Ultrasound in Acute Kidney Injury
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hydronephrosis
Hydronephrosis Natasha Brownrigg RN(EC), MN, NP-Pediatrics Assistant Clinical Professor, McMaster School of Nursing Nurse Practitioner, Pediatric Urology, McMaster Children’s Hospital, Hamilton, ON, Canada Dr. Jorge DeMaria Pediatric Urologist, McMaster Children’s Hospital Professor Department of Surgery/Urology, McMaster University, Hamilton, ON, Canada Dr. Luis H.P. Braga Pediatric Urologist, McMaster Children’s Hospital. Associate professor Department of Surgery/Urology, McMaster University, Hamilton, ON, Canada What is hydronephrosis? Hydro Nephrosis Hydronephrosis += Refers to water Refers to the kidney A build up of fluid or fluid (urine) in the kidney Hydronephrosis is the medical term for a build-up of urine in the kidney. As the urine builds up, it stretches or dilates the inside of the kidney, known as the collecting system. If an unborn baby has hydronephrosis, an ultrasound scan will show a build-up of urine in the kidney. This is called “antenatal hydronephrosis.” Hydronephrosis is found in as many as five out of 100 pregnancies. Hydronephrosis may also be found after birth. For example, if a baby has a urinary tract infection, an ultrasound of the baby’s kidneys and bladder may detect hydronephrosis. Key points to remember if your baby has hydronephrosis • Your baby can grow and develop normally with hydronephrosis. • Hydronephrosis may affect one kidney or both. • Hydronephrosis is a finding, not a disease. • Further tests are needed to find the cause of hydronephrosis. • If the cause is known, a pediatric urologist will discuss the possible treatment. Surgery is sometimes required to correct the cause of the hydronephrosis. Hydronephrosis is often transient and improves without any intervention. -
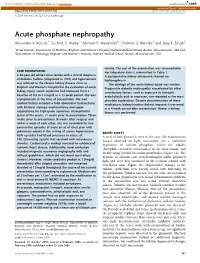
Acute Phosphate Nephropathy Alexander K
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector http://www.kidney-international.org the renal consult & 2009 International Society of Nephrology Acute phosphate nephropathy Alexander K. Rocuts1, Sushrut S. Waikar1, Mariam P. Alexander1,2, Helmut G. Rennke2 and Ajay K. Singh1 1Renal Division, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA and 2Department of Pathology, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA minute. The rest of the examination was unremarkable. CASE PRESENTATION HerlaboratorydataissummarizedinTable1. A 60-year-old white Latino female with a clinical diagnosis A postoperative kidney ultrasound showed no of diabetes mellitus (diagnosed in 1993) and hypertension hydronephrosis. was referred to the chronic kidney disease clinic at The etiology of the acute kidney injury was unclear. Brigham and Women’s Hospital for the evaluation of acute Progressive diabetic nephropathy exacerbated by other kidney injury; serum creatinine had increased from a contributory factors, such as exposure to lisinopril, baseline of 0.9 to 1.5 mg/dl in a 11-week period. She was acetylsalicylic acid, or naproxen, was regarded as the most asymptomatic at the time of presentation. Her past plausible explanation. Despite discontinuation of these medical history included a total abdominal hysterectomy medications, kidney function did not improve; it worsened with bilateral salpingo oophorectomy and upper in a 4-week period after presentation. Hence, a kidney vaginectomy for high-grade squamous intraepithelial biopsy was performed. lesion of the cervix, 11 weeks prior to presentation. Three weeks prior to presentation (8 weeks after surgery) and within a week of each other, she was evaluated for two consecutive episodes of acute onset of chest pain with pulmonary edema in the setting of severe hypertension. -

