Populated Printable COP Without TBD Partners
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
![Botswana. Delimitation Commission. [Report Of] Delimitation Commission 1972](https://docslib.b-cdn.net/cover/5626/botswana-delimitation-commission-report-of-delimitation-commission-1972-45626.webp)
Botswana. Delimitation Commission. [Report Of] Delimitation Commission 1972
Botswana. Delimitation Commission. [Report of] Delimitation Commission 1972. Gaborone, Government Pointer [1972?] 16p. 3 fold, maps in pocket at end. 29icm. 1. Botswana-Boundaries, Internal. DELIMITATION COMMISSION 1972 His Excellency Sir Seretse Khama, K.B.E., President of the Republic of Botswana. Your Excellency, We, the undersigned, having been appointed by the Judicial Service Commission to hold a Delimitation Commission under the provisions of Section 65 (1) of the Botswana Constitution, and such appointment having been published in the Government Notice No. 292 of 1972 on the Thirteenth Day of October, 1972 have the honour to inform Your Excellency that we have carried out the said Commission and we append hereto our. Report. (Sir Peter Watkin Williams) Chairman. ,(Rev. A.G. Kgasa) (Father B. Setlalekgosi) Member. Member. (M.J. Pilane) (S.T. Khama) Member. Member. GABORONE, Botswana. The'1st Day of November, 1972. REPORT OF THE DELIMITATION COMMISSION 1972 ~ « .. 1 th ye ar 19 4 cl,mitation - - ? ® L ® ^'p 'Commission was appointed under the provisions of Section 3 of the Bechuanaland (Electoral Provisions) Order-ln-Council of 1964 and this Commission . then proceeded to;divide the country up into thirty-one Constituencies. This Commission was enjoined, as we, ourselves, are similarly enjoined, to base the delimitation of the Constituencies primarily on the number of inhabitants of the. country, but also taking account of natural community of interst, means of communication, geographical features, the density of population and the boundaries of tribal territories and administrative districts. This Commission created thirty-one Constituencies with populations all of which were reasonably cWe to the population quote, that is to say the total population of the country divided by the number of constituencies; the greatest variation being only 18.7% This is assuming that the Census which had taken place shortly before the Commission sat had arrived at a reasonably accurate assessment of the population in each district. -

Environmental Hydrogeology of Lobatse South East District, Republic of Botswana
Bundesanstalt für Geowissenschaften und Rohstoffe Geozentrum Hannover, Germany Environmental Hydrogeology of Lobatse South East District, Republic of Botswana by Katharina Beger, June 2001 Edited by Dr. H. Vogel Table of contents 1. Abstract.............................................................................................................................1 2. Acknowledgements ...........................................................................................................1 3. Introduction ......................................................................................................................2 3.1.1. Project objectives .............................................................................................2 3.1.2. Background......................................................................................................2 4. Geography and geology of the project area .....................................................................4 4.1.1. Geography .......................................................................................................4 4.1.1.1. Location ....................................................................................................5 4.1.1.2. Morphology ...............................................................................................5 4.1.1.3. Climate ......................................................................................................5 4.1.1.4. Settlement, infrastructure and land use .......................................................6 -

