Downloading Raw Data from Tool Aimed at Identifying Congenital Cataracts [44] from Orphanet [70]
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

ICD-10-CM Expert for SNF, IRF, and LTCH the Complete Official Code Set Codes Valid from October 1, 2018 Through September 30, 2019
EXPERT 2019 ICD-10-CM Expert for SNF, IRF, and LTCH The complete official code set Codes valid from October 1, 2018 through September 30, 2019 Power up your coding optum360coding.com ITSN_ITSN19_CVR.indd 1 12/4/17 2:54 PM Contents Preface ................................................................................ iii ICD-10-CM Index to Diseases and Injuries .......................... 1 ICD-10-CM Official Preface ........................................................................iii Characteristics of ICD-10-CM ....................................................................iii ICD-10-CM Neoplasm Table ............................................ 331 What’s New for 2019 .......................................................... iv ICD-10-CM Table of Drugs and Chemicals ...................... 349 Official Updates ............................................................................................iv Proprietary Updates ...................................................................................vii ICD-10-CM Index to External Causes ............................... 397 Introduction ....................................................................... ix ICD-10-CM Tabular List of Diseases and Injuries ............ 433 History of ICD-10-CM .................................................................................ix Chapter 1. Certain Infectious and Parasitic Diseases (A00-B99) .........................................................................433 How to Use ICD-10-CM Expert for Skilled Nursing Chapter -

History of the Development of the ICD
History of the development of the ICD 1. Early history Sir George Knibbs, the eminent Australian statistician, credited François Bossier de Lacroix (1706-1777), better known as Sauvages, with the first attempt to classify diseases systematically (10). Sauvages' comprehensive treatise was published under the title Nosologia methodica. A contemporary of Sauvages was the great methodologist Linnaeus (1707-1778), one of whose treatises was entitled Genera morborum. At the beginning of the 19th century, the classification of disease in most general use was one by William Cullen (1710-1790), of Edinburgh, which was published in 1785 under the title Synopsis nosologiae methodicae. For all practical purposes, however, the statistical study of disease began a century earlier with the work of John Graunt on the London Bills of Mortality. The kind of classification envisaged by this pioneer is exemplified by his attempt to estimate the proportion of liveborn children who died before reaching the age of six years, no records of age at death being available. He took all deaths classed as thrush, convulsions, rickets, teeth and worms, abortives, chrysomes, infants, livergrown, and overlaid and added to them half the deaths classed as smallpox, swinepox, measles, and worms without convulsions. Despite the crudity of this classification his estimate of a 36 % mortality before the age of six years appears from later evidence to have been a good one. While three centuries have contributed something to the scientific accuracy of disease classification, there are many who doubt the usefulness of attempts to compile statistics of disease, or even causes of death, because of the difficulties of classification. -

Diseases/Symptoms Reported to Be Associated with Lyme Disease
Diseases/Symptoms Reported to be Associated with Lyme Disease Abdominal pseudo-eventration Abdominal wall weakness Acrodermatitis chronica atrophicans (ACA) Acute Acral Ischemia Acute conduction disorders Acute coronary syndrome Acute exogenous psychosis Acute febrile illness Acute hemiparesis Acute ischaemic pontine stroke Acute meningitis Acute myelo-meningo-radiculitis Acute myelitis Acute pediatric monoarticular arthritis Acute peripheral facial palsy Acute perimyocarditis Acute posterior multifocal placoid pigment epitheliopathy (APMPPE) Acute pyogenic arthritis Acute reversible diffuse conduction system disease Acute septic arthritis Acute severe encephalitis Acute transitory auriculoventricular block Acute transverse myelitis Acute urinary retention Acquired Immune Deficiency Syndrome (AIDS) Algodystrophy Allergic conditions Allergic conjunctivitis Alopecia Alzheimer’s Disease Amyotrophic lateral sclerosis (ALS - Lou Gehrig's Disease) Amyotrophy Anamnesis Anetoderma Anorexia nervosa Anterior optic neuropathy Antepartum fever Anxiety Arrhythmia Arthralgia Arthritis Asymmetrical hearing loss Ataxic sensory neuropathy Atraumatic spontaneous hemarthrosis Atrioventricular block Attention Deficit Disorder (ADD) Attention Deficit Hyperactivity Disorder (ADHD) Back pain without radiculitis Bannwarth’s Syndrome Behcet's disease Bell’s Palsy Benign cutaneous lymphocytoma Benign lymphocytic infiltration (Jessner-Kanof) Bilateral acute confluent disseminated choroiditis Bilateral carpal tunnel syndrome Bilateral facial nerve palsy Bilateral -

