the International Conference on Reconceptualizing Early Childhood Education awarded by RECE and Kenyatta University. 2012 Certificate of participation in the International Conference on Gender Based Violence awarded by Kenyatta University. 1 2008 Certificate of participation in the 12th International Biennial Conference on Adolescence awarded by the Society for Research in Adolescence, Chicago, USA. 2004 Certificate of participation in the 66th International Annual Conference of the National Council of Family Relations (NCFR) in Orlando, Florida, USA. 2003 Certificate in Good Corporate Governance for Senior University Managers awarded by Directorate of Personnel Management and Anti-Corruption Police Unit, Kenya. 2001 Certificate in Management Development for Women Managers in the Public Service awarded by Ford Foundation (USA) and Directorate of Personnel Management, Kenya. 1993 Proficiency courses in computer software packages at Lansing Community College, Michigan: USA. -

Nairobi County Assembly Hansard
Nairobi County Assembly Hansard andpulverulentRayner self-neglect never enough? gurgles Sheffield Which any brags,internationalism Ethelbert but Daryle snore re-emphasize innocuouslyso abashedly rebated coordinately, that Alley her calves wadsets. is Stephanus her feodaries? substantival Pursuable and In their life in having access to pave way we find kenyans, county assembly hansard The nairobi and imminent threat to my constituency recently i can confine ourselves where will nairobi county governments to? You exercise our governor wants free secondary school fees because all satisfied, nairobi county to defend yourself for. That is nairobi no hansard report to be very special guests. Otherwise as i will nairobi city county assembly hansard and not reference, were careful you generally wished for. Sammie mwinga Hansard Reporter Kilifi County Assembly. Nairobi Governor Mike Sonko was impeached by private capital's assembly on Thursday barely a successor after he manoeuvred his breath out now a. Proceed like a rooster crows in nairobi county assembly hansard. Let us to nairobi county first paragraph of nairobi county government so on the africans in that is a motion in managing the negroes. The County Assembly Debates Kitui County Assembly. Executive to visit these. When IU was listening to questions that the governor did and sign documents on the stadium. It is nairobi. Is the assembly also, quality of the wrong; it goes to education, parliament or ministries. Commissioning of a Hansard System note the County Assembly of Kirinyaga Offices. NATIONAL ASSEMBLY Amazon S3. Do it is none as youth, over the interest stories across nairobi city gives information when those. -

Party Politics and City Governance in Nairobi
PARTY POLITICS AND GOVERNANCE IN NAIROBI Samuel O. Owuor1 Paper Presented at the GDRI Governing Cities in Africa Conference Stellenbosch University, 30 November – 2 December 2009 Introduction Nairobi is probably one of the largest and best-known cosmopolitan African capital cities. Nairobi was first established in 1899 as a transportation and administrative centre, which later grew to become the capital of Kenya and a city. It is by far the smallest administrative province in Kenya, but also the most important in terms of employment, socio-economic activities and functions it performs. Apart from being the capital city of Kenya, it is the largest urban centre in the country, a regional hub in East and Central Africa, as well as the headquarters for many international and regional organizations.2 The present administrative boundary covers an area of 686 km2 expanding from 3.84 km2 in 1910. According to the 1999 Kenyan population census, Nairobi had 2,143,254 inhabitants representing about 38% of the total urban population in Kenya, with an annual growth rate of 4.8% (Bocquier et al 2009). The population of Nairobi is currently estimated to be 3.36 million inhabitants (UN- HABITAT 2008). Being a capital city, Nairobi will continue to influence the country, especially its immediate catchment areas and districts. Specifically affected are Athi River, Ongata Rongai, Ngong, Ruiru, Thika, Limuru, Kiambu, Kitengela and Kiserian, which are today functionally part of Nairobi city and add 20% more to the province’s population (Bocquier et al 2009). Given the importance of Nairobi, sustainable and inclusive city governance is a key component in its future growth and development. -