LIST of LAW FIRMS NAME of FIRM ADDRESS TEL # FAX # Ajayi Legal
THE LAW SOCIETY OF BOTSWANA - LIST OF LAW FIRMS NAME OF FIRM ADDRESS TEL # FAX # Ajayi Legal Chambers P.O.Box 228, Sebele 3111321 Ajayi Legal Chambers P.O.Box 10220, Selebi Phikwe 2622441 2622442 Ajayi Legal Chambers P.O.Box 449, Letlhakane 2976784 2976785 Akheel Jinabhai & Associates P.O.Box 20575, Gaborone 3906636/3903906 3906642 Akoonyatse Law Firm P.O. Box 25058, Gaborone 3937360 3937350 Antonio & Partners Legal Practice P.O.Box HA 16 HAK, Maun 6864475 6864475 Armstrong Attorneys P.O.Box 1368, Gaborone 3953481 3952757 Badasu & Associates P.O.Box 80274, Gaborone 3700297 3700297 Banyatsi Mmekwa Attorneys P.O.Box 2278 ADD Poso House, Gaborone 3906450/2 3906449 Baoleki Attorneys P.O.Box 45111 Riverwalk, Gaborone 3924775 3924779 Bayford & Botha Attorneys P.O.Box 390, Lobatse 5301369 5301370 B. Maripe & Company P.O.Box 1425, Gaborone 3903258 3181719 B.K.Mmolawa Attorneys P.O.Box 30750, Francistown 2415944 2415943 Bayford & Associates P.O.Box 202283, Gaborone 3956877 3956886 Begane & Associates P.O. Box 60230, Gaborone 3191078 Benito Acolatse Attorneys P.O.Box 1157, Gaborone 3956454 3956447 Bernard Bolele Attorneys P.O.Box 47048, Gaborone 3959111 3951636 Biki & Associates P.O.Box AD 137ABE, Gaborone 3952559 Bogopa Manewe & Tobedza Attorneys P.O.Box 26465, Gaborone 3905466 3905451 Bonner Attorneys Bookbinder Business Law P/Bag 382, Gaborone 3912397 3912395 Briscoe Attorneys P.O.Box 402492, Gaborone 3953377 3904809 Britz Attorneys 3957524 3957062 Callender Attorneys P.O.Box 1354, Francistown 2441418 2446886 Charles Tlagae Attorneys P.O.Box -

Botswana Environment Statistics Water Digest 2018
Botswana Environment Statistics Water Digest 2018 Private Bag 0024 Gaborone TOLL FREE NUMBER: 0800600200 Tel: ( +267) 367 1300 Fax: ( +267) 395 2201 E-mail: [email protected] Website: http://www.statsbots.org.bw Published by STATISTICS BOTSWANA Private Bag 0024, Gaborone Phone: 3671300 Fax: 3952201 Email: [email protected] Website: www.statsbots.org.bw Contact Unit: Environment Statistics Unit Phone: 367 1300 ISBN: 978-99968-482-3-0 (e-book) Copyright © Statistics Botswana 2020 No part of this information shall be reproduced, stored in a Retrieval system, or even transmitted in any form or by any means, whether electronically, mechanically, photocopying or otherwise, without the prior permission of Statistics Botswana. BOTSWANA ENVIRONMENT STATISTICS WATER DIGEST 2018 Statistics Botswana PREFACE This is Statistics Botswana’s annual Botswana Environment Statistics: Water Digest. It is the first solely water statistics annual digest. This Digest will provide data for use by decision-makers in water management and development and provide tools for the monitoring of trends in water statistics. The indicators in this report cover data on dam levels, water production, billed water consumption, non-revenue water, and water supplied to mines. It is envisaged that coverage of indicators will be expanded as more data becomes available. International standards and guidelines were followed in the compilation of this report. The United Nations Framework for the Development of Environment Statistics (UNFDES) and the United Nations International Recommendations for Water Statistics were particularly useful guidelines. The data collected herein will feed into the UN System of Environmental Economic Accounting (SEEA) for water and hence facilitate an informed management of water resources. -
Questions 1. Mr. Dl Keorapetse
BOTSWANA NATIONAL ASSEMBLY O R D E R P A P E R (WEDNESDAY 3RD FEBRUARY, 2016) QUESTIONS 1. MR. D. L. KEORAPETSE, MP. (SELEBI PHIKWE WEST): To ask the (187) Minister of Minerals, Energy and Water Resources:- (i) how often electricity and water meters should be serviced; (ii) whether Botswana Power Corporation (BPC) and Water Utilities Corporation (WUC) allow consumers to service electricity and water meters themselves; if not, (iii) how often BPC and WUC service the said meters; and (iv) who, in the absence of electricity and water regulators, independently receives and investigates consumer complaints about malfunctioning and/or suspect electricity and water meters. 2. MR. N. M. NGAKA, MP. (TAKATOKWANE): To ask the Minister of (188) Health if she is aware that Motokwe, Khekhenye and Tsetseng Health Posts are not in either Kgalagadi or Kweneng Districts’ staff houses building lists; if so:- (i) why and which of the two lists are they supposed to be in; (ii) how many houses are the three (3) health posts mentioned above allocated; and (iii) whether this omission is not a sign that the three (3) health posts should be serviced by Kweneng and not Kgalagadi as it was the case before. 3. MR. A. S. KESUPILE, MP. (KANYE SOUTH): To ask the Minister of (189) Agriculture:- (i) if he is aware that Lobutse is a well organised community that needs regular visits by the agriculture officer to advise on a host of issues regarding the use of their fields and to resolve with their involvement the long standing issue of a drift fence; if so, (ii) to explain why the agriculture officers are not regular enough to the satisfaction of the farmers; and (iii) when Lobutse community will be assisted to put up the drift fence. -