PATHOLOGY of the RENAL SYSTEM”, I Hope You Guys Like It
ﺑﺴﻢ اﷲ اﻟﺮﺣﻤﻦ اﻟﺮﺣﯿﻢ ھﺬه اﻟﻤﺬﻛﺮة ﻋﺒﺎرة ﻋﻦ إﻋﺎدة ﺗﻨﺴﯿﻖ وإﺿﺎﻓﺔ ﻧﻮﺗﺎت وﻣﻮاﺿﯿﻊ ﻟﻤﺬﻛﺮة زﻣﻼﺋﻨﺎ ﻣﻦ اﻟﺪﻓﻌﺔ اﻟﺴﺎﺑﻘﺔ ٤٢٧ اﻷﻋﺰاء.. ﻟﺘﺘﻮاﻓﻖ ﻣﻊ اﻟﻤﻨﮭﺞ اﻟﻤﻘﺮر ﻣﻦ اﻟﻘﺴﻢ ﺣﺮﺻﻨﺎ ﻓﯿﮭﺎ ﻋﻠﻰ إﻋﺎدة ﺻﯿﺎﻏﺔ ﻛﺜﯿﺮ ﻣﻦ اﻟﺠﻤﻞ ﻟﺘﻜﻮن ﺳﮭﻠﺔ اﻟﻔﮭﻢ وﺳﻠﺴﺔ إن ﺷﺎء اﷲ.. وﺿﻔﻨﺎ ﺑﻌﺾ اﻟﻨﻮﺗﺎت اﻟﻤﮭﻤﺔ وأﺿﻔﻨﺎ ﻣﻮاﺿﯿﻊ ﻣﻮﺟﻮدة ﺑﺎﻟـ curriculum ﺗﻌﺪﯾﻞ ٤٢٨ ﻋﻠﻰ اﻟﻤﺬﻛﺮة ﺑﻮاﺳﻄﺔ اﺧﻮاﻧﻜﻢ: ﻓﺎرس اﻟﻌﺒﺪي ﺑﻼل ﻣﺮوة ﻣﺤﻤﺪ اﻟﺼﻮﯾﺎن أﺣﻤﺪ اﻟﺴﯿﺪ ﺣﺴﻦ اﻟﻌﻨﺰي ﻧﺘﻤﻨﻰ ﻣﻨﮭﺎ اﻟﻔﺎﺋﺪة ﻗﺪر اﻟﻤﺴﺘﻄﺎع، وﻻ ﺗﻨﺴﻮﻧﺎ ﻣﻦ دﻋﻮاﺗﻜﻢ ! 2 After hours, or maybe days, of working hard, WE “THE PATHOLOGY TEAM” are proud to present “PATHOLOGY OF THE RENAL SYSTEM”, I hope you guys like it . Plz give us your prayers. Credits: 1st part = written by Assem “ THe AWesOme” KAlAnTAn revised by A.Z.K 2nd part = written by TMA revised by A.Z.K د.ﺧﺎﻟﺪ اﻟﻘﺮﻧﻲ 3rd part = written by Abo Malik revised by 4th part = written by A.Z.K revised by Assem “ THe AWesOme” KAlAnTAn 5th part = written by The Dude revised by TMA figures were provided by A.Z.K Page styling and figure embedding by: If u find any error, or u want to share any idea then plz, feel free to msg me [email protected] 3 Table of Contents Topic page THE NEPHROTIC SYNDROME 4 Minimal Change Disease 5 MEMBRANOUS GLOMERULONEPHRITIS 7 FOCAL SEGMENTAL GLOMERULOSCLEROSIS 9 MEMBRANOPROLIFERATIVE GLOMERULONEPHRITIS 11 DIABETIC NEPHROPATHY (new) 14 NEPHRITIC SYNDROME 18 Acute Post-infectious GN 19 IgA Nephropathy (Berger Disease) 20 Crescentic GN 22 Chronic GN 24 SLE Nephropathy (new) 26 Allograft rejection of the transplanted kidney (new) 27 Urinary Tract OBSTRUCTION, 28 RENAL STONES 23 HYDRONEPHROSIS -

Impact of Urolithiasis and Hydronephrosis on Acute Kidney Injury in Patients with Urinary Tract Infection
bioRxiv preprint doi: https://doi.org/10.1101/2020.07.13.200337; this version posted July 13, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Impact of urolithiasis and hydronephrosis on acute kidney injury in patients with urinary tract infection Short title: Impact of urolithiasis and hydronephrosis on AKI in UTI Chih-Yen Hsiao1,2, Tsung-Hsien Chen1, Yi-Chien Lee3,4, Ming-Cheng Wang5,* 1Division of Nephrology, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chia-Yi, Taiwan 2Department of Hospital and Health Care Administration, Chia Nan University of Pharmacy and Science, Tainan, Taiwan 3Department of Internal Medicine, Fu Jen Catholic University Hospital, Fu Jen Catholic University, New Taipei, Taiwan 4School of Medicine, College of Medicine, Fu Jen Catholic University, New Taipei, Taiwan 5Division of Nephrology, Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan *[email protected] 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.07.13.200337; this version posted July 13, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Abstract Background: Urolithiasis is a common cause of urinary tract obstruction and urinary tract infection (UTI). This study aimed to identify whether urolithiasis with or without hydronephrosis has an impact on acute kidney injury (AKI) in patients with UTI. -