A Brief Evaluation and Image Formation of Pediatrics Nutritional Forum in Opinion Sector Disouja Wills* Nutritonal Sciences, Christian Universita Degli Studo, Italy
d Pediatr Wills, Matern Pediatr Nutr 2016, 2:2 an ic l N a u n t DOI: 10.4172/2472-1182.1000113 r r e i t t i o Maternal and Pediatric a n M ISSN: 2472-1182 Nutrition ShortResearch Commentary Article OpenOpen Access Access A Brief Evaluation and Image formation of Pediatrics Nutritional Forum in Opinion Sector Disouja Wills* Nutritonal Sciences, Christian Universita degli studo, Italy Abstract Severe most and one of the main global threat is Nutritional disorders to backward countries, with respect to this issue WHO involved and trying to overcome this issue with the Co-ordination of INF and BNF. International Nutrition Foundation and British Nutrition Foundation, development in weight gain through proper nutrition and proper immune mechanism in the kids is their main role to eradicate and overcome nutritional problems in world. Keywords: INF; BNF; Malnutrition; Merasmus; Rickets; Weight loss; Precautions to Avoid Nutrition Deficiency in Paediatric health issue Paediatrics Introduction Respective disease having respective deficiency dis order but in the case of nutritional diseases. Proper nutrition is the only thing to cure In the mankind a respective one health and weight gain is fully nutritional disorders. Providing sufficient diet like fish, meat, egg, milk based on perfect nutritional intake which he is having daily, poor diet to malnourished kids and consuming beef, fish liver oil, sheep meat, will show the improper impact and injury to the some of the systems boiled eggs from the age of 3 itself (Tables 1 and 2). in the body, total health also in some times. Blindness, Scurvy, Rickets will be caused by nutritional deficiency disorders only, mainly in kids. -

ICD-10-CM TABULAR LIST of DISEASES and INJURIES 2018 Addenda No Change Chapter 1 No Change Certain Infectious and Parasitic Diseases (A00-B99)
ICD-10-CM TABULAR LIST of DISEASES and INJURIES 2018 Addenda No Change Chapter 1 No Change Certain infectious and parasitic diseases (A00-B99) No Change Intestinal infectious diseases (A00-A09) No Change A04 Other bacterial intestinal infections No Change A04.7 Enterocolitis due to Clostridium difficile Add A04.71 Enterocolitis due to Clostridium difficile, recurrent Add A04.72 Enterocolitis due to Clostridium difficile, not specified as recurrent No Change A05 Other bacterial foodborne intoxications, not elsewhere classified No Change Excludes1: Revise from Clostridium difficile foodborne intoxication and infection (A04.7) Revise to Clostridium difficile foodborne intoxication and infection (A04.7-) No Change Helminthiases (B65-B83) No Change B81 Other intestinal helminthiases, not elsewhere classified No Change Excludes1: Revise from angiostrongyliasis due to Parastrongylus cantonensis (B83.2) Revise to angiostrongyliasis due to: Add Angiostrongylus cantonensis (B83.2) Add Parastrongylus cantonensis (B83.2) No Change B81.3 Intestinal angiostrongyliasis Revise from Angiostrongyliasis due to Parastrongylus costaricensis Revise to Angiostrongyliasis due to: Add Angiostrongylus costaricensis Add Parastrongylus costaricensis No Change Chapter 2 No Change Neoplasms (C00-D49) No Change Malignant neoplasms of ill-defined, other secondary and unspecified sites (C76-C80) No Change C79 Secondary malignant neoplasm of other and unspecified sites Delete Excludes2: lymph node metastases (C77.0) No Change C79.1 Secondary malignant neoplasm of bladder -