Populated Printable COP 2009 Botswana Generated 9/28/2009 12:01:26 AM
Populated Printable COP 2009 Botswana Generated 9/28/2009 12:01:26 AM ***pages: 415*** Botswana Page 1 Table 1: Overview Executive Summary None uploaded. Country Program Strategic Overview Will you be submitting changes to your country's 5-Year Strategy this year? If so, please briefly describe the changes you will be submitting. X Yes No Description: test Ambassador Letter File Name Content Type Date Uploaded Description Uploaded By Letter from Ambassador application/pdf 11/14/2008 TSukalac Nolan.pdf Country Contacts Contact Type First Name Last Name Title Email PEPFAR Coordinator Thierry Roels Associate Director GAP-Botswana [email protected] DOD In-Country Contact Chris Wyatt Chief, Office of Security [email protected] Cooperation HHS/CDC In-Country Contact Thierry Roels Associate Director GAP-Botswana [email protected] Peace Corps In-Country Peggy McClure Director [email protected] Contact USAID In-Country Contact Joan LaRosa USAID Director [email protected] U.S. Embassy In-Country Phillip Druin DCM [email protected] Contact Global Fund In-Country Batho C Molomo Coordinator of NACA [email protected] Representative Global Fund What is the planned funding for Global Fund Technical Assistance in FY 2009? $0 Does the USG assist GFATM proposal writing? Yes Does the USG participate on the CCM? Yes Generated 9/28/2009 12:01:26 AM ***pages: 415*** Botswana Page 2 Table 2: Prevention, Care, and Treatment Targets 2.1 Targets for Reporting Period Ending September 30, 2009 National 2-7-10 USG USG Upstream USG Total Target Downstream (Indirect) -
List of Examination Centres by Region Bobirwa Region Centr Name Addres Place Phone 0101 Bobonong Primary School P.O
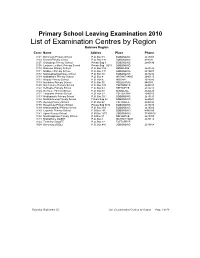
Primary School Leaving Examination 2010 List of Examination Centres by Region Bobirwa Region Centr Name Addres Place Phone 0101 Bobonong Primary School P.O. Box 48 BOBONONG 2619207 0103 Borotsi Primary School P.O. Box 136 BOBONONG 819208 0107 Gobojango Primary School Private Bag 8 BOBONONG 2645436 0108 Lentswe-Le-Moriti Primary School Private Bag 0019 BOBONONG 0110 Mabolwe Primary School P.O. Box 182 SEMOLALE 2645422 0111 Madikwe Primary School P.O. Box 131 BOBONONG 2619221 0112 Mafetsakgang primary school P.O. Box 46 BOBONONG 2619232 0114 Mathathane Primary School P.O. Box 4 MATHATHANE 2645110 0117 Mogapi Primary School P.O. Box 6 MOGAPI 2618545 0119 Molalatau Primary School P.O. Box 50 MOLALATAU 845374 0120 Moletemane Primary School P.O. Box 176 TSETSEBYE 2646035 0123 Sefhophe Primary School P.O. Box 41 SEFHOPHE 2618210 0124 Semolale Primary School P.O. Box 10 SEMOLALE 2645422 0131 Tsetsejwe Primary School P.O. Box 33 TSETSEJWE 2646103 0133 Modisaotsile Primary School P.O. Box 591 BOBONONG 2619123 0134 Motlhabaneng Primary School Private Bag 20 BOBONONG 2645541 0135 Busang Primary School P.O. Box 47 TSETSEBJE 2646144 0138 Rasetimela Primary School Private Bag 0014 BOBONONG 2619485 0139 Mabumahibidu Primary School P.O. Box 168 BOBONONG 2619040 0140 Lepokole Primary School P O Box 148 BOBONONG 4900035 0141 Agosi Primary School P O Box 1673 BOBONONG 71868614 0142 Motsholapheko Primary School P O Box 37 SEFHOPHE 2618305 0143 Mathathane DOSET P.O. Box 4 MATHATHANE 2645110 0144 Tsetsebye DOSET P.O. Box 33 TSETSEBYE 3024 Bobonong DOSET P.O. Box 483 BOBONONG 2619164 Saturday, September 25, List of Examination Centres by Region Page 1 of 39 Boteti Region Centr Name Addres Place Phone 0201 Adult Education Private Bag 1 ORAPA 0202 Baipidi Primary School P.O. -