RENAL BIOPSY and GLOMERULONEPHRITIS by J
Postgrad Med J: first published as 10.1136/pgmj.35.409.604 on 1 November 1959. Downloaded from 604 RENAL BIOPSY AND GLOMERULONEPHRITIS By J. H. Ross, M.D., M.R.C.P. Senior Medical Registrar, The Connaught Hospital, and Assistant, The Mledical Unit, The London Hospital Introduction sufficient to establish a diagnosis in a few condi- Safe methods of percutaneous renal biopsy were tions such as amyloid disease and diabetic first described by Perez Ara (1950) and Iversen glomerulosclerosis, but cortex with at least io and Brun (I95I) who used aspiration techniques. glomeruli is necessary for an accurate assessment Many different methods have since been described; of the renal structure; occasionally, up to 40 the simplest is that of Kark and Muehrcke (1954) glomeruli may be present in a single specimen. who use the Franklin modification of the Vim- The revelation of gross structural changes in Silverman needle. the kidneys of patients who can be recognized Brun and Raaschou (1958) have recently re- clinically as having chronic glomerulonephritis is viewed the majority of publications concerned of little value and does not contribute to manage- with renal biopsy and have concluded that the risk ment or prognosis. In contrast, biopsy specimensProtected by copyright. to the patients is slight. They mentioned three from patients in the early stages of glomerulo- fatalities which have been reported but considered nephritis, particularly those who have developed that, in each case, death was probably due to the the nephrotic syndrome insidiously without disease process rather than the investigation. haematuria or renal failure or who showy no Retroperitoneal haematomata have been recorded evidence of disease other than proteinuria, may in patients with hypertension or uraemia but are provide useful information. -

Renal Tubular Acidosis in Children: State of the Art, Diagnosis and Treatment
www.medigraphic.org.mx Bol Med Hosp Infant Mex 2013;70(3):178-193 REVIEW ARTICLE Renal tubular acidosis in children: state of the art, diagnosis and treatment Ricardo Muñoz-Arizpe,1 Laura Escobar,2 Mara Medeiros3 ABSTRACT Overdiagnosis of renal tubular acidosis (RTA) has been recently detected in Mexican children, perhaps due to diagnostic errors as well as due to a lack of knowledge regarding the pathophysiology and molecular biochemistry involved in this illness. The objective of the present study is to facilitate the knowledge and diagnosis of RTA, a clinical condition infrequently seen worldwide. RTA is an alteration of the acid-base equilibrium due to a bicarbonate wasting in the proximal renal tubules [proximal RTA, (pRTA) or type 2 RTA] or due to a distal nephron hy- drogen ion excretion defect [distal RTA (dRTA) or type 1 RTA]. Hyperkalemic, or type 4 RTA, is due to alterations in aldosterone metabolism. RTA may be primary, secondary, acquired or hereditary and frequently presents secondary to an array of systemic diseases, usually accom- panied by multiple renal tubular defects. The main defect occurs in the transmembrane transporters such as carbonic anhydrase (CA I and + - - + - II), H -ATPase, HCO3 /Cl (AE1) exchanger and Na /HCO3 (NBCe1) cotransporter. Diagnosis should include the presence of hyperchloremic metabolic acidosis with normal serum anion gap (done in an arterial or arterialized blood sample), lack of appetite, polyuria, thirst, growth failure, and rickets; nephrocalcinosis and renal stones (in dRTA); abnormal urine anion gap and abnormal urine/serum pCO2 gradient. Diagnosis of a primary systemic disease must be made in cases of secondary RTA. -

Silent Hydronephrosis, a Hazard Revisited
SILENT HYDRONEPHROSIS, A HAZARD REVISITED By JOEL S. ROSEN, M.D., JOHN B. NANNINGA, M.D. and VINCENT J. O'CONOR, M.D. Midwest Regional Spinal Cord Injury Care System, Chicago, Illinois, U.S.A. Abstract. Six patients with neurogenic bladder secondary to spinal cord injury were seen in our Centre for routine follow-up. All of these individuals had attained the catheter-free state by various means and were, by their standards, functioning very well. They had gone from 6 months to 2t years without genito-urinary re-evaluations. One individual had a normal urogram I year after catheter removal and then 2 years later was noted to have bilateral hydronephrosis. Development of silent hydronephrosis in the catheter-free state, its treatment, and a regimen for following patients are discussed. THE recognition of hydronephrosis following spinal cord injury has been docu mented in the past by several authorities (Talbot & Bunts, 1940; Hutch & Bunts, 1951; Damanski & Gibbon, 1956). Damanski and Gibbon stated that hydro nephrosis occurred in one.;.third of a group of patients suffering from spinal cord injury. The changes have been reported to occur as early as 2 months after injury to as long as 8 years later. Ross (1963) has found hydronephrosis to be associated with the neural damage, urinary infection and back pressure; the importance of each factor varying considerably with the individual, Ascoli and Franch (1970) noted hydronephrosis most frequently in patients more than 4 years post trauma. Warning signs of impending hydronephrosis include the onset of urinary tract infection, deterioration of bladder function, increasing residual urine, bladder hypertonia and the appearance of bladder diverticula and reflux. -