Preventable Diseases Nick Wilson, Michael G Baker Abstract New Zealanders Can Now Reflect on and Celebrate 50 Years of Polio Elimination in This Country
THE NEW ZEALAND MEDICAL JOURNAL Journal of the New Zealand Medical Association Celebrating 50 years of polio elimination in New Zealand: but inadequate progress in eliminating other vaccine- preventable diseases Nick Wilson, Michael G Baker Abstract New Zealanders can now reflect on and celebrate 50 years of polio elimination in this country. This success was followed by eliminating two other infectious diseases, brucellosis and hydatids, and an imported potential disease vector, the southern saltmarsh mosquito. However, this country has made inadequate progress in eliminating several other vaccine-preventable diseases. These include measles, mumps, and rubella, which are priority candidates for elimination, and potentially Hib disease and rotavirus infection. To achieve such successes almost certainly requires that the country: (i) builds national leadership for elimination goals; (ii) develops detailed plans; (iii) continues recent successes in enhancing routine vaccination coverage; (iv) introduces rotavirus vaccine into the childhood immunisation schedule; and (v) strengthens surveillance and research (on such questions as the cost-effectiveness of new vaccines, measures to enhance uptake, and effective border controls to reduce the risk of disease importation). For 50 years now (since 1 April 1962), New Zealand has been free of transmission of wild-type polio virus infection. The end of this disease was particularly sudden with cases declining from 214 notifications in an outbreak in 1961 (with seven deaths) to only five cases in early 1962. 1 The end coincided with mass immunisation campaigns with the new Sabin (oral) vaccine in 1961 and 1962. The coverage in the vaccination campaign running from April to June 1962 was approximately 95% of the child population up to school leaving age. -
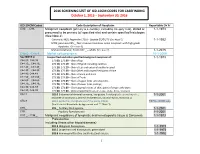
2016 SCREENING LIST of ICD-10CM CODES for CASEFINDING October 1, 2015 – September 30, 2016
2016 SCREENING LIST OF ICD-10CM CODES FOR CASEFINDING October 1, 2015 – September 30, 2016 ICD-10-CM Codes Code Description of Neoplasm Reportable Dx Yr C00._- C96._ Malignant neoplasm (primary & secondary; excluding category C44), stated or 1-1-1973 presumed to be primary (of specified site) and certain specified histologies (See Note 2) Carcinoid, NOS; Appendix C18.0 - Update 01/01/15 (See Note 5) 1-1-1992 MCN; pancreas C25._; Non-invasive mucinous cystic neoplasm with high grade dysplasia. (See note 6) Mature teratoma; Testis C62._ – adults (See note 7) 1-1-2015 C4a.0_-C4a.9_ Merkel cell carcinoma 10-1-2009 See NOTE 4 Unspecified and other specified malignant neoplasm of : 1-1-1973 C44.00.-C44.09 173.00, 173.09 – Skin of Lip C44.10_, C44.19_ 173.10, 173.19 – Skin of Eyelid including canthus C44.20_, C44.29_ 173. 20, 173.29 – Skin of Ear and external auditory canal C44.30_, C44.39_ 173.30, 173.39 – Skin Other and unspecified parts of face C44.40, C44.49 173. 40, 173.49 – Skin of Scalp and neck C44.50_, C44.59_ 173.50, 173.59 – Skin of Trunk C44.60_, C44.69_ 173. 60, 173.69 – Skin of Upper limb and shoulder, C44.70_, C44.79_ 173.70, 173.79 – Skin of Lower limb and hip; C44.80, C44.89 173.80, 173.89 – Overlapping lesions of skin, point of origin unknown; C44.90, C44.99 173.90, 173.99 - Sites unspecified (excludes Labia, Vulva, Penis, Scrotum) C54.1 182.0 Endometrial stromal sarcoma, low grade; Endolymphatic stromal myosis ; 1-1-2001 Endometrial stromatosis, Stromal endometriosis, Stromal myosis, NOS (C54.1) C56.9 183.0 Borderline malignancies -