2017 SEAT Report Orapa, Letlhakane and Damtshaa Mines
SEAT 3 REPORT Debswana - Orapa, Letlhakane and Damtshaa Mine (OLDM) November 2017 1 2 FOREWORD rounded assessment of the socio-economic impacts of our operation – positive and negative - in our zone of influence. This is the second impact assessment of this nature being conducted, the first one having been carried out in 2014. The information in this socio-economic assessment report helped to improve our understanding of the local dynamics associated with the impact our operation’s that are real and perceived. It also provided us with invaluable insight into our stakeholders’ perspectives, expectations, concerns and suggestions. This report is a valuable tool to guide our thinking on community development and our management of the social impacts of OLDM’s future closure at the end of the life of mine. Furthermore, it provides a useful mechanism in mobilising local stakeholders to work with us towards successful mine closure. The report has also given valuable feedback on issues around mine expansion initiatives and access to resources like land and groundwater. More importantly, meaningful feedback has been provided around two critical areas: resettlement and options around town transformation. We recognise the complexity of a proper plan for future mine closure at the end of the life of mine. In the past, our plans for future mine closure mainly focused on environmental aspects, with community involvement often limited to cursory consultation processes. Today, in line with current trends, my team and I are convinced that community ownership of the post closure goals is the only sustainable means to propel communities to prosper when OLDM is no longer involved. -

Refundable Fee of P280.00 (Two Hundred and Eighty Pula Only) VAT Inclusive
PUBLIC TENDER NOTICE TENDER NO: BOCRA/PT/006/2020.2021 SUPPLY, INSTALLATION AND COMMISSIONING OF ICT EQUIPMENT AT TWELVE (12) TRIBAL ADMINISTRATIONS IN KWENENG DISTRICT The Botswana Communications Regulatory Authority (BOCRA or the Authority) hereby invites experienced and reputable companies to tender for the Supply, Installation and Commissioning of ICT Equipment at twelve (12) Tribal Administrations in Kweneng District. The tender is reserved for 100% citizen-owned companies who are registered with the Public Procurement and Asset Disposal Board (PPADB) under the following codes and subcodes; Code 203: Electrical, Electronic, Mechanical and ICT Supplies Subcode 01: Electrical and Electronic Equipment, Spares and Accessories (includes ICT, photographic equipment, and others). Youth owned companies in Botswana shall purchase the ITT at 50% of the purchase price as per Presidential Directive CAB 14 (B)/2015. The Invitation to Tender (ITT) document may be purchased at the BOCRA Head Office by interested companies at a non-refundable fee of P280.00 (Two Hundred and Eighty Pula Only) VAT inclusive. Payment must be made in the form of bank transfer or deposits to the following bank details: Bank Name: First National Bank Botswana Ltd Branch Name: Mall Branch Code: 28-28-67 Account Name: Botswana Communications Regulatory Authority Bank Account No: 62011115088 Swift Code: FIRNBWGX Reference: BTA0001 Tender documents shall be issued upon provision of Proof of Payment (POP). All funds transfer bank charges shall be borne by the bidder. Compulsory -