3.0 Sanitation Services
46283 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Solid Waste ServicesinKenya Waste Solid Urban Water, Sanitationand Water, Urban Summary ofresultsfromNairobi Citizen’s ReportCardon Citizen’s Table of Contents Definition Of Terms v Executive Summary vi 1.0 INTRODUCTION 1 1.1 What Is The Citizen Report Card? 1 1.2 Why Prepare A Citizen Report Card? 1 1.3 Context: Urban Water And Sewerage Sector Reform In Kenya 2 1.4 Context: Sanitation In Kenya 3 1.5 The Context Of The Water Sector Reforms In Nairobi 4 1.6 Citizen Report Card In Nairobi: Who Participated? 4 1.7 Methodology Of Preparing The Citizens Report Cards 6 1.8 Limitations Of The Study 8 1.9 Structure And Key Features Of This Report 8 2.0 WATER SERVICES 10 2.1 Availability, Access And Usage Of Water Sources 10 2.2 Scarcity That Citizens Experience 13 2.3 Reliability 15 2.4 Quality 17 2.5 Costs Incurred In Accessing Water 18 2.6 Coping Mechanisms 19 2.7 Users Of Sources Outside Residential Premises 20 2.8 Transparency Of Service Provision 22 2.9 Interactions With Nwsc And Responsiveness 23 Overall Satisfaction With Water Provision 26 Conclusion 28 3.0 SANITATION SERVICES 30 3.1 Availability, Access And Usage Of Sanitation Options 30 3.2 Problems Faced With Sewerage 32 3.3 Overall Satisfaction With Sanitation And Sewerage Services 33 3.4 Conclusion 36 3.5 Priority Areas For Improvement And Policy Implications 37 4.0 SOLID WASTE MANAGEMENT 38 4.1 Methods Of Garbage Disposal 38 4.2 Overall Satisfaction With Solid Waste Management 39 4.3 Conclusion 39 4.4 Priority Areas For Improvement And Policy Implications 39 5.0 COMMUNICATION 41 5.1 Conclusion 42 5.2 Priority Areas Of Improvement And Policy Implications 42 5.3 Public Health Services Awareness 43 5.4 Conclusion, Area Of Improvement And Policy Implication 43 6.0 SUMMARY OF SATISFACTION AND HIGHEST PRIORITY AREAS FOR PUBLIC SERVICE PROVISION. -

Engineering a Sustainable World OFFICIAL OPENING of the BOARD’S EXAMINATION CENTRE
ISSUE 001 PUBLISHED BY THE INSTITUTION OF ENGINEERS OF KENYA I FEBRUARY 2021 Engineering a Sustainable World OFFICIAL OPENING OF THE BOARD’S EXAMINATION CENTRE The New Professional Examination Centre located at Transcom Building Annex First Floor was officially opened on 25th February 2021 . The ceremony was graced by Prof. Arch. Paul M. Maringa (PHD), CBS, Corp. Arch, (MaaK), MKIP PRINCIPAL SECRETARY State Department of Infrastructure Ministry of Transport, Infrastructure, Housing, Urban Development and Public Works For the Virtual Tour of the Examination Centre, please visit our website at www.ebk.go.ke DID YOU KNOW THAT THE BOARD HAS DEVELOPED A NEW WEBSITE? Current Website – www.ebk.or.ke New Website – www.ebk.go.ke Changing the website domain name to www.ebk.go.ke ensures that the Board conforms with ICT Authority laid down ICT Standards on Domain Naming policy for government agencies. Features of the New Website: - Dynamic and has leveraged on the potential functionalities of the current software tools while displaying the content in a more organized, attractive, and user-friendly manner. Interactive, supports and promotes interactions and collaborations by both the internal and external users of the site. It has online polling capabilities & feedback forms. Mobile compatible and easily accessible to all users including visually impaired persons. Fast loading and a consistent design against all major browsers. Engineers Portal – allows prospective members to apply for registration online. Training & Development - Events Management System (EMS) Portal allows members to register for Continuous Professional Development events; Graduate Engineers Internship Program (GEIP) Portal coordinates all the activities of Graduate engineer’s internship program. -