Eye Disease 1 Eye Disease
Eye disease 1 Eye disease Eye disease Classification and external resources [1] MeSH D005128 This is a partial list of human eye diseases and disorders. The World Health Organisation publishes a classification of known diseases and injuries called the International Statistical Classification of Diseases and Related Health Problems or ICD-10. This list uses that classification. H00-H59 Diseases of the eye and adnexa H00-H06 Disorders of eyelid, lacrimal system and orbit • (H00.0) Hordeolum ("stye" or "sty") — a bacterial infection of sebaceous glands of eyelashes • (H00.1) Chalazion — a cyst in the eyelid (usually upper eyelid) • (H01.0) Blepharitis — inflammation of eyelids and eyelashes; characterized by white flaky skin near the eyelashes • (H02.0) Entropion and trichiasis • (H02.1) Ectropion • (H02.2) Lagophthalmos • (H02.3) Blepharochalasis • (H02.4) Ptosis • (H02.6) Xanthelasma of eyelid • (H03.0*) Parasitic infestation of eyelid in diseases classified elsewhere • Dermatitis of eyelid due to Demodex species ( B88.0+ ) • Parasitic infestation of eyelid in: • leishmaniasis ( B55.-+ ) • loiasis ( B74.3+ ) • onchocerciasis ( B73+ ) • phthiriasis ( B85.3+ ) • (H03.1*) Involvement of eyelid in other infectious diseases classified elsewhere • Involvement of eyelid in: • herpesviral (herpes simplex) infection ( B00.5+ ) • leprosy ( A30.-+ ) • molluscum contagiosum ( B08.1+ ) • tuberculosis ( A18.4+ ) • yaws ( A66.-+ ) • zoster ( B02.3+ ) • (H03.8*) Involvement of eyelid in other diseases classified elsewhere • Involvement of eyelid in impetigo -

Scientific and Medical Aspects of Apheresis: Issues and Evidence 3 ● Scientific and Medical Aspects of Apheresis: Issues and Evidence
3 Scientific and Medical Aspects of Apheresis: Issues and Evidence 3 ● Scientific and Medical Aspects of Apheresis: Issues and Evidence Various types of apheresis procedures have paucity of high-quality research, conclusions been performed on a clinical basis for many years, about the safety, efficacy, and effectiveness of but the number of patients and types of diseases apheresis are necessarily limited, although some treated have risen significantly in the last 5 years. tentative conclusions and directions for treatment This increase is partially due to increased under- can be discerned. standing of the disease and partially due to engi- The present chapter analyzes the methodolog- neering advances in equipment technologies. By ical problems in conducting apheresis research and almost any standard, treatment by apheresis is still examines available evidence of the safety, ef- in relatively early stages of development—there ficacy, and effectiveness of apheresis. Following are no ideal protocols based on a thorough un- a discussion of methodological issues, several derstanding of reasons for its efficacy. Never- major reviews of apheresis research will be sum- theless, there is an increasing flow of clinical data, marized and evaluated. This chapter will further sometimes describing dramatic patient improve- include the findings of a primary literature review ment, supporting the view that apheresis is a and assessment of apheresis in the treatment of rapidly emerging technology with significant three diseases—namely, hemolytic uremic syn- promise (117). Such evidence of treatment effec- drome, acquired Factor-VIII inhibitor, and Guil- tiveness’ is even today, however, often based on lain-Barré syndrome— where preliminary reports unsystematically collected data. -

In the Prevention of Occupational Diseases 94 7.1 Introduction
Report on the current situation in relation to occupational diseases' systems in EU Member States and EFTA/EEA countries, in particular relative to Commission Recommendation 2003/670/EC concerning the European Schedule of Occupational Diseases and gathering of data on relevant related aspects ‘Report on the current situation in relation to occupational diseases’ systems in EU Member States and EFTA/EEA countries, in particular relative to Commission Recommendation 2003/670/EC concerning the European Schedule of Occupational Diseases and gathering of data on relevant related aspects’ Table of Contents 1 Introduction 4 1.1 Foreword .................................................................................................... 4 1.2 The burden of occupational diseases ......................................................... 4 1.3 Recommendation 2003/670/EC .................................................................. 6 1.4 The EU context .......................................................................................... 9 1.5 Information notices on occupational diseases, a guide to diagnosis .................................................................................................. 11 1.6 Objectives of the project ........................................................................... 11 1.7 Methodology and sources ........................................................................ 12 1.8 Structure of the report .............................................................................. 15 2 Developments -