Botswana Country Report-Annex-4 4Th Interim Techical Report
PROMOTING PARTNERSHIPS FOR CRIMEPREVENTION BETWEEN THE STATE AND PRIVATE SECURITY PROVIDERS IN BOTSWANA BY MPHO MOLOMO AND ZIBANI MAUNDENI Introduction Botswana stands out as the only African country to have sustained an unbroken record of liberal democracy and political stability since independence. The country has been dubbed the ‘African Miracle’ (Thumberg Hartland, 1978; Samatar, 1999). It is widely regarded as a success story arising from its exploitation and utilisation of natural resources, establishing a strong state, institutional and administrative capacity, prudent macro-economic stability and strong political leadership. These attributes, together with the careful blending of traditional and modern institutions have afforded Botswana a rare opportunity of political stability in the Africa region characterised by political and social strife. The expectation is that the economic growth will bring about development and security. However, a critical analysis of Botswana’s development trajectory indicates that the country’s prosperity has it attendant problems of poverty, unemployment, inequalities and crime. Historically crime prevention was a preserve of the state using state security agencies as the police, military, prisons and other state apparatus, such as, the courts and laws. However, since the late 1980s with the expanded definition of security from the narrow static conception to include human security, it has become apparent that state agencies alone cannot combat the rising levels of crime. The police in recognising that alone they cannot cope with the crime levels have been innovative and embarked on other models of public policing, such as, community policing as a public society partnership to combat crime. To further cater for the huge demand on policing, other actors, which are non-state actors; in particular private security firms have come in, especially in the urban market and occupy a special niche to provide a service to those who can afford to pay for it. -

Land Tenure Reforms and Social Transformation in Botswana: Implications for Urbanization
Land Tenure Reforms and Social Transformation in Botswana: Implications for Urbanization. Item Type text; Electronic Dissertation Authors Ijagbemi, Bayo, 1963- Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 06/10/2021 17:13:55 Link to Item http://hdl.handle.net/10150/196133 LAND TENURE REFORMS AND SOCIAL TRANSFORMATION IN BOTSWANA: IMPLICATIONS FOR URBANIZATION by Bayo Ijagbemi ____________________ Copyright © Bayo Ijagbemi 2006 A Dissertation Submitted to the Faculty of the DEPARTMENT OF ANTHROPOLOGY In Partial Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY In the Graduate College THE UNIVERSITY OF ARIZONA 2006 2 THE UNIVERSITY OF ARIZONA GRADUATE COLLEGE As members of the Dissertation Committee, we certify that we have read the dissertation prepared by Bayo Ijagbemi entitled “Land Reforms and Social Transformation in Botswana: Implications for Urbanization” and recommend that it be accepted as fulfilling the dissertation requirement for the Degree of Doctor of Philosophy _______________________________________________________________________ Date: 10 November 2006 Dr Thomas Park _______________________________________________________________________ Date: 10 November 2006 Dr Stephen Lansing _______________________________________________________________________ Date: 10 November 2006 Dr David Killick _______________________________________________________________________ Date: 10 November 2006 Dr Mamadou Baro Final approval and acceptance of this dissertation is contingent upon the candidate’s submission of the final copies of the dissertation to the Graduate College. I hereby certify that I have read this dissertation prepared under my direction and recommend that it be accepted as fulfilling the dissertation requirement. -

Department of Road Transport and Safety Offices
DEPARTMENT OF ROAD TRANSPORT AND SAFETY OFFICES AND SERVICES MOLEPOLOLE • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Transport Inspectorate Tel: 5920148 Fax: 5910620 P/Bag 52 Molepolole Next to Molepolole Police MOCHUDI • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Transport Inspectorate P/Bag 36 Mochudi Tel : 5777127 Fax : 5748542 White House GABORONE Headquarters BBS Mall Plot no 53796 Tshomarelo House (Botswana Savings Bank) 1st, 2nd &3rd Floor Corner Lekgarapa/Letswai Road •Registration & Licensing of vehicles and drivers •Road safety (Public Education) Tel: 3688600/62 Fax : Fax: 3904067 P/Bag 0054 Gaborone GABORONE VTS – MARUAPULA • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Vehicle Examination Tel: 3912674/2259 P/Bag BR 318 B/Hurst Near Roads Training & Roads Maintenance behind Maruapula Flats GABORONE II – FAIRGROUNDS • Registration & Licensing of vehicles and drivers • Driver Examination : Theory Tel: 3190214/3911540/3911994 Fax : P/Bag 0054 Gaborone GABORONE - OLD SUPPLIES • Registration & Licensing of vehicles and drivers • Transport Permits • Transport Inspectorate Tel: 3905050 Fax :3932671 P/Bag 0054 Gaborone Plot 1221, Along Nkrumah Road, Near Botswana Power Corporation CHILDREN TRAFFIC SCHOOL •Road Safety Promotion for children only Tel: 3161851 P/Bag BR 318 B/Hurst RAMOTSWA •Registration & Licensing of vehicles and drivers •Driver Examination (Theory & Practical