The Links Between Microbiome and Uremic Toxins in Acute Kidney Injury: Beyond Gut Feeling—A Systematic Review
toxins Article The Links between Microbiome and Uremic Toxins in Acute Kidney Injury: Beyond Gut Feeling—A Systematic Review Alicja Rydzewska-Rosołowska 1,* , Natalia Sroka 1, Katarzyna Kakareko 1, Mariusz Rosołowski 2 , Edyta Zbroch 1 and Tomasz Hryszko 1 1 2nd Department of Nephrology and Hypertension with Dialysis Unit, Medical University of Białystok, 15-276 Białystok, Poland; [email protected] (N.S.); [email protected] (K.K.); [email protected] (E.Z.); [email protected] (T.H.) 2 Department of Gastroenterology and Internal Medicine, Medical University of Białystok, 15-276 Białystok, Poland; [email protected] * Correspondence: [email protected] Received: 30 October 2020; Accepted: 9 December 2020; Published: 11 December 2020 Abstract: The last years have brought an abundance of data on the existence of a gut-kidney axis and the importance of microbiome in kidney injury. Data on kidney-gut crosstalk suggest the possibility that microbiota alter renal inflammation; we therefore aimed to answer questions about the role of microbiome and gut-derived toxins in acute kidney injury. PubMed and Cochrane Library were searched from inception to October 10, 2020 for relevant studies with an additional search performed on ClinicalTrials.gov. We identified 33 eligible articles and one ongoing trial (21 original studies and 12 reviews/commentaries), which were included in this systematic review. Experimental studies prove the existence of a kidney-gut axis, focusing on the role of gut-derived uremic toxins and providing concepts that modification of the microbiota composition may result in better AKI outcomes. Small interventional studies in animal models and in humans show promising results, therefore, microbiome-targeted therapy for AKI treatment might be a promising possibility. -

Guidelines on Urolithiasis
Guidelines on Urolithiasis C. Türk (chair), T. Knoll (vice-chair), A. Petrik, K. Sarica, A. Skolarikos, M. Straub, C. Seitz © European Association of Urology 2014 TABLE OF CONTENTS PAGE 1. METHODOLOGY 7 1.1 Introduction 7 1.2 Data identification 7 1.3 Evidence sources 7 1.4 Level of evidence and grade of recommendation 7 1.5 Publication history 8 1.5.2 Potential conflict of interest statement 8 1.6 References 8 2. CLASSIFICATION OF STONES 9 2.1 Stone size 9 2.2 Stone location 9 2.3 X-ray characteristics 9 2.4 Aetiology of stone formation 9 2.5 Stone composition 9 2.6 Risk groups for stone formation 10 2.7 References 11 3. DIAGNOSIS 12 3.1 Diagnostic imaging 12 3.1.1 Evaluation of patients with acute flank pain 12 3.1.2 Evaluation of patients for whom further treatment of renal stones is planned 13 3.1.3 References 13 3.2 Diagnostics - metabolism-related 14 3.2.1 Basic laboratory analysis - non-emergency urolithiasis patients 15 3.2.2 Analysis of stone composition 15 3.3 References 16 4. TREATMENT OF PATIENTS WITH RENAL COLIC 16 4.1 Renal colic 16 4.1.1 Pain relief 16 4.1.2 Prevention of recurrent renal colic 16 4.1.3 Recommendations for analgesia during renal colic 17 4.1.4 References 17 4.2 Management of sepsis in obstructed kidney 18 4.2.1 Decompression 18 4.2.2 Further measures 18 4.2.3 References 18 5. STONE RELIEF 19 5.1 Observation of ureteral stones 19 5.1.1 Stone-passage rates 19 5.2 Observation of kidney stones 19 5.3 Medical expulsive therapy (MET) 20 5.3.1 Medical agents 20 5.3.2 Factors affecting success of medical expulsive -