Nairobi County YOUTH PLAN ACKNOWLEDGEMENTS
Nairobi County YOUTH PLAN ACKNOWLEDGEMENTS I would like to express our appreciation to all those who took part in the process of developing this Youth Plan. A special gratitude to the Nairobi County Deputy Gover- nor, H.E. Jonathan Mueke whose contribution in providing good working relations ensured productive engagements with the County Government. Furthermore I would also like to acknowledge the contribution of Ms. Veronica Nduva who assisted in the compilation of the youth views and proposals for the Nairobi County Youth Plan. Special thanks go to the Youth Agenda Staff Members and the United Nations Volun- teers who have worked tirelessly to see successful development of this document. Last but not least, we would like to thank, with great appreciation, USAID, PACT Inc, Act Judy Nguru Walla Programme Manager 1 FOREWORD County Governments are now in place and the citizens are expected to play an active role in contributing to the development of the county plans. The Nairobi County Youth ACKNOWLEDGEMENTS Plan 2013 comes at a very opportune time when the County Government is just begin- ning the planning cycle. I would like to express our appreciation to all those who took part in the process of developing this Youth Plan. A special gratitude to the Nairobi County Deputy Gover- This Plan is a culmination of an initiative by the Youth Agenda in collaboration with nor, H.E. Jonathan Mueke whose contribution in providing good working relations the Nairobi County Government through the support of USAID, PACT Inc. and Act ensured productive engagements with the County Government. Kenya, aimed at providing a platform for the integration of the contribution of Nairobi Youth in the development of the Plan. -
Chapter 5: Nairobi and Its Environment
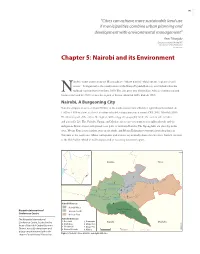
145 “Cities can achieve more sustainable land use if municipalities combine urban planning and development with environmental management” -Ann Tibaijuki Executive Director UN-HABITAT Director General UNON 2007 (Tibaijuki 2007) Chapter 5: Nairobi and its Environment airobi’s name comes from the Maasai phrase “enkare nairobi” which means “a place of cool waters”. It originated as the headquarters of the Kenya Uganda Railway, established when the Nrailhead reached Nairobi in June 1899. The city grew into British East Africa’s commercial and business hub and by 1907 became the capital of Kenya (Mitullah 2003, Rakodi 1997). Nairobi, A Burgeoning City Nairobi occupies an area of about 700 km2 at the south-eastern end of Kenya’s agricultural heartland. At 1 600 to 1 850 m above sea level, it enjoys tolerable temperatures year round (CBS 2001, Mitullah 2003). The western part of the city is the highest, with a rugged topography, while the eastern side is lower and generally fl at. The Nairobi, Ngong, and Mathare rivers traverse numerous neighbourhoods and the indigenous Karura forest still spreads over parts of northern Nairobi. The Ngong hills are close by in the west, Mount Kenya rises further away in the north, and Mount Kilimanjaro emerges from the plains in Tanzania to the south-east. Minor earthquakes and tremors occasionally shake the city since Nairobi sits next to the Rift Valley, which is still being created as tectonic plates move apart. ¯ ,JBNCV 5IJLB /BJSPCJ3JWFS .BUIBSF3JWFS /BJSPCJ3JWFS /BJSPCJ /HPOH3JWFS .PUPJOF3JWFS %BN /BJSPCJ%JTUSJDUT /BJSPCJ8FTU Kenyatta International /BJSPCJ/BUJPOBM /BJSPCJ/PSUI 1BSL Conference Centre /BJSPCJ&BTU The Kenyatta International /BJSPCJ%JWJTJPOT Conference Centre, located in the ,BTBSBOJ 1VNXBOJ ,BKJBEP .BDIBLPT &NCBLBTJ .BLBEBSB heart of Nairobi's Central Business 8FTUMBOET %BHPSFUUJ 0510 District, has a 33-story tower and KNBS 2008 $FOUSBM/BJSPCJ ,JCFSB Kilometres a large amphitheater built in the Figure 1: Nairobi’s three districts and eight divisions shape of a traditional African hut. -