Coxiella Burnetii, the Agent of Q Fever in Brazil
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 107(5): 695-697, August 2012 695 Coxiella burnetii, the agent of Q fever in Brazil: its hidden role in seronegative arthritis and the importance of molecular diagnosis based on the repetitive element IS1111 associated with the transposase gene Tatiana Rozental1/+, Luis Filipe Mascarenhas2, Ronaldo Rozenbaum2,3, Raphael Gomes1, Grasiely Souza Mattos1, Cecília Carlos Magno4, Daniele Nunes Almeida1, Maria Inês Doria Rossi1, Alexsandra RM Favacho1, Elba Regina Sampaio de Lemos1 1Laboratório de Hantaviroses e Rickettsioses, Instituto Oswaldo Cruz-Fiocruz, Rio de Janeiro, RJ, Brasil 2Hospital Servidores do Estado, Rio de Janeiro, RJ, Brasil 3Hospital Samaritano, Rio de Janeiro, RJ, Brasil 4Hospital Copa-D’Or, Rio de Janeiro, RJ, Brasil Coxiella burnetii is the agent of Q fever, an emergent worldwide zoonosis of wide clinical spectrum. Although C. burnetii infection is typically associated with acute infection, atypical pneumonia and flu-like symptoms, endo- carditis, osteoarticular manifestations and severe disease are possible, especially when the patient has a suppressed immune system; however, these severe complications are typically neglected. This study reports the sequencing of the repetitive element IS1111 of the transposase gene of C. burnetii from blood and bronchoalveolar lavage (BAL) samples from a patient with severe pneumonia following methotrexate therapy, resulting in the molecular diagnosis of Q fever in a patient who had been diagnosed with active seronegative polyarthritis two years earlier. To the best of our knowledge, this represents the first documented case of the isolation of C. burnetii DNA from a BAL sample. Key words: Q fever - bronchoalveolar lavage - molecular analysis - seronegative polyarthritis - methotrexate Q fever is caused by Coxiella burnetii, a small obli- patients present symptoms of Q fever fatigue syndrome gate intracellular Gram-negative bacterium of the order (QFS), characterised by headache, joint and muscle pain Legionellales (Stein et al. -
Level I Syllabus
LEVEL I SYLLABUS 1 ACDT Course Learning Objectives Upon Completion, Those Enrolled Will Be MODULE Prepared To... The Language of Dermatology 1. Define and spell the following cutaneous lesions/descriptors: a. Macule b. Patch c. Papule d. Nodule e. Cyst f. Plaque g. Wheal h. Vesicle i. Bulla j. Pustule k. Erosion l. Ulcer m. Atrophy n. Scaling o. Crusting p. Excoriations q. Fissures r. Lichenification s. Erythematous t. Violaceous u. Purpuric v. Hypo/Hyperpigmented w. Linear x. Annular y. Nummular/Discoid z. Blaschkoid aa. Morbilliform bb. Polycyclic cc. Arcuate dd. Reticular Collecting & Documenting Patient History Part I 1. Describe the importance of documentation and chart review, while properly collecting dermatologyspecific medical history components, including: a. Chief Complaint b. Past Medical History c. Family History d. Medications e. Allergies Collecting & Documenting Patient History Part II 1. Demonstrate the proper collection of dermatologyspecific medical history and explain the significance of the following: a. Social History b. Review of Systems c. History of Present Illness Anatomy 1. Spell and document the following directional indicators while applying them to the appropriate anatomical landmarks: a. Proximal/Distal b. Superior/Mid/Inferior c. Anterior/Posterior d. Medial/Lateral e. Dorsal/Ventral 2. Spell and identify specific anatomical locations involving the: a. Scalp b. Forehead c. Ears d. Eyes e. Nose f. Cheeks g. Lips h. Chin i. Neck j. Back k. Upper extremity l. Hands m. Nails n. Chest o. Abdomen p. Buttocks q. Hips r. Lower extremity s. Feet Skin Structure and Function 1. Identify and spell the three primary layers of skin: a.