Guidelines on Urolithiasis
GUIDELINES ON UROLITHIASIS (Text update April 2010) Ch. Türk (chairman), T. Knoll (vice-chairman), A. Petrik, K. Sarica, C. Seitz, M. Straub, O. Traxer Eur Urol 2001 Oct;40(4):362-71 Eur Urol 2007 Dec;52(6):1610-31 J Urol 2007 Dec;178(6):2418-34 Methodology This update is based on the 2008 version of the Urolithiasis guidelines produced by the former guidelines panel. Literature searches were carried out in Medline and Embase for ran- domised control trials and systematic reviews published between January 1st, 2008, and November 30, 2009, and sig- nificant differences in diagnosis and treatment or in evidence level were considered. Introduction Urinary stone disease continues to occupy an important place in everyday urological practice. The average lifetime risk of stone formation has been reported in the range of 5-10%. Recurrent stone formation is a common problem with all types of stones and therefore an important part of the medical care of patients with stone disease. Classification and Risk Factors Different categories of stone formers can be identified based Urolithiasis 251 on the chemical composition of the stone and the severity of the disease (Table 1). Special attention must be given to those patients who are at high risk of recurrent stone formation (Table 2). Table 1: Categories of stone formers Stone composition Category Non-calcium Infection stones: INF stones Magnesium ammonium phosphate Ammonium urate Uric acid UR Sodium urate Cystine CY Calcium First time stone former, without residual So stones stone or stone fragments. First time stone former, with residual Sres stone or stone fragments. -

Renal Papillary Necrosis in Infancy PETER HUSBAND* and K
Arch Dis Child: first published as 10.1136/adc.48.2.116 on 1 February 1973. Downloaded from Archives of Disease in Childhood, 1973, 48, 116. Renal papillary necrosis in infancy PETER HUSBAND* and K. A. HOWLETT From the Departments of Paediatrics and Radiology, Charing Cross Group of Hospitals, Fulham Hospital, London Husband, P., and Howlett, K. A. (1973). Archives of Disease in Childhood, 48, 116. Renal papillary necrosis in infancy. Two infants developed renal papillary necrosis after acute illnesses associated with dehydration. After a short oliguric phase there was a longer phase characterized by impaired urinary concen- tration, hyponatraemia, metabolic acidosis, and a raised blood urea. Intravenous urograms showed contrast collecting in the papillae, with subsequent sinus formation extending into the medulla. In one case impaired urinary concentration was still present 21 months after the initial illness. Renal papillary necrosis was originally described admitted to hospital 9 days later after he had been by Friedreich (1877) in a man aged 70 years. found in his cot, grey, with respiratory distress and a Since then the majority of further cases reported high temperature. 3 days before he had diarrhoea and have also been in adults. It has been thought to vomiting for 24 hours but subsequently tolerated feeds be uncommon and usually to have a fatal outcome of full cream Cow and Gate milk, 180 ml 5 times a day. He was again extremely ill: temperature 40 3 °C, pale, copyright. in infancy and childhood (Davies, Kennedy, and cyanosed with a rapid respiratory rate, but not dehydra- Roberts, 1969). In the newborn infant renal ted. -

Risk of Renal Function Decline in Patients with Ketamine-Associated Uropathy
International Journal of Environmental Research and Public Health Article Risk of Renal Function Decline in Patients with Ketamine-Associated Uropathy Shih-Hsiang Ou 1,2,3, Ling-Ying Wu 4, Hsin-Yu Chen 1,2, Chien-Wei Huang 1,2, Chih-Yang Hsu 1,2, Chien-Liang Chen 1,2 , Kang-Ju Chou 1,2, Hua-Chang Fang 1,2 and Po-Tsang Lee 1,2,* 1 Division of Nephrology, Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung 813, Taiwan; [email protected] (S.-H.O.); [email protected] (H.-Y.C.); [email protected] (C.-W.H.); [email protected] (C.-Y.H.); [email protected] (C.-L.C.); [email protected] (K.-J.C.); [email protected] (H.-C.F.) 2 Faculty of Medicine, School of Medicine, National Yang-Ming University, Taipei 112, Taiwan 3 Graduate Institute of Clinical Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung 807, Taiwan 4 Department of Obstetrics and Gynecology, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung 833, Taiwan; [email protected] * Correspondence: [email protected]; Tel.: +886-7342-2121 (ext. 8090) Received: 8 August 2020; Accepted: 29 September 2020; Published: 4 October 2020 Abstract: Ketamine-associated diseases have been increasing with the rise in ketamine abuse. Ketamine-associated uropathy is one of the most common complications. We investigated the effects of ketamine-associated uropathy on renal health and determined predictors of renal function decline in chronic ketamine abusers. This retrospective cohort study analyzed 51 patients (22 with ketamine- associated hydronephrosis and 29 with ketamine cystitis) from Kaohsiung Veterans General Hospital in Taiwan.