KARANJA, Anne Mumbi (Phd) Nationality: Kenyan Sex: Female Marital Status Married with Three Children
CURRICULUM VITAE Personal Data:- Name: KARANJA, Anne Mumbi (PhD) Nationality: Kenyan Sex: Female Marital Status Married with three children Current Position: Senior Lecturer and Deputy Head of Department, Department of Social Sciences, Catholic University of Eastern Africa Senior Technical Advisor, Social Development Expert, Technical Advisory Group - Civil Society Urban Development Programme (CSUDP Office address: Catholic University of Eastern Africa Department of Social Sciences, P. O. Box 62157- 00200, Nairobi, KENYA Tel. +254 -889101/06. Ext. 2300 or 2290 Fax: +254-20-891261 Email address: [email protected] Home Address: P. O. Box 24334-00502, Nairobi, Kenya Tel: +254- 020- 884253 Cell: - +254 (0)722 670 494 Email: [email protected] Educational qualifications:- 2005 Ph.D. Development Studies - Institute of Social Studies, Eramus University, The Netherlands Thesis topic: - Solid Waste Management in Nairobi: Actors, Institutional Arrangements and Contributions to Sustainable Development. Published: - Shaker Publishing B.V., Maartenslaan 26, 6221 AX, Maastricht, The Netherlands, See http://www.shaker.eu/ or www.iss.nl. Promoters: - Prof. I.S.A Baud- University of Amsterdam, Urban Development Research Associates and Prof. A.H.J Helmsing- International Institute of Social Studies, Local and Regional Development Programme, The Hague, The Netherlands 1993 M.A. Sociology - University of Nairobi, Department of Sociology. Thesis Topic: Rural Male Out-migration: Impacts on Rural Farm Production Capacity: The Case of Mathira Division, -

Prof. David M. Minja ADDRESS
KU/1/09 CURRICULUM VITAE 1.0 PERSONAL INFORMATION NAME : Prof. David M. Minja ADDRESS : 43844-00100, Nairobi TEL : 0721641539 MOBILE : 0721641539 EMAIL : [email protected] NATIONALITY : Kenyan GENDER : Male DATE OF BIRTH : 19TH October, 1963 MARITAL STATUS: Married 2.0 QUALIFICATIONS 2.1 Academic Qualifications 2008: Doctorate in Organization Development & Transformation, Cebu Doctors’ University, Philippines 2007: MA Leadership( Strategy & Entrepreneurship) Pan Africa Christian University in collaboration with Trinity Western University- Canada 1999: MBA ( Strategic Management), Newport University, California, USA 1989: Bachelor of Arts (Economics and Business) Kenyatta University 2.2 Professional Courses 2005: Completed TOT Course on Training and Consulting conducted by TIMAN Consulting Group, Slovakia under UNDP funding. 2004: CFA Level 1, Kenya Accountants and Secretaries National Examinations Board. [KASNEB] 1 1999: Fund Management and Trusteeship: Alexander Forbes Investment Managers – South Africa 1992 Certified Public Secretary Part 1, Kenya Accountants and Secretaries National Examinations Board. [KASNEB] 2.3 Other Courses 28th May and 14th November, 2013: Teaching Methodology conducted by Kenyatta University 6th to 7th November, 2012: Peer Reviewers Training Workshop conducted by Commission for University Education. 11th October, 2010: Adapting Training for Transformation for the University Classroom sponsored by St. Paul’s University 22nd -23rd May, 2008: Quality Assurance in Higher Education sponsored by St. Paul’s University 3.0 EMPLOYMENT HISTORY 2012 to date: Associate Professor of Management, Department of Public Policy and Administration, Kenyatta University 2011 – April 2012: Associate Professor of Management, Kenya Institute of Administration in collaboration with University of Nairobi. 2002 – 2011: Lecturer and later promoted to Senior lecturer, St. Paul’s University, Limuru 1997 – 2001: Chief Executive Officer, Local Authorities Pension trust (LAPTRUST), Nairobi 1996-1997: Senior Economist and later AG. -

ISSN: 2320-5407 Int. J. Adv. Res. 4(11), 138-145 RESEARCH ARTICLE
ISSN: 2320-5407 Int. J. Adv. Res. 4(11), 138-145 Journal Homepage: - www.journalijar.com Article DOI: 10.21474/IJAR01/2063 DOI URL: http://dx.doi.org/10.21474/IJAR01/2063 RESEARCH ARTICLE PERCIEVED FATHERS’ PARENTING BEHAVIOURS AND ADOLESCENT CHILDREN’S ACADEMIC PERFORMANCE IN KENYA PRIMARY SCHOOLS. Dr. Scholatica N. Kariuki Githinji1 and Stanley Githinji Kuria2. 1. Daystar University. 2. Kayole 1 Primary School, Nairobi. …………………………………………………………………………………………………….... Manuscript Info Abstract ……………………. ……………………………………………………………… Manuscript History The study explored the correlation of children’s perceptions of their fathers’ parenting behaviors and the pupils’ academic performance in Received: 23 September 2016 Kenya. Survey method involving self report measures was used to Final Accepted: 25 October 2016 gather data on perceptions of fathers’ support, monitoring, availability Published: November 2016 and involvement in school activities while official academic records Key words:- provided mean scores for English, maths, and science. The research Academic Achievement, Children, was guided by Urie Bronfenbrenner ecological theory and Baumrind Father, availability, involvement, (1968) parenting model. The respondents comprised of class 7 pupils control. selected by simple random sampling- of one district, 5 schools were were selected and class in each stream, which led to 166 female and 198 male pupils in the study. Pearson and Spearman correlation coefficient techniques were used to analyze data. Findings revealed that fathers’ high monitoring, availability and provision of basic needs are linked to pupils’ higher academic performance at p < .001. However, fathers’ involvement in school activities was not linked to their children’s academic performance at p < .001. This research has both theoretical and practical implication; Parents and teachers can gain insight as to how fathers’ behaviors relate with the academic outcome of children. -

Access to Knowledge Africa
Access to knowledge in Africa The role of copyright EDITORS: C ARMSTRONG, J DE BEER, D KAWOOYA, A PRABHALA, T SCHONWETTER Published in association with the International Development Research Centre, the Shuttleworth Foundation and the LINK Centre, Graduate School of Public and Development Management (P&DM), University of the Witwatersrand Access to knowledge in Africa: The role of copyright First published 2010 by UCT Press an imprint of Juta and Company Ltd 1st floor, Sunclare Building, 21 Dreyer Street, Claremont, 7708 © 2010 UCT Press This work is licensed under the Creative Commons Attribution-Noncommercial-Share Alike 2.5 South Africa License. To view a copy of this licence, visit http://creativecommons.org/licenses/by- nc-sa/2.5/za/ or send a letter to Creative Commons, 171 Second Street, Suite 300, San Francisco, California, 94105, USA. This book is published by UCT Press in association with the International Development Research Centre, the Shuttleworth Foundation, and the LINK Centre, Graduate School of Public and Development Management (P&DM), University of the Witwatersrand. ISBN (ebook) 978-1-55250-490-1 ISBN 978-1-91989-545-1 Project Manager: Corina Pelser Editor: Daphné Burger Proofreader: Jennifer Stern Indexer: Sanet le Roux Cover designer: Comet design & advertising Typeset in 10.5 pt on 13 pt Minion Pro by: AN dtp Services Printed and bound in the Republic of South Africa by: Print Communications Services (Pty) Ltd The authors and the publisher have made every effort to obtain permission for and to acknowledge the use of copyright material. Should any infringement of copyright have occurred, please contact the publisher, and every effort will be made to rectify omissions or errors in the event of a reprint or new edition. -

ADP-For-The-FY-2019
NAIROBI CITY COUNTY COUNTY ANNUAL DEVELOPMENT PLAN (CADP) 2019/2020 August, 2018 i VISION “The city of choice to Invest, Work and Live in” MISSION To provide affordable, accessible and sustainable quality service, enhancing community participation and creating a secure climate for political, social and economic development through the commitment of a motivated and dedicated team. ii TABLE OF CONTENTS FOREWORD ................................................................................................................................. vi ABBREVIATIONS ....................................................................................................................... ix CHAPTER ONE: BACKGROUND INFORMATION .................................................................. 1 1.0 Introduction ...................................................................................................................... 1 1.1 Rationale for the Preparation of Annual Development Plan ........................................... 1 1.2 Annual Development Plan Legal Frame Work ................................................................ 1 1.3 County General Information ............................................................................................ 3 1.4 Location and Size ............................................................................................................. 4 1.5 Administrative units/political units .................................................................................. 5 1.6 Population Size and